
Iatrogenic Hyponatremia
Iatrogenic Hyponatremia
You might also like
- Homework 8Document2 pagesHomework 8Kitsum Li0% (1)
- Fluids & Electrolytes ExamDocument13 pagesFluids & Electrolytes ExamJan Macarambon73% (11)
- Iatrogenic HyponatremiaDocument2 pagesIatrogenic Hyponatremiadr Iyan DarmawanNo ratings yet
- Fluid Management of Neurosurgical Patient, Recent Update: Taeha. RyuDocument73 pagesFluid Management of Neurosurgical Patient, Recent Update: Taeha. RyuMada Oktav CakradwipaNo ratings yet
- Liquidos Hipotonocos IV-1 PDFDocument6 pagesLiquidos Hipotonocos IV-1 PDFAdrianRuizNo ratings yet
- 'Ab' Normsal SalineDocument11 pages'Ab' Normsal Salinedrmurad321No ratings yet
- Terapi Cairan Salin AnakDocument5 pagesTerapi Cairan Salin AnakDokter UmumNo ratings yet
- Pi Is 2590059522000863Document4 pagesPi Is 2590059522000863nina2911No ratings yet
- Colloid PDFDocument45 pagesColloid PDFubaidrahamanNo ratings yet
- Cao Et Al 2022 Perioperative Fluid Management in Surgical Patients A ReviewDocument8 pagesCao Et Al 2022 Perioperative Fluid Management in Surgical Patients A Reviewyqxdbkd868No ratings yet
- PN Composition CompilationDocument15 pagesPN Composition CompilationAnonymous rDD9I2No ratings yet
- The Effect of Nacl 0.9% and Nacl 0.45% On Sodium, Chloride, and Acid-Base Balance in A Picu PopulationDocument7 pagesThe Effect of Nacl 0.9% and Nacl 0.45% On Sodium, Chloride, and Acid-Base Balance in A Picu PopulationJoecoNo ratings yet
- Otsuka CairanDocument60 pagesOtsuka Cairan_LipRaa_No ratings yet
- New Trend IV FluidsDocument9 pagesNew Trend IV FluidsMarfu'ah Mar'ahNo ratings yet
- Fluid Student 2012Document43 pagesFluid Student 2012Sara Ilyas KhanNo ratings yet
- Bellomo 2006Document7 pagesBellomo 2006Manal regraguiNo ratings yet
- 061.p159-164 NOTE KAWAHARADocument7 pages061.p159-164 NOTE KAWAHARAallhayokNo ratings yet
- Saline Is The Solution For Crystalloid Resuscitation: Paul Young, MBCHBDocument3 pagesSaline Is The Solution For Crystalloid Resuscitation: Paul Young, MBCHBAnonymous lF3962RA1cNo ratings yet
- 2 PDFDocument6 pages2 PDFLisa HikmawanNo ratings yet
- Demystifying HyponatremiaDocument10 pagesDemystifying HyponatremiaJavier Vivanco100% (1)
- RLEFandECS Garlitos RoanneDocument4 pagesRLEFandECS Garlitos RoannePaul JacksonNo ratings yet
- A Comparison of Sterofundin & RL On Intraoperative Acid Base & Electrolytes Status in Children (ACCM Journal)Document8 pagesA Comparison of Sterofundin & RL On Intraoperative Acid Base & Electrolytes Status in Children (ACCM Journal)TedyJaswadiNo ratings yet
- Lactated RingersDocument3 pagesLactated RingersE100% (5)
- The Effect of Coconut Water (Cocos Nucifera L.) and An Isotonic Drink On The Change of Heart Rate Frequency in The Rats Induced HypertensionDocument4 pagesThe Effect of Coconut Water (Cocos Nucifera L.) and An Isotonic Drink On The Change of Heart Rate Frequency in The Rats Induced HypertensionKaushik MankarNo ratings yet
- Fluid & Electrolytes SaurabhDocument88 pagesFluid & Electrolytes Saurabhunknownsince1986No ratings yet
- Infusion Of. WaterDocument4 pagesInfusion Of. Waternewo dimNo ratings yet
- Diagnosis and Management of Water Intoxication in A Buffalo CalfDocument2 pagesDiagnosis and Management of Water Intoxication in A Buffalo CalfY.rajuNo ratings yet
