
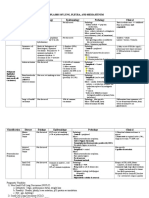
Neoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology Clinical
Neoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology Clinical
You might also like
- Primary Aldosteronism - A Multidimensional SyndromeDocument18 pagesPrimary Aldosteronism - A Multidimensional SyndromeErwin SiahaanNo ratings yet
- Khantzian, Edward J. (2008), Understanding Addiction As Self MedicationDocument177 pagesKhantzian, Edward J. (2008), Understanding Addiction As Self MedicationmirandacatalinaNo ratings yet
- General Practitioner Sample Resume WWW - Careerfaqs.com - AuDocument3 pagesGeneral Practitioner Sample Resume WWW - Careerfaqs.com - AuSubhash RitwalNo ratings yet
- Neoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalDocument4 pagesNeoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalMrSomnambululNo ratings yet
- Lungs Benign and MalignantDocument7 pagesLungs Benign and MalignantNestley TiongsonNo ratings yet
- General Stages and TX of Malignant Cells? Naming TumorsDocument11 pagesGeneral Stages and TX of Malignant Cells? Naming TumorsRyan TurnerNo ratings yet
- Neoplasms of The ThyroidDocument5 pagesNeoplasms of The ThyroidMahmoud AbouelsoudNo ratings yet
- " Chest:: by Definition Malignant Tumor of The Lung Primary Its EtiologyDocument10 pages" Chest:: by Definition Malignant Tumor of The Lung Primary Its EtiologyAhmed GaberNo ratings yet
- CESA January 2009Document7 pagesCESA January 2009Anonymous rZdsbP67iXNo ratings yet
- 5 Lung TumorsDocument23 pages5 Lung TumorsAnupam NathNo ratings yet
- Oral Pathology Dent1411Document7 pagesOral Pathology Dent1411api-663458841No ratings yet
- Respiratory 03 - Bronchiogenic CA: 1) Smoking/industrial Hazards/air Pollution 2) Molecular Genetic MutationDocument2 pagesRespiratory 03 - Bronchiogenic CA: 1) Smoking/industrial Hazards/air Pollution 2) Molecular Genetic Mutationkamil malikNo ratings yet
- Path Adrenal TumorDocument4 pagesPath Adrenal TumorRama HijaziNo ratings yet
- 01 FNAC Approach To Scrotal MassesDocument3 pages01 FNAC Approach To Scrotal MassescandiddreamsNo ratings yet
- Salivary Gland TumorsDocument16 pagesSalivary Gland Tumorsmaria del mar RoblesNo ratings yet
- Aparato Genital MasculinoDocument22 pagesAparato Genital MasculinoletttttNo ratings yet
- Breast Cancer Didactics - ManzanoDocument49 pagesBreast Cancer Didactics - ManzanoJoy ManzanoNo ratings yet
- Notes DermaDocument17 pagesNotes DermaCiullaeNo ratings yet
- Lung Ca Small Bx2 PDFDocument4 pagesLung Ca Small Bx2 PDFJose SirittNo ratings yet
- Thyroid Neoplasms: Muhammad Haris Aslam Janjua Resident, Surgical Unit I SIMS/Services Hospital, LahoreDocument116 pagesThyroid Neoplasms: Muhammad Haris Aslam Janjua Resident, Surgical Unit I SIMS/Services Hospital, LahoreHajra IsrarNo ratings yet
- Neoplasia: Monoclonal Unregulated, and IrreversibleDocument10 pagesNeoplasia: Monoclonal Unregulated, and Irreversiblehippypsyduck mdNo ratings yet
- URO 3 - Neoplasm in The Genitourinary TractDocument8 pagesURO 3 - Neoplasm in The Genitourinary TractHa Jae kyeongNo ratings yet
