Download as ppsx, pdf, or txt
You might also like
- Lecture 1 HISTOLOGY OF THE RESPIRATORY SYSTEMDocument53 pagesLecture 1 HISTOLOGY OF THE RESPIRATORY SYSTEMlilimanao86% (7)
- Measuring Health and Disease (Session 7 and 8) 2Document37 pagesMeasuring Health and Disease (Session 7 and 8) 2teklay100% (2)
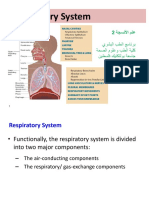
- Respiratory SystemDocument72 pagesRespiratory SystemmmmmmmmmmmNo ratings yet
- Histology Lecture. Histological Structure of URTDocument41 pagesHistology Lecture. Histological Structure of URTSounds of MindNo ratings yet
- ANA 221 - Respiratory Histology Copy 2Document68 pagesANA 221 - Respiratory Histology Copy 2Ototo ForexNo ratings yet
- Histology of Respiratory EpitheliumDocument61 pagesHistology of Respiratory EpitheliumNina Mornin GloryNo ratings yet
- 0402 Histo LectureDocument46 pages0402 Histo LectureJoe JNo ratings yet
- Respiratory System FKG 2020Document45 pagesRespiratory System FKG 2020Fira TasyaNo ratings yet
- Respiratory SystemDocument40 pagesRespiratory SystemCenen de GuzmanNo ratings yet
- His To RespDocument37 pagesHis To Respchocoholic potchiNo ratings yet
- Histology of Trachea and Lungs 2Document45 pagesHistology of Trachea and Lungs 2OnwumerechimdikepreciousNo ratings yet
- Histology of Lower Respiratory TractDocument42 pagesHistology of Lower Respiratory TractRahma ShofiNo ratings yet
- Histologi Kepala Leher THTDocument38 pagesHistologi Kepala Leher THTWidya ParamitaNo ratings yet
- Blood-Air Barrier That Separates The Blood in The Capillaries From The Air in The Air Sacs (Alveoli)Document5 pagesBlood-Air Barrier That Separates The Blood in The Capillaries From The Air in The Air Sacs (Alveoli)Sharon GabrielNo ratings yet
- Respiratory SystemDocument23 pagesRespiratory SystemZeianne BosabicaNo ratings yet
- 16 Respiratory System 2022Document67 pages16 Respiratory System 2022Yiannis AlatsathianosNo ratings yet
- Respiratory Lect1 240210 213802Document31 pagesRespiratory Lect1 240210 213802beneficialboxer9237No ratings yet
- TH E RE SP IRA TO RY SY ST EM: Learning ObjectivesDocument36 pagesTH E RE SP IRA TO RY SY ST EM: Learning Objectivesmaria tafaNo ratings yet
- Respiratory SystemDocument88 pagesRespiratory SystemoumerNo ratings yet
- Respiratory System HandoutDocument15 pagesRespiratory System HandoutJei SanNo ratings yet
- The Respiratory System PP First - Stage 2021Document27 pagesThe Respiratory System PP First - Stage 2021HHHNo ratings yet
- 17 Respiratory SystemDocument7 pages17 Respiratory SystemmariamhusseiniuniNo ratings yet
- Histo Respiratory-HistologyDocument14 pagesHisto Respiratory-HistologyMahmoud hilmyNo ratings yet
- Body System II 5 Respiratory 1Document27 pagesBody System II 5 Respiratory 1rrq8cwk2gnNo ratings yet
- Respiratory System: Indira PratiwiDocument53 pagesRespiratory System: Indira PratiwivirginiafbyNo ratings yet
- Respiratory PDFDocument55 pagesRespiratory PDFKristine De VillaNo ratings yet
- 3.3 Ear Histology 45Document48 pages3.3 Ear Histology 45Namomsa W.No ratings yet
- Histology of The Respiratory SystemDocument34 pagesHistology of The Respiratory Systemsanullah123khan.13No ratings yet
- Histology Lecture 6 - Respiratory SystemDocument43 pagesHistology Lecture 6 - Respiratory SystemMicahNo ratings yet