- 1-Fluid Management in Critically Ill Patients - Update Int Med Feb2018Document46 pages1-Fluid Management in Critically Ill Patients - Update Int Med Feb2018ดนุ เกษรศิริNo ratings yet
- B2 PDFDocument9 pagesB2 PDFDr. Arvind YadavNo ratings yet
- IMBALANCE ofDocument21 pagesIMBALANCE ofapi-19916399No ratings yet
- Fluid Resuscitation: Ringer Lactate Versus Normal Saline-A Clinical StudyDocument4 pagesFluid Resuscitation: Ringer Lactate Versus Normal Saline-A Clinical StudyMirela Marina BlajNo ratings yet
- Fluid ManagementDocument11 pagesFluid ManagementAtzi FNo ratings yet
- LEV IntraoperatoriosDocument11 pagesLEV IntraoperatoriosCasual CasualNo ratings yet
- DR - Nursamsu, SpPD-KGH-Penggunaan Cairan Koloid Pada Kondisi Syok PDFDocument38 pagesDR - Nursamsu, SpPD-KGH-Penggunaan Cairan Koloid Pada Kondisi Syok PDFNONANo ratings yet
- Stoelting 5th Edition - 1Document17 pagesStoelting 5th Edition - 1hariNo ratings yet
- Fluids in Septic Shock: Crystalloid, Colloids, or Blood?: CrystalloidsDocument10 pagesFluids in Septic Shock: Crystalloid, Colloids, or Blood?: CrystalloidsfbihansipNo ratings yet
- Wang Et Al 2018 Electrocardiographic Manifestations in Severe HypokalemiaDocument7 pagesWang Et Al 2018 Electrocardiographic Manifestations in Severe HypokalemiaaisyahhelmadevithalibNo ratings yet
- Effect of Abdominal Trauma On Hemorrhagic Shock-Induced Acute Lung Injury in RatsDocument4 pagesEffect of Abdominal Trauma On Hemorrhagic Shock-Induced Acute Lung Injury in RatsBelajar PintarNo ratings yet
- Smith L (2017) Nursing Times 113: 12, 20-23Document59 pagesSmith L (2017) Nursing Times 113: 12, 20-23Derick RanaNo ratings yet
- Sodium Disorders AAFP PDFDocument12 pagesSodium Disorders AAFP PDFIvan Tintaya UrureNo ratings yet
- Management of Acute Metabolic Acidosis in The ICU Sodium BicarbonateDocument6 pagesManagement of Acute Metabolic Acidosis in The ICU Sodium Bicarbonatecastillojess100% (1)
- Maintenance and Replacement Therapy: Fluids and Electrolytes (Part 2)Document6 pagesMaintenance and Replacement Therapy: Fluids and Electrolytes (Part 2)Maikka IlaganNo ratings yet
- DBDDocument42 pagesDBDAri Evananda Dwi PutraNo ratings yet
- (1479683X - European Journal of Endocrinology) The Syndrome of Inappropriate Antidiuretic Hormone - Current and Future Management OptionsDocument6 pages(1479683X - European Journal of Endocrinology) The Syndrome of Inappropriate Antidiuretic Hormone - Current and Future Management OptionsYulius DonyNo ratings yet
- Neuro4Nurses: Syndrome of Inappropriate Release of Antidiuretic HormoneDocument2 pagesNeuro4Nurses: Syndrome of Inappropriate Release of Antidiuretic HormoneM Zainun IrsyadNo ratings yet
- Smith y Berchtold, 2014 Fluid Therapy in CalvesDocument19 pagesSmith y Berchtold, 2014 Fluid Therapy in Calvestiggerrhk6315No ratings yet
- w5 PDFDocument4 pagesw5 PDFAmber ClarkNo ratings yet
- Fluid and Electrolyte Administration - CPGDocument7 pagesFluid and Electrolyte Administration - CPGhelamahjoubmounirdmoNo ratings yet
- 149779-Article Text-393916-1-10-20170111 PDFDocument4 pages149779-Article Text-393916-1-10-20170111 PDFvisiniNo ratings yet
- The Effect of Dialysis Membrane Flux On Amino Acid Loss in Hemodialysis PatientsDocument6 pagesThe Effect of Dialysis Membrane Flux On Amino Acid Loss in Hemodialysis PatientsmaydamayNo ratings yet