- Female GUDocument18 pagesFemale GULauren LaMonicaNo ratings yet
- Lung TumoursDocument43 pagesLung TumourseviltohuntNo ratings yet
- NeoplasiaDocument78 pagesNeoplasiageetikaNo ratings yet
- Adult Desmoid Tumors: Biology, Management and Ongoing TrialsDocument7 pagesAdult Desmoid Tumors: Biology, Management and Ongoing TrialsGustavo GasperiNo ratings yet
- Curr Diag Pathol-2006-12 - Sinonasal CarcinomasDocument14 pagesCurr Diag Pathol-2006-12 - Sinonasal Carcinomasdarmayanti ibnuNo ratings yet
- Surgical Pathology - Major and Minor Salivary GlandsDocument2 pagesSurgical Pathology - Major and Minor Salivary GlandsIsabel CastilloNo ratings yet
- Ocular LymphomaDocument67 pagesOcular LymphomaFera Yunita RodhiatyNo ratings yet
- Lung Tumors PDFDocument15 pagesLung Tumors PDFJose SirittNo ratings yet
- Additional Notes in Pedia Neuro2Document4 pagesAdditional Notes in Pedia Neuro2Geraldine Marie SalvoNo ratings yet
- Ped Solid TumorDocument52 pagesPed Solid TumorIndranil GhoshNo ratings yet
- Y1.6 Neoplasia - Malignant Tumors 2022 PDFDocument41 pagesY1.6 Neoplasia - Malignant Tumors 2022 PDFlina hossamNo ratings yet
- CNS Tumors NeurologyDocument45 pagesCNS Tumors NeurologyChristinaNo ratings yet
- Dr. P. Karpagam Kiruba Rajeswari, M.B.B.S.,D.C.P., Tutor in Pathology, MapimsDocument59 pagesDr. P. Karpagam Kiruba Rajeswari, M.B.B.S.,D.C.P., Tutor in Pathology, MapimsIntan Eklesiana Napitupulu100% (1)
- Genetic Diseases: Mendelian Inheritance Multifactorial Inheritance Chromosome Inheritance Mitochondria InheritanceDocument74 pagesGenetic Diseases: Mendelian Inheritance Multifactorial Inheritance Chromosome Inheritance Mitochondria InheritanceinakiNo ratings yet
- Descriptive Techniques in Pathology IIRoccabiancaDocument9 pagesDescriptive Techniques in Pathology IIRoccabiancaLajla KušmićNo ratings yet
- Thyroid CancersDocument10 pagesThyroid Cancerssk100% (1)
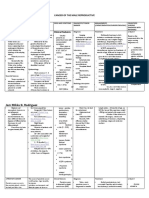
- Jam Mikka G. Rodriguez (Cancer of The Male Reproductive 1)Document12 pagesJam Mikka G. Rodriguez (Cancer of The Male Reproductive 1)Dinarkram Rabreca EculNo ratings yet
- Dermatology SummariesDocument7 pagesDermatology SummariesShiv KolheNo ratings yet
- Skin Cancer ShowDocument57 pagesSkin Cancer ShowNice YouNo ratings yet
- A.K12 - FINAL Management Brain Tumors Dr. Dr. Rr. Suzy Indharty, M. Kes, SP - BsDocument42 pagesA.K12 - FINAL Management Brain Tumors Dr. Dr. Rr. Suzy Indharty, M. Kes, SP - BsandrianyNo ratings yet
- Nose Sinus CA Slides 040519Document40 pagesNose Sinus CA Slides 040519AchmadPrihadiantoNo ratings yet
- Epk FDocument73 pagesEpk FBryan FjbNo ratings yet
- Bladder Cancer BasicsDocument1 pageBladder Cancer BasicsAziz KhalidNo ratings yet
- Testicular TumorsDocument14 pagesTesticular TumorsJose SirittNo ratings yet
- Pharma en OncologyDocument14 pagesPharma en Oncologyyaqoob008No ratings yet
- Eca - Cellular Aberration-Neuro-MusculoskeletalDocument29 pagesEca - Cellular Aberration-Neuro-MusculoskeletalFrancis Alfred EscaranNo ratings yet
- Cellular Aberrations NotesDocument22 pagesCellular Aberrations NotesH50% (2)