- Respiratory SystemDocument15 pagesRespiratory Systemرافت العواضيNo ratings yet
- Department of Histology Medical Faculty, University of North SumateraDocument44 pagesDepartment of Histology Medical Faculty, University of North Sumatera292Vien HardiyantiNo ratings yet
- San Beda Respiratory System 9-15Document68 pagesSan Beda Respiratory System 9-15conyxzNo ratings yet
- Lecture 6 RespiratoryDocument49 pagesLecture 6 Respiratoryngocnm.bi12-320No ratings yet
- Respiratory SystemDocument54 pagesRespiratory SystemEndin Nokik StujannaNo ratings yet
- Respiratory System: General Histology by Falia, JoyjoyDocument29 pagesRespiratory System: General Histology by Falia, JoyjoyJoyjoy FaliaNo ratings yet
- 25 10uhygtfcDocument91 pages25 10uhygtfcfdla rhmahNo ratings yet
- Complete Histology of Respiratory SystemDocument66 pagesComplete Histology of Respiratory Systemhassam qazi100% (1)
- Lec 5 HistologyDocument25 pagesLec 5 Histologyأ. علي محمدNo ratings yet
- Respiratory Lect2 - 2022 240210 213849Document39 pagesRespiratory Lect2 - 2022 240210 213849beneficialboxer9237No ratings yet
- Histology of Respiratory System: Dr. Mirna Muis, SP - Rad Dept. of Histology Faculty of Medicine, Hasanuddin UnivDocument31 pagesHistology of Respiratory System: Dr. Mirna Muis, SP - Rad Dept. of Histology Faculty of Medicine, Hasanuddin UnivNor Izhharuddin ZainyNo ratings yet
- Respiratory SystemDocument13 pagesRespiratory SystemJabbawokeez KiddsNo ratings yet
- Histology of The Larynx, BronchiDocument49 pagesHistology of The Larynx, BronchiAffie SaikolNo ratings yet
- UntitledDocument62 pagesUntitledManaye MamuyeNo ratings yet
- Respiratory System by Dr. Vincent-JrDocument48 pagesRespiratory System by Dr. Vincent-JrEmma OsabohienNo ratings yet
- 1. Histology of Respiratory SystemDocument65 pages1. Histology of Respiratory SystemOloruntomi AdesinaNo ratings yet
- Lymphoid OrgansDocument4 pagesLymphoid OrgansJadys Merill DiezNo ratings yet
- RESPIRATORY LAB. Edited - PPTX STDocument33 pagesRESPIRATORY LAB. Edited - PPTX STLORENA POLONNo ratings yet
- Respiratory AnatomyDocument50 pagesRespiratory Anatomynimonayoseph27No ratings yet
- MTHISTO100 Lesson 2 Respiratory SystemDocument7 pagesMTHISTO100 Lesson 2 Respiratory SystemJaeri HuangNo ratings yet
- Respiratoy System HistologyDocument32 pagesRespiratoy System HistologyNaveed AkhterNo ratings yet
- Respiratory SystemDocument15 pagesRespiratory SystemJovelou MihangosNo ratings yet
- 11 Respiratory Pharma PrintDocument53 pages11 Respiratory Pharma Printabenezer isayasNo ratings yet
- Physiology Of: RespirationDocument51 pagesPhysiology Of: RespirationDr. R. PeriasamyNo ratings yet
- Anatomy and Physiology of The Respiratory SystemDocument43 pagesAnatomy and Physiology of The Respiratory SystemChristina GonezNo ratings yet
- 2012 EarDocument7 pages2012 EarDinar Riny NvNo ratings yet
- Lecture 4Document7 pagesLecture 4cejix87209No ratings yet
- NCM 113 M1 Lesson 1Document10 pagesNCM 113 M1 Lesson 1Ryrl ShinNo ratings yet
- Respiratory Tract Part 1Document62 pagesRespiratory Tract Part 1El-rohyKalongoNo ratings yet
- Anatomy of EarDocument32 pagesAnatomy of EartarshaNo ratings yet
- A Guide for the Dissection of the Dogfish (Squalus Acanthias)From EverandA Guide for the Dissection of the Dogfish (Squalus Acanthias)No ratings yet