- No Resucitar Con SalinaDocument4 pagesNo Resucitar Con SalinaAntonia Holguin HoyosNo ratings yet
- Journal Reading BPPDocument29 pagesJournal Reading BPPMiftahuljannah SudirmanNo ratings yet
- Jonathan B. Edelson, MD Evan W. Orenstein, MD Lisa B. Zaoutis, MD Lawrence Copelovitch, MDDocument29 pagesJonathan B. Edelson, MD Evan W. Orenstein, MD Lisa B. Zaoutis, MD Lawrence Copelovitch, MDrifkiNo ratings yet
- Hypocalcemia: Julie Allen, BVMS, MS, MRCVS, Dacvim (Saim), DacvpDocument1 pageHypocalcemia: Julie Allen, BVMS, MS, MRCVS, Dacvim (Saim), DacvpElenaNo ratings yet
- Use of Intravenous Fluidssolutions A Narrative ReviewDocument14 pagesUse of Intravenous Fluidssolutions A Narrative Reviewbarbarba obrequeNo ratings yet
- A Physiologic-Based Approach To The Treatment of A Patient With HypokalemiaDocument6 pagesA Physiologic-Based Approach To The Treatment of A Patient With HypokalemiaPablo IgnacioNo ratings yet
- Ex Vivo Heart ProjectDocument41 pagesEx Vivo Heart ProjectKitchanan KosalathipNo ratings yet
- Ionized Alkaline Water New Strategy For ManagementDocument6 pagesIonized Alkaline Water New Strategy For ManagementninoNo ratings yet
- FsfsdfsDocument35 pagesFsfsdfsJonathan wiradinataNo ratings yet
- Case Presentation Station 3B Drug Study Sodium ChlorideDocument4 pagesCase Presentation Station 3B Drug Study Sodium ChloridehahahahaaaaaaaNo ratings yet
- Equine Fluid TherapyFrom EverandEquine Fluid TherapyC. Langdon FieldingNo ratings yet
- Fluid Therapy in Various ConditionsDocument62 pagesFluid Therapy in Various ConditionsAndy F MonroeNo ratings yet
- 01-Guidelines For Use of Hypertonic SalineDocument13 pages01-Guidelines For Use of Hypertonic SalineSatish VeerlaNo ratings yet
- Buffers and Isotonic SolutionsDocument16 pagesBuffers and Isotonic SolutionsGiang PhamNo ratings yet
- Hypertonic SalineDocument3 pagesHypertonic SalineEldimson BermudoNo ratings yet
- Kim 2021Document8 pagesKim 2021Arun AdhikariNo ratings yet
- Fluid Management BurnDocument13 pagesFluid Management BurnWeronika StarrNo ratings yet
- Pharmacy Calculations: Random Problems: Actimed by Generika DrugstoreDocument17 pagesPharmacy Calculations: Random Problems: Actimed by Generika Drugstoreamethyst grandeNo ratings yet
- Parenteral Medication Labels and Dosage CalculationDocument22 pagesParenteral Medication Labels and Dosage CalculationlisaNo ratings yet
- Repeated Up To 3times With 5min Interval, It Causes Hypotension)Document4 pagesRepeated Up To 3times With 5min Interval, It Causes Hypotension)Ebrahim MokhtarNo ratings yet
- PROJECT REPORT ON I.V. FLUID UNIT (Ringer's Lactate, Normal Saline, Dextrose 4.3%, 5%, 10%, 50% & Darrows Solution)Document13 pagesPROJECT REPORT ON I.V. FLUID UNIT (Ringer's Lactate, Normal Saline, Dextrose 4.3%, 5%, 10%, 50% & Darrows Solution)EIRI Board of Consultants and PublishersNo ratings yet
- Different Types of IV FluidsDocument10 pagesDifferent Types of IV FluidsMarinill SolimanNo ratings yet
- Fluid and Electrolyte ImbalancesDocument37 pagesFluid and Electrolyte Imbalancesapi-3797941100% (4)
- The Origin of IV FluidsDocument15 pagesThe Origin of IV Fluidsashley nicholeNo ratings yet
- اسئله جراحه عامه سنوات سابقه امتحان الامتيازDocument110 pagesاسئله جراحه عامه سنوات سابقه امتحان الامتيازZaid Zayed100% (1)