- Chapter 16 - Head and NeckDocument8 pagesChapter 16 - Head and NeckAgnieszka WisniewskaNo ratings yet
- Cellular Aberrations NotesDocument23 pagesCellular Aberrations NotesPamela Ria HensonNo ratings yet
- Sarcomas: Bone Sarcoma Soft Tissue SarcomasDocument3 pagesSarcomas: Bone Sarcoma Soft Tissue SarcomasCharlie65129No ratings yet
- Thyroid Malignancy With MRNDDocument25 pagesThyroid Malignancy With MRNDRashma JosephNo ratings yet
- Update On Nasopharyngeal Carcinoma: Ó Humana 2007Document6 pagesUpdate On Nasopharyngeal Carcinoma: Ó Humana 2007Zakia AjaNo ratings yet
- Presentation 1Document31 pagesPresentation 1Nice YouNo ratings yet
- Screenshot 2023-03-01 at 3.14.03 PMDocument17 pagesScreenshot 2023-03-01 at 3.14.03 PMmohameeedar1No ratings yet
- CA M1 RVWR HshsDocument5 pagesCA M1 RVWR HshscharmiemabaoNo ratings yet
- Salivary Gland TumoursDocument131 pagesSalivary Gland TumoursSushmithaNo ratings yet
- Thyroid CancerDocument11 pagesThyroid Cancermarselia23No ratings yet
- Didactics 3 - Neoplastic Diseases of The Salivary Glands (Autosaved)Document28 pagesDidactics 3 - Neoplastic Diseases of The Salivary Glands (Autosaved)Moritz SolivenNo ratings yet
- Head and Neck: Salivary Gland Tumors: An OverviewDocument12 pagesHead and Neck: Salivary Gland Tumors: An OverviewVanessa MordiNo ratings yet
- Salivary Gland Neoplasms: Dr. Sohail BakkarDocument14 pagesSalivary Gland Neoplasms: Dr. Sohail Bakkarseun williamsNo ratings yet
- Spun Candy Investor PresentationDocument32 pagesSpun Candy Investor PresentationMrSomnambululNo ratings yet
- Enrolment Overview: 1. Select My Student Center' From Your Myglasgow HomepageDocument16 pagesEnrolment Overview: 1. Select My Student Center' From Your Myglasgow HomepageMrSomnambululNo ratings yet
- ChitosanDocument52 pagesChitosanMrSomnambululNo ratings yet
- 100-2010 Zhabg PDFDocument8 pages100-2010 Zhabg PDFMrSomnambululNo ratings yet
- Notes On HomeworkDocument19 pagesNotes On HomeworkMrSomnambululNo ratings yet
- Applications of Chitin and Chitosan in Industry and Medical Science: A ReviewDocument6 pagesApplications of Chitin and Chitosan in Industry and Medical Science: A ReviewMrSomnambululNo ratings yet
- Chitosan: Kimberly Novak, Melanie Johns Cupp, and Timothy S. TracyDocument9 pagesChitosan: Kimberly Novak, Melanie Johns Cupp, and Timothy S. TracyMrSomnambululNo ratings yet
- Chapter 9 Subtract Ive MixingDocument19 pagesChapter 9 Subtract Ive MixingMrSomnambululNo ratings yet
- Chapter 9: Color Additive Primary ColorsDocument19 pagesChapter 9: Color Additive Primary ColorsMrSomnambululNo ratings yet
- Course Info: Dr. Ellen KeisterDocument14 pagesCourse Info: Dr. Ellen KeisterMrSomnambululNo ratings yet
- Chapter 7 Receptive Fields 2Document18 pagesChapter 7 Receptive Fields 2MrSomnambululNo ratings yet
- Chapter 5 EyeDocument14 pagesChapter 5 EyeMrSomnambululNo ratings yet
- Chapter 4: Cameras and Photography: - Depth of Field - ExposureDocument21 pagesChapter 4: Cameras and Photography: - Depth of Field - ExposureMrSomnambululNo ratings yet