- CHAPTER 6 Epidemiological SurveillanceDocument50 pagesCHAPTER 6 Epidemiological Surveillanceteklay100% (1)
- CHAPTER 2 Infectious EpidemiologyDocument89 pagesCHAPTER 2 Infectious EpidemiologyteklayNo ratings yet
- CHAPTER 1 Introduction To Epidemiology MPHDocument84 pagesCHAPTER 1 Introduction To Epidemiology MPHteklayNo ratings yet
- CHAPTER 3 Non-Communicable Disease EpidemiologyDocument24 pagesCHAPTER 3 Non-Communicable Disease EpidemiologyteklayNo ratings yet
- Global Cooperation in Health: Manay KifleDocument45 pagesGlobal Cooperation in Health: Manay KifleteklayNo ratings yet
- CHAPTER 4 Environmental EpidemiologyDocument23 pagesCHAPTER 4 Environmental EpidemiologyteklayNo ratings yet
- Emerging and Re Emerging DiseasesDocument49 pagesEmerging and Re Emerging DiseasesteklayNo ratings yet
- Epidemiology For MPH StudentsDocument91 pagesEpidemiology For MPH StudentsteklayNo ratings yet
- 1 Problem Solving & Dicision MakingDocument55 pages1 Problem Solving & Dicision MakingteklayNo ratings yet
- Evidence-Based Public HealthDocument21 pagesEvidence-Based Public HealthteklayNo ratings yet
- Chapter-4 Health Professionals Motivation: Zemichael WGDocument37 pagesChapter-4 Health Professionals Motivation: Zemichael WGteklayNo ratings yet
- 2 Management of Specialized Projects, ProgramesDocument67 pages2 Management of Specialized Projects, ProgramesteklayNo ratings yet
- ch-8 Conflict Management in The Health Sector (2016 - 03 - 30 15 - 23 - 50 UTC)Document61 pagesch-8 Conflict Management in The Health Sector (2016 - 03 - 30 15 - 23 - 50 UTC)teklayNo ratings yet
- Ch-4 Leadership For MPHDocument69 pagesCh-4 Leadership For MPHteklayNo ratings yet
- L - 3 Outbreak InvestigationDocument57 pagesL - 3 Outbreak InvestigationteklayNo ratings yet
- CH-1 Introduction To HSM For MPHDocument96 pagesCH-1 Introduction To HSM For MPHteklayNo ratings yet
- Epidemics: Fessahaye Alemseged (MD, MPHE)Document34 pagesEpidemics: Fessahaye Alemseged (MD, MPHE)teklay100% (1)
- Screening: Berhe Beyene (Email:)Document71 pagesScreening: Berhe Beyene (Email:)teklayNo ratings yet
- L - 1measure of AssociationsDocument48 pagesL - 1measure of AssociationsteklayNo ratings yet
- Aksum University-Department of Nursing For 3 Yr BSC Nursing StudentsDocument21 pagesAksum University-Department of Nursing For 3 Yr BSC Nursing StudentsteklayNo ratings yet
- Course Syllabus of IT PG PDFDocument39 pagesCourse Syllabus of IT PG PDFteklayNo ratings yet
- Functions of Public HealthDocument30 pagesFunctions of Public Healthteklay100% (1)
- Validity of Epi Studies 2019Document26 pagesValidity of Epi Studies 2019teklayNo ratings yet
- Statistical Methods in Epi 2019Document30 pagesStatistical Methods in Epi 2019teklayNo ratings yet
- Economic Evaluation (MPH)Document52 pagesEconomic Evaluation (MPH)teklayNo ratings yet
- Buku Panduan TBDocument111 pagesBuku Panduan TBwidia mujtiawatiNo ratings yet
- Colour Atlas of Vertebrate Anatomy PDFDocument2 pagesColour Atlas of Vertebrate Anatomy PDFJeffrey0% (3)
- OligohidramnionDocument9 pagesOligohidramnionRizki R. WahidahNo ratings yet
- Humidificado Aquecido Marca Vapotherm Modelo Precision FlowDocument32 pagesHumidificado Aquecido Marca Vapotherm Modelo Precision FlowEng. Edelson MartinsNo ratings yet