- Blood Transfusion PDFDocument8 pagesBlood Transfusion PDFHasan A AsFour100% (1)
- Parenteral InjectionsDocument42 pagesParenteral InjectionsAngelica AmandoNo ratings yet
- HESI Dosage Calculation Practice ExamDocument24 pagesHESI Dosage Calculation Practice Exambhilligoss35No ratings yet
- 05 - An Evaluation of Tetramethylbenzidine As A Presumptive Test For BloodDocument6 pages05 - An Evaluation of Tetramethylbenzidine As A Presumptive Test For BloodMicawber7No ratings yet
- Surgery-On CallDocument729 pagesSurgery-On CallNadhirah ZulkifliNo ratings yet
- Day 2 QuizDocument2 pagesDay 2 QuizAngie MandeoyaNo ratings yet
- Principles of Fluid Management 2015 PDFDocument17 pagesPrinciples of Fluid Management 2015 PDFJorge DíazNo ratings yet
- Acid-Base Balance Revisited - Stewart and Strong IonsDocument8 pagesAcid-Base Balance Revisited - Stewart and Strong IonsMileidys LopezNo ratings yet
- Drugs Used in EmergencyDocument7 pagesDrugs Used in EmergencyAzza DianNo ratings yet
- Iv-Infusion-Rate-Calculations and Sample QuestionsDocument3 pagesIv-Infusion-Rate-Calculations and Sample QuestionsACanNo ratings yet
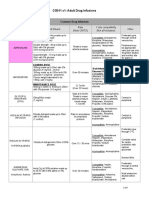
- CG011.v1: Adult Drug Infusions: Drug Dose and Diluent Rate (Note UNITS) Y Site Compatibility (Not All-Inclusive) OtherDocument8 pagesCG011.v1: Adult Drug Infusions: Drug Dose and Diluent Rate (Note UNITS) Y Site Compatibility (Not All-Inclusive) OtheriqbalNo ratings yet
- Medications AdministrationDocument69 pagesMedications AdministrationyuddNo ratings yet
- Exam 2018 PDFDocument62 pagesExam 2018 PDFWondimu Koy100% (2)























































































Download as pdf or txt
You might also like
- Homework 8Document2 pagesHomework 8Kitsum Li0% (1)
- Fluids & Electrolytes ExamDocument13 pagesFluids & Electrolytes ExamJan Macarambon73% (11)
- Iatrogenic HyponatremiaDocument2 pagesIatrogenic Hyponatremiadr Iyan DarmawanNo ratings yet
- Fluid Management of Neurosurgical Patient, Recent Update: Taeha. RyuDocument73 pagesFluid Management of Neurosurgical Patient, Recent Update: Taeha. RyuMada Oktav CakradwipaNo ratings yet
- Liquidos Hipotonocos IV-1 PDFDocument6 pagesLiquidos Hipotonocos IV-1 PDFAdrianRuizNo ratings yet
- 'Ab' Normsal SalineDocument11 pages'Ab' Normsal Salinedrmurad321No ratings yet
- Terapi Cairan Salin AnakDocument5 pagesTerapi Cairan Salin AnakDokter UmumNo ratings yet
- Pi Is 2590059522000863Document4 pagesPi Is 2590059522000863nina2911No ratings yet
- Colloid PDFDocument45 pagesColloid PDFubaidrahamanNo ratings yet
- Cao Et Al 2022 Perioperative Fluid Management in Surgical Patients A ReviewDocument8 pagesCao Et Al 2022 Perioperative Fluid Management in Surgical Patients A Reviewyqxdbkd868No ratings yet
- PN Composition CompilationDocument15 pagesPN Composition CompilationAnonymous rDD9I2No ratings yet
- The Effect of Nacl 0.9% and Nacl 0.45% On Sodium, Chloride, and Acid-Base Balance in A Picu PopulationDocument7 pagesThe Effect of Nacl 0.9% and Nacl 0.45% On Sodium, Chloride, and Acid-Base Balance in A Picu PopulationJoecoNo ratings yet
- Otsuka CairanDocument60 pagesOtsuka Cairan_LipRaa_No ratings yet
- New Trend IV FluidsDocument9 pagesNew Trend IV FluidsMarfu'ah Mar'ahNo ratings yet