- Homework Policies: - Molly: Tuesdays 2-4pm - Dr. Keister: Wednesdays 10am-12 - Prof. Goldman: Wednesdays 2-3:30pmDocument14 pagesHomework Policies: - Molly: Tuesdays 2-4pm - Dr. Keister: Wednesdays 10am-12 - Prof. Goldman: Wednesdays 2-3:30pmMrSomnambululNo ratings yet
- L 10 BalanceDocument11 pagesL 10 BalanceMrSomnambululNo ratings yet
- The Physiology of The Senses - Touch, Pain, Taste and SmellDocument20 pagesThe Physiology of The Senses - Touch, Pain, Taste and SmellMrSomnambululNo ratings yet
- 12taste and SmellDocument19 pages12taste and SmellMrSomnambululNo ratings yet
- Faith To Go ForwardDocument10 pagesFaith To Go ForwardAlejandro DominguezNo ratings yet
- EULAR RecommendationsDocument13 pagesEULAR RecommendationsAmer Wasim100% (1)
- Daftar Harga Tiap PBFDocument4 pagesDaftar Harga Tiap PBFPraja Setia NingsihNo ratings yet
- Patofisiologi HematuriaDocument10 pagesPatofisiologi HematuriaNurunSalamanNo ratings yet
- College of NursingDocument1 pageCollege of NursingJohn Michael Manlupig PitoyNo ratings yet
- Laboratory and Diagnostic ExaminationDocument3 pagesLaboratory and Diagnostic ExaminationRose Anne MücklNo ratings yet
- CVS - Charts & DiagramsDocument20 pagesCVS - Charts & DiagramsMamathaNo ratings yet
- Opioid SpeechDocument3 pagesOpioid Speechapi-267758642No ratings yet
- Bahan Tutor Skenario 3Document5 pagesBahan Tutor Skenario 3Azka MuflihaNo ratings yet
- Hospital Literature StudyDocument52 pagesHospital Literature Studylakshma reddyNo ratings yet
- Oral Motor ExercisesDocument7 pagesOral Motor Exercisesmeh wish100% (5)
- Acute Respiratory Distress Syndrome - Background, Pathophysiology, EtiologyDocument5 pagesAcute Respiratory Distress Syndrome - Background, Pathophysiology, EtiologyARHNo ratings yet
- 40 Normal Labor and DystociaDocument47 pages40 Normal Labor and DystociaCitra Wulandari SofyanNo ratings yet
- Soft Tissue Infection by SlidesgoDocument40 pagesSoft Tissue Infection by SlidesgoDurga MadhuriNo ratings yet
- PedsCases CF Note (SP Edit)Document1 pagePedsCases CF Note (SP Edit)Mehtab AlamNo ratings yet
- Thyroid Function Tests: What Is The Thyroid Gland?Document2 pagesThyroid Function Tests: What Is The Thyroid Gland?rastamaneazy269No ratings yet
- Dabur Product PortfolioDocument18 pagesDabur Product PortfolioAshutosh SamantNo ratings yet
- Pathophysiology of Myocardial Infarction (STEMI)Document2 pagesPathophysiology of Myocardial Infarction (STEMI)michaela100% (3)
- Photo EssayDocument13 pagesPhoto Essayapi-314854412No ratings yet
- MCL FormatDocument49 pagesMCL Formatasheesh kumarNo ratings yet
- Valvular Heart Disease: Bekele T. (MD)Document47 pagesValvular Heart Disease: Bekele T. (MD)alehegn beleteNo ratings yet
- Applications of EnzymesDocument9 pagesApplications of EnzymesRabia HussainNo ratings yet
- Case Presentation 2Document135 pagesCase Presentation 2Muhammad AliNo ratings yet
- Gastrointestinal Tract System NotesDocument8 pagesGastrointestinal Tract System NotesCarl Elexer Cuyugan Ano100% (1)
- Algoritma StatinDocument1 pageAlgoritma StatinAgnes Irene ZagotoNo ratings yet