- Balanitis and Balanoposthitis - Review ArticleDocument10 pagesBalanitis and Balanoposthitis - Review Articleikbalnur03No ratings yet
- Electrical Shock First AidDocument17 pagesElectrical Shock First Aiddpc876No ratings yet
- Geographic TongueDocument2 pagesGeographic TongueclaudianrjNo ratings yet
- Bassett and Turner 2007Document17 pagesBassett and Turner 2007Ludovic FanstenNo ratings yet
- F.E. Campbell - Bound Wrists Hit 199Document124 pagesF.E. Campbell - Bound Wrists Hit 199HokusLocus67% (6)
- AbdomenDocument9 pagesAbdomenJazzmyne T.No ratings yet
- Special CirculationsDocument29 pagesSpecial Circulationslessank12100% (1)
- Matthias Hofer - Ultrasound Teaching Manual - The Basics of Performing and Interpreting Ultrasound Scans-Thieme (2021)Document173 pagesMatthias Hofer - Ultrasound Teaching Manual - The Basics of Performing and Interpreting Ultrasound Scans-Thieme (2021)Аркадий ЖивицаNo ratings yet
- C-MAMI Enrolment and Management CardDocument3 pagesC-MAMI Enrolment and Management CardAbebe TilahunNo ratings yet
- Safe Food HandlerDocument24 pagesSafe Food HandlermaddieecomeauNo ratings yet
- Anti-Fungal: Tinea Flava, Ringworm, Athlete's Foot and ScabiesDocument2 pagesAnti-Fungal: Tinea Flava, Ringworm, Athlete's Foot and ScabiesShairuz Caesar Briones DugayNo ratings yet
- Liquid H2O Is The Sine Qua Non of LifeDocument2 pagesLiquid H2O Is The Sine Qua Non of LifeShafiq HakimiNo ratings yet
- AnaphyDocument8 pagesAnaphyCELLINA CLARISSE DE LEONNo ratings yet
- Hawke S Pride Norah HessDocument201 pagesHawke S Pride Norah HessZe John100% (4)
- See My Pet Again in HeavenDocument4 pagesSee My Pet Again in HeavenVince MiglioreNo ratings yet
- Busulfan Induces Apoptotic and Cytotoxic Effects On Testis and Epididymal Sperm of Adult Male Mouse Following Low Dose TreatmentDocument9 pagesBusulfan Induces Apoptotic and Cytotoxic Effects On Testis and Epididymal Sperm of Adult Male Mouse Following Low Dose TreatmentInternational Network For Natural SciencesNo ratings yet
- Parts of The Respiratory System & Their FunctionsDocument38 pagesParts of The Respiratory System & Their FunctionsSaajid AmraNo ratings yet
- Lab Exercise 38Document8 pagesLab Exercise 38lalaNo ratings yet
- 4 Metabolic Response of Tissue To InjuryDocument5 pages4 Metabolic Response of Tissue To InjuryZllison Mae Teodoro Mangabat100% (1)
- Short - and Long-Term Effects of The Herbst Appliance On Temporomandibular Joint FunctionDocument13 pagesShort - and Long-Term Effects of The Herbst Appliance On Temporomandibular Joint FunctionSushma Rayal SANo ratings yet
- NCP Risk For InfectionDocument2 pagesNCP Risk For Infectionnj_pink08179460% (5)
- Dengue Hemorrhagic Fever PathophysiologyDocument4 pagesDengue Hemorrhagic Fever PathophysiologyKirk Espanol BigstoneNo ratings yet
- Epn 3 Modul 14Document9 pagesEpn 3 Modul 14CesarNo ratings yet
- Aap 2023 The Darkness Behind The Spotlights FinalDocument26 pagesAap 2023 The Darkness Behind The Spotlights FinalRoel PlmrsNo ratings yet
- My 4-H Dog Care and Training Project Record BookDocument28 pagesMy 4-H Dog Care and Training Project Record BookKavya BajajNo ratings yet
- Key To PhoneticDocument13 pagesKey To PhoneticMidou El MàtàdøŗNo ratings yet