- Fluid Student 2012Document43 pagesFluid Student 2012Sara Ilyas KhanNo ratings yet
- Bellomo 2006Document7 pagesBellomo 2006Manal regraguiNo ratings yet
- 061.p159-164 NOTE KAWAHARADocument7 pages061.p159-164 NOTE KAWAHARAallhayokNo ratings yet
- Saline Is The Solution For Crystalloid Resuscitation: Paul Young, MBCHBDocument3 pagesSaline Is The Solution For Crystalloid Resuscitation: Paul Young, MBCHBAnonymous lF3962RA1cNo ratings yet
- 2 PDFDocument6 pages2 PDFLisa HikmawanNo ratings yet
- Demystifying HyponatremiaDocument10 pagesDemystifying HyponatremiaJavier Vivanco100% (1)
- RLEFandECS Garlitos RoanneDocument4 pagesRLEFandECS Garlitos RoannePaul JacksonNo ratings yet
- A Comparison of Sterofundin & RL On Intraoperative Acid Base & Electrolytes Status in Children (ACCM Journal)Document8 pagesA Comparison of Sterofundin & RL On Intraoperative Acid Base & Electrolytes Status in Children (ACCM Journal)TedyJaswadiNo ratings yet
- Lactated RingersDocument3 pagesLactated RingersE100% (5)
- The Effect of Coconut Water (Cocos Nucifera L.) and An Isotonic Drink On The Change of Heart Rate Frequency in The Rats Induced HypertensionDocument4 pagesThe Effect of Coconut Water (Cocos Nucifera L.) and An Isotonic Drink On The Change of Heart Rate Frequency in The Rats Induced HypertensionKaushik MankarNo ratings yet
- Fluid & Electrolytes SaurabhDocument88 pagesFluid & Electrolytes Saurabhunknownsince1986No ratings yet
- Infusion Of. WaterDocument4 pagesInfusion Of. Waternewo dimNo ratings yet
- Diagnosis and Management of Water Intoxication in A Buffalo CalfDocument2 pagesDiagnosis and Management of Water Intoxication in A Buffalo CalfY.rajuNo ratings yet
- 1-Fluid Management in Critically Ill Patients - Update Int Med Feb2018Document46 pages1-Fluid Management in Critically Ill Patients - Update Int Med Feb2018ดนุ เกษรศิริNo ratings yet
- B2 PDFDocument9 pagesB2 PDFDr. Arvind YadavNo ratings yet
- IMBALANCE ofDocument21 pagesIMBALANCE ofapi-19916399No ratings yet
- Fluid Resuscitation: Ringer Lactate Versus Normal Saline-A Clinical StudyDocument4 pagesFluid Resuscitation: Ringer Lactate Versus Normal Saline-A Clinical StudyMirela Marina BlajNo ratings yet
- Fluid ManagementDocument11 pagesFluid ManagementAtzi FNo ratings yet
- LEV IntraoperatoriosDocument11 pagesLEV IntraoperatoriosCasual CasualNo ratings yet
- DR - Nursamsu, SpPD-KGH-Penggunaan Cairan Koloid Pada Kondisi Syok PDFDocument38 pagesDR - Nursamsu, SpPD-KGH-Penggunaan Cairan Koloid Pada Kondisi Syok PDFNONANo ratings yet
- Stoelting 5th Edition - 1Document17 pagesStoelting 5th Edition - 1hariNo ratings yet
- Fluids in Septic Shock: Crystalloid, Colloids, or Blood?: CrystalloidsDocument10 pagesFluids in Septic Shock: Crystalloid, Colloids, or Blood?: CrystalloidsfbihansipNo ratings yet
- Wang Et Al 2018 Electrocardiographic Manifestations in Severe HypokalemiaDocument7 pagesWang Et Al 2018 Electrocardiographic Manifestations in Severe HypokalemiaaisyahhelmadevithalibNo ratings yet
- Effect of Abdominal Trauma On Hemorrhagic Shock-Induced Acute Lung Injury in RatsDocument4 pagesEffect of Abdominal Trauma On Hemorrhagic Shock-Induced Acute Lung Injury in RatsBelajar PintarNo ratings yet
- Smith L (2017) Nursing Times 113: 12, 20-23Document59 pagesSmith L (2017) Nursing Times 113: 12, 20-23Derick RanaNo ratings yet