- Danger Signs During Pregnancy 4 1Document33 pagesDanger Signs During Pregnancy 4 1Precious Maslang PadawilNo ratings yet





































































































Download as doc, pdf, or txt
You might also like
- Primary Aldosteronism - A Multidimensional SyndromeDocument18 pagesPrimary Aldosteronism - A Multidimensional SyndromeErwin SiahaanNo ratings yet
- Khantzian, Edward J. (2008), Understanding Addiction As Self MedicationDocument177 pagesKhantzian, Edward J. (2008), Understanding Addiction As Self MedicationmirandacatalinaNo ratings yet
- General Practitioner Sample Resume WWW - Careerfaqs.com - AuDocument3 pagesGeneral Practitioner Sample Resume WWW - Careerfaqs.com - AuSubhash RitwalNo ratings yet
- Neoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalDocument4 pagesNeoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalMrSomnambululNo ratings yet
- Lungs Benign and MalignantDocument7 pagesLungs Benign and MalignantNestley TiongsonNo ratings yet
- General Stages and TX of Malignant Cells? Naming TumorsDocument11 pagesGeneral Stages and TX of Malignant Cells? Naming TumorsRyan TurnerNo ratings yet
- Neoplasms of The ThyroidDocument5 pagesNeoplasms of The ThyroidMahmoud AbouelsoudNo ratings yet
- " Chest:: by Definition Malignant Tumor of The Lung Primary Its EtiologyDocument10 pages" Chest:: by Definition Malignant Tumor of The Lung Primary Its EtiologyAhmed GaberNo ratings yet
- CESA January 2009Document7 pagesCESA January 2009Anonymous rZdsbP67iXNo ratings yet
- 5 Lung TumorsDocument23 pages5 Lung TumorsAnupam NathNo ratings yet
- Oral Pathology Dent1411Document7 pagesOral Pathology Dent1411api-663458841No ratings yet
- Respiratory 03 - Bronchiogenic CA: 1) Smoking/industrial Hazards/air Pollution 2) Molecular Genetic MutationDocument2 pagesRespiratory 03 - Bronchiogenic CA: 1) Smoking/industrial Hazards/air Pollution 2) Molecular Genetic Mutationkamil malikNo ratings yet
- Path Adrenal TumorDocument4 pagesPath Adrenal TumorRama HijaziNo ratings yet
- 01 FNAC Approach To Scrotal MassesDocument3 pages01 FNAC Approach To Scrotal MassescandiddreamsNo ratings yet
- Salivary Gland TumorsDocument16 pagesSalivary Gland Tumorsmaria del mar RoblesNo ratings yet
- Aparato Genital MasculinoDocument22 pagesAparato Genital MasculinoletttttNo ratings yet
- Breast Cancer Didactics - ManzanoDocument49 pagesBreast Cancer Didactics - ManzanoJoy ManzanoNo ratings yet
- Notes DermaDocument17 pagesNotes DermaCiullaeNo ratings yet
- Lung Ca Small Bx2 PDFDocument4 pagesLung Ca Small Bx2 PDFJose SirittNo ratings yet
- Thyroid Neoplasms: Muhammad Haris Aslam Janjua Resident, Surgical Unit I SIMS/Services Hospital, LahoreDocument116 pagesThyroid Neoplasms: Muhammad Haris Aslam Janjua Resident, Surgical Unit I SIMS/Services Hospital, LahoreHajra IsrarNo ratings yet
- Neoplasia: Monoclonal Unregulated, and IrreversibleDocument10 pagesNeoplasia: Monoclonal Unregulated, and Irreversiblehippypsyduck mdNo ratings yet
- URO 3 - Neoplasm in The Genitourinary TractDocument8 pagesURO 3 - Neoplasm in The Genitourinary TractHa Jae kyeongNo ratings yet
- Female GUDocument18 pagesFemale GULauren LaMonicaNo ratings yet
- Lung TumoursDocument43 pagesLung TumourseviltohuntNo ratings yet
- NeoplasiaDocument78 pagesNeoplasiageetikaNo ratings yet
- Adult Desmoid Tumors: Biology, Management and Ongoing TrialsDocument7 pagesAdult Desmoid Tumors: Biology, Management and Ongoing TrialsGustavo GasperiNo ratings yet
- Curr Diag Pathol-2006-12 - Sinonasal CarcinomasDocument14 pagesCurr Diag Pathol-2006-12 - Sinonasal Carcinomasdarmayanti ibnuNo ratings yet
- Surgical Pathology - Major and Minor Salivary GlandsDocument2 pagesSurgical Pathology - Major and Minor Salivary GlandsIsabel CastilloNo ratings yet
- Ocular LymphomaDocument67 pagesOcular LymphomaFera Yunita RodhiatyNo ratings yet
- Lung Tumors PDFDocument15 pagesLung Tumors PDFJose SirittNo ratings yet
- Additional Notes in Pedia Neuro2Document4 pagesAdditional Notes in Pedia Neuro2Geraldine Marie SalvoNo ratings yet
- Ped Solid TumorDocument52 pagesPed Solid TumorIndranil GhoshNo ratings yet
- Y1.6 Neoplasia - Malignant Tumors 2022 PDFDocument41 pagesY1.6 Neoplasia - Malignant Tumors 2022 PDFlina hossamNo ratings yet
- CNS Tumors NeurologyDocument45 pagesCNS Tumors NeurologyChristinaNo ratings yet
- Dr. P. Karpagam Kiruba Rajeswari, M.B.B.S.,D.C.P., Tutor in Pathology, MapimsDocument59 pagesDr. P. Karpagam Kiruba Rajeswari, M.B.B.S.,D.C.P., Tutor in Pathology, MapimsIntan Eklesiana Napitupulu100% (1)
- Genetic Diseases: Mendelian Inheritance Multifactorial Inheritance Chromosome Inheritance Mitochondria InheritanceDocument74 pagesGenetic Diseases: Mendelian Inheritance Multifactorial Inheritance Chromosome Inheritance Mitochondria InheritanceinakiNo ratings yet
- Descriptive Techniques in Pathology IIRoccabiancaDocument9 pagesDescriptive Techniques in Pathology IIRoccabiancaLajla KušmićNo ratings yet
- Thyroid CancersDocument10 pagesThyroid Cancerssk100% (1)
- Jam Mikka G. Rodriguez (Cancer of The Male Reproductive 1)Document12 pagesJam Mikka G. Rodriguez (Cancer of The Male Reproductive 1)Dinarkram Rabreca EculNo ratings yet
- Dermatology SummariesDocument7 pagesDermatology SummariesShiv KolheNo ratings yet
- Skin Cancer ShowDocument57 pagesSkin Cancer ShowNice YouNo ratings yet
- A.K12 - FINAL Management Brain Tumors Dr. Dr. Rr. Suzy Indharty, M. Kes, SP - BsDocument42 pagesA.K12 - FINAL Management Brain Tumors Dr. Dr. Rr. Suzy Indharty, M. Kes, SP - BsandrianyNo ratings yet
- Nose Sinus CA Slides 040519Document40 pagesNose Sinus CA Slides 040519AchmadPrihadiantoNo ratings yet
- Epk FDocument73 pagesEpk FBryan FjbNo ratings yet
- Bladder Cancer BasicsDocument1 pageBladder Cancer BasicsAziz KhalidNo ratings yet
- Testicular TumorsDocument14 pagesTesticular TumorsJose SirittNo ratings yet
- Pharma en OncologyDocument14 pagesPharma en Oncologyyaqoob008No ratings yet
- Eca - Cellular Aberration-Neuro-MusculoskeletalDocument29 pagesEca - Cellular Aberration-Neuro-MusculoskeletalFrancis Alfred EscaranNo ratings yet
- Cellular Aberrations NotesDocument22 pagesCellular Aberrations NotesH50% (2)
- Chapter 16 - Head and NeckDocument8 pagesChapter 16 - Head and NeckAgnieszka WisniewskaNo ratings yet