- Sodium Disorders AAFP PDFDocument12 pagesSodium Disorders AAFP PDFIvan Tintaya UrureNo ratings yet
- Management of Acute Metabolic Acidosis in The ICU Sodium BicarbonateDocument6 pagesManagement of Acute Metabolic Acidosis in The ICU Sodium Bicarbonatecastillojess100% (1)
- Maintenance and Replacement Therapy: Fluids and Electrolytes (Part 2)Document6 pagesMaintenance and Replacement Therapy: Fluids and Electrolytes (Part 2)Maikka IlaganNo ratings yet
- DBDDocument42 pagesDBDAri Evananda Dwi PutraNo ratings yet
- (1479683X - European Journal of Endocrinology) The Syndrome of Inappropriate Antidiuretic Hormone - Current and Future Management OptionsDocument6 pages(1479683X - European Journal of Endocrinology) The Syndrome of Inappropriate Antidiuretic Hormone - Current and Future Management OptionsYulius DonyNo ratings yet
- Neuro4Nurses: Syndrome of Inappropriate Release of Antidiuretic HormoneDocument2 pagesNeuro4Nurses: Syndrome of Inappropriate Release of Antidiuretic HormoneM Zainun IrsyadNo ratings yet
- Smith y Berchtold, 2014 Fluid Therapy in CalvesDocument19 pagesSmith y Berchtold, 2014 Fluid Therapy in Calvestiggerrhk6315No ratings yet
- w5 PDFDocument4 pagesw5 PDFAmber ClarkNo ratings yet
- Fluid and Electrolyte Administration - CPGDocument7 pagesFluid and Electrolyte Administration - CPGhelamahjoubmounirdmoNo ratings yet
- 149779-Article Text-393916-1-10-20170111 PDFDocument4 pages149779-Article Text-393916-1-10-20170111 PDFvisiniNo ratings yet
- The Effect of Dialysis Membrane Flux On Amino Acid Loss in Hemodialysis PatientsDocument6 pagesThe Effect of Dialysis Membrane Flux On Amino Acid Loss in Hemodialysis PatientsmaydamayNo ratings yet
- No Resucitar Con SalinaDocument4 pagesNo Resucitar Con SalinaAntonia Holguin HoyosNo ratings yet
- Journal Reading BPPDocument29 pagesJournal Reading BPPMiftahuljannah SudirmanNo ratings yet
- Jonathan B. Edelson, MD Evan W. Orenstein, MD Lisa B. Zaoutis, MD Lawrence Copelovitch, MDDocument29 pagesJonathan B. Edelson, MD Evan W. Orenstein, MD Lisa B. Zaoutis, MD Lawrence Copelovitch, MDrifkiNo ratings yet
- Hypocalcemia: Julie Allen, BVMS, MS, MRCVS, Dacvim (Saim), DacvpDocument1 pageHypocalcemia: Julie Allen, BVMS, MS, MRCVS, Dacvim (Saim), DacvpElenaNo ratings yet
- Use of Intravenous Fluidssolutions A Narrative ReviewDocument14 pagesUse of Intravenous Fluidssolutions A Narrative Reviewbarbarba obrequeNo ratings yet
- A Physiologic-Based Approach To The Treatment of A Patient With HypokalemiaDocument6 pagesA Physiologic-Based Approach To The Treatment of A Patient With HypokalemiaPablo IgnacioNo ratings yet
- Ex Vivo Heart ProjectDocument41 pagesEx Vivo Heart ProjectKitchanan KosalathipNo ratings yet
- Ionized Alkaline Water New Strategy For ManagementDocument6 pagesIonized Alkaline Water New Strategy For ManagementninoNo ratings yet
- FsfsdfsDocument35 pagesFsfsdfsJonathan wiradinataNo ratings yet
- Case Presentation Station 3B Drug Study Sodium ChlorideDocument4 pagesCase Presentation Station 3B Drug Study Sodium ChloridehahahahaaaaaaaNo ratings yet
- Equine Fluid TherapyFrom EverandEquine Fluid TherapyC. Langdon FieldingNo ratings yet
- Fluid Therapy in Various ConditionsDocument62 pagesFluid Therapy in Various ConditionsAndy F MonroeNo ratings yet