- Cellular Aberrations NotesDocument23 pagesCellular Aberrations NotesPamela Ria HensonNo ratings yet
- Sarcomas: Bone Sarcoma Soft Tissue SarcomasDocument3 pagesSarcomas: Bone Sarcoma Soft Tissue SarcomasCharlie65129No ratings yet
- Thyroid Malignancy With MRNDDocument25 pagesThyroid Malignancy With MRNDRashma JosephNo ratings yet
- Update On Nasopharyngeal Carcinoma: Ó Humana 2007Document6 pagesUpdate On Nasopharyngeal Carcinoma: Ó Humana 2007Zakia AjaNo ratings yet
- Presentation 1Document31 pagesPresentation 1Nice YouNo ratings yet
- Screenshot 2023-03-01 at 3.14.03 PMDocument17 pagesScreenshot 2023-03-01 at 3.14.03 PMmohameeedar1No ratings yet
- CA M1 RVWR HshsDocument5 pagesCA M1 RVWR HshscharmiemabaoNo ratings yet
- Salivary Gland TumoursDocument131 pagesSalivary Gland TumoursSushmithaNo ratings yet
- Thyroid CancerDocument11 pagesThyroid Cancermarselia23No ratings yet
- Didactics 3 - Neoplastic Diseases of The Salivary Glands (Autosaved)Document28 pagesDidactics 3 - Neoplastic Diseases of The Salivary Glands (Autosaved)Moritz SolivenNo ratings yet
- Head and Neck: Salivary Gland Tumors: An OverviewDocument12 pagesHead and Neck: Salivary Gland Tumors: An OverviewVanessa MordiNo ratings yet
- Salivary Gland Neoplasms: Dr. Sohail BakkarDocument14 pagesSalivary Gland Neoplasms: Dr. Sohail Bakkarseun williamsNo ratings yet
- Spun Candy Investor PresentationDocument32 pagesSpun Candy Investor PresentationMrSomnambululNo ratings yet
- Enrolment Overview: 1. Select My Student Center' From Your Myglasgow HomepageDocument16 pagesEnrolment Overview: 1. Select My Student Center' From Your Myglasgow HomepageMrSomnambululNo ratings yet
- ChitosanDocument52 pagesChitosanMrSomnambululNo ratings yet
- 100-2010 Zhabg PDFDocument8 pages100-2010 Zhabg PDFMrSomnambululNo ratings yet
- Notes On HomeworkDocument19 pagesNotes On HomeworkMrSomnambululNo ratings yet
- Applications of Chitin and Chitosan in Industry and Medical Science: A ReviewDocument6 pagesApplications of Chitin and Chitosan in Industry and Medical Science: A ReviewMrSomnambululNo ratings yet
- Chitosan: Kimberly Novak, Melanie Johns Cupp, and Timothy S. TracyDocument9 pagesChitosan: Kimberly Novak, Melanie Johns Cupp, and Timothy S. TracyMrSomnambululNo ratings yet
- Chapter 9 Subtract Ive MixingDocument19 pagesChapter 9 Subtract Ive MixingMrSomnambululNo ratings yet
- Chapter 9: Color Additive Primary ColorsDocument19 pagesChapter 9: Color Additive Primary ColorsMrSomnambululNo ratings yet
- Course Info: Dr. Ellen KeisterDocument14 pagesCourse Info: Dr. Ellen KeisterMrSomnambululNo ratings yet
- Chapter 7 Receptive Fields 2Document18 pagesChapter 7 Receptive Fields 2MrSomnambululNo ratings yet
- Chapter 5 EyeDocument14 pagesChapter 5 EyeMrSomnambululNo ratings yet
- Chapter 4: Cameras and Photography: - Depth of Field - ExposureDocument21 pagesChapter 4: Cameras and Photography: - Depth of Field - ExposureMrSomnambululNo ratings yet