- 01-Guidelines For Use of Hypertonic SalineDocument13 pages01-Guidelines For Use of Hypertonic SalineSatish VeerlaNo ratings yet
- Buffers and Isotonic SolutionsDocument16 pagesBuffers and Isotonic SolutionsGiang PhamNo ratings yet
- Hypertonic SalineDocument3 pagesHypertonic SalineEldimson BermudoNo ratings yet
- Kim 2021Document8 pagesKim 2021Arun AdhikariNo ratings yet
- Fluid Management BurnDocument13 pagesFluid Management BurnWeronika StarrNo ratings yet
- Pharmacy Calculations: Random Problems: Actimed by Generika DrugstoreDocument17 pagesPharmacy Calculations: Random Problems: Actimed by Generika Drugstoreamethyst grandeNo ratings yet
- Parenteral Medication Labels and Dosage CalculationDocument22 pagesParenteral Medication Labels and Dosage CalculationlisaNo ratings yet
- Repeated Up To 3times With 5min Interval, It Causes Hypotension)Document4 pagesRepeated Up To 3times With 5min Interval, It Causes Hypotension)Ebrahim MokhtarNo ratings yet
- PROJECT REPORT ON I.V. FLUID UNIT (Ringer's Lactate, Normal Saline, Dextrose 4.3%, 5%, 10%, 50% & Darrows Solution)Document13 pagesPROJECT REPORT ON I.V. FLUID UNIT (Ringer's Lactate, Normal Saline, Dextrose 4.3%, 5%, 10%, 50% & Darrows Solution)EIRI Board of Consultants and PublishersNo ratings yet
- Different Types of IV FluidsDocument10 pagesDifferent Types of IV FluidsMarinill SolimanNo ratings yet
- Fluid and Electrolyte ImbalancesDocument37 pagesFluid and Electrolyte Imbalancesapi-3797941100% (4)
- The Origin of IV FluidsDocument15 pagesThe Origin of IV Fluidsashley nicholeNo ratings yet
- اسئله جراحه عامه سنوات سابقه امتحان الامتيازDocument110 pagesاسئله جراحه عامه سنوات سابقه امتحان الامتيازZaid Zayed100% (1)
- Blood Transfusion PDFDocument8 pagesBlood Transfusion PDFHasan A AsFour100% (1)
- Parenteral InjectionsDocument42 pagesParenteral InjectionsAngelica AmandoNo ratings yet
- HESI Dosage Calculation Practice ExamDocument24 pagesHESI Dosage Calculation Practice Exambhilligoss35No ratings yet
- 05 - An Evaluation of Tetramethylbenzidine As A Presumptive Test For BloodDocument6 pages05 - An Evaluation of Tetramethylbenzidine As A Presumptive Test For BloodMicawber7No ratings yet
- Surgery-On CallDocument729 pagesSurgery-On CallNadhirah ZulkifliNo ratings yet
- Day 2 QuizDocument2 pagesDay 2 QuizAngie MandeoyaNo ratings yet
- Principles of Fluid Management 2015 PDFDocument17 pagesPrinciples of Fluid Management 2015 PDFJorge DíazNo ratings yet
- Acid-Base Balance Revisited - Stewart and Strong IonsDocument8 pagesAcid-Base Balance Revisited - Stewart and Strong IonsMileidys LopezNo ratings yet
- Drugs Used in EmergencyDocument7 pagesDrugs Used in EmergencyAzza DianNo ratings yet
- Iv-Infusion-Rate-Calculations and Sample QuestionsDocument3 pagesIv-Infusion-Rate-Calculations and Sample QuestionsACanNo ratings yet
- CG011.v1: Adult Drug Infusions: Drug Dose and Diluent Rate (Note UNITS) Y Site Compatibility (Not All-Inclusive) OtherDocument8 pagesCG011.v1: Adult Drug Infusions: Drug Dose and Diluent Rate (Note UNITS) Y Site Compatibility (Not All-Inclusive) OtheriqbalNo ratings yet
- Medications AdministrationDocument69 pagesMedications AdministrationyuddNo ratings yet
- Exam 2018 PDFDocument62 pagesExam 2018 PDFWondimu Koy100% (2)