- Homework Policies: - Molly: Tuesdays 2-4pm - Dr. Keister: Wednesdays 10am-12 - Prof. Goldman: Wednesdays 2-3:30pmDocument14 pagesHomework Policies: - Molly: Tuesdays 2-4pm - Dr. Keister: Wednesdays 10am-12 - Prof. Goldman: Wednesdays 2-3:30pmMrSomnambululNo ratings yet
- L 10 BalanceDocument11 pagesL 10 BalanceMrSomnambululNo ratings yet
- The Physiology of The Senses - Touch, Pain, Taste and SmellDocument20 pagesThe Physiology of The Senses - Touch, Pain, Taste and SmellMrSomnambululNo ratings yet
- 12taste and SmellDocument19 pages12taste and SmellMrSomnambululNo ratings yet
- Faith To Go ForwardDocument10 pagesFaith To Go ForwardAlejandro DominguezNo ratings yet
- EULAR RecommendationsDocument13 pagesEULAR RecommendationsAmer Wasim100% (1)
- Daftar Harga Tiap PBFDocument4 pagesDaftar Harga Tiap PBFPraja Setia NingsihNo ratings yet
- Patofisiologi HematuriaDocument10 pagesPatofisiologi HematuriaNurunSalamanNo ratings yet
- College of NursingDocument1 pageCollege of NursingJohn Michael Manlupig PitoyNo ratings yet
- Laboratory and Diagnostic ExaminationDocument3 pagesLaboratory and Diagnostic ExaminationRose Anne MücklNo ratings yet
- CVS - Charts & DiagramsDocument20 pagesCVS - Charts & DiagramsMamathaNo ratings yet
- Opioid SpeechDocument3 pagesOpioid Speechapi-267758642No ratings yet
- Bahan Tutor Skenario 3Document5 pagesBahan Tutor Skenario 3Azka MuflihaNo ratings yet
- Hospital Literature StudyDocument52 pagesHospital Literature Studylakshma reddyNo ratings yet
- Oral Motor ExercisesDocument7 pagesOral Motor Exercisesmeh wish100% (5)
- Acute Respiratory Distress Syndrome - Background, Pathophysiology, EtiologyDocument5 pagesAcute Respiratory Distress Syndrome - Background, Pathophysiology, EtiologyARHNo ratings yet
- 40 Normal Labor and DystociaDocument47 pages40 Normal Labor and DystociaCitra Wulandari SofyanNo ratings yet
- Soft Tissue Infection by SlidesgoDocument40 pagesSoft Tissue Infection by SlidesgoDurga MadhuriNo ratings yet
- PedsCases CF Note (SP Edit)Document1 pagePedsCases CF Note (SP Edit)Mehtab AlamNo ratings yet
- Thyroid Function Tests: What Is The Thyroid Gland?Document2 pagesThyroid Function Tests: What Is The Thyroid Gland?rastamaneazy269No ratings yet
- Dabur Product PortfolioDocument18 pagesDabur Product PortfolioAshutosh SamantNo ratings yet
- Pathophysiology of Myocardial Infarction (STEMI)Document2 pagesPathophysiology of Myocardial Infarction (STEMI)michaela100% (3)
- Photo EssayDocument13 pagesPhoto Essayapi-314854412No ratings yet
- MCL FormatDocument49 pagesMCL Formatasheesh kumarNo ratings yet
- Valvular Heart Disease: Bekele T. (MD)Document47 pagesValvular Heart Disease: Bekele T. (MD)alehegn beleteNo ratings yet
- Applications of EnzymesDocument9 pagesApplications of EnzymesRabia HussainNo ratings yet
- Case Presentation 2Document135 pagesCase Presentation 2Muhammad AliNo ratings yet
- Gastrointestinal Tract System NotesDocument8 pagesGastrointestinal Tract System NotesCarl Elexer Cuyugan Ano100% (1)
- Algoritma StatinDocument1 pageAlgoritma StatinAgnes Irene ZagotoNo ratings yet
- Danger Signs During Pregnancy 4 1Document33 pagesDanger Signs During Pregnancy 4 1Precious Maslang PadawilNo ratings yet