
Heroin: Health Hazards
Heroin: Health Hazards
You might also like
- Types of Drugs and Their Effects PDFDocument28 pagesTypes of Drugs and Their Effects PDFAnonymous hF5zAdvwCC50% (2)
- Muslim Rajputs of RajouriDocument10 pagesMuslim Rajputs of RajouriEPILOGUE MAGAZINE100% (2)
- The Gods of Greece PDFDocument224 pagesThe Gods of Greece PDFCiro Formicola100% (2)
- Offshore Engineer-February 2015Document84 pagesOffshore Engineer-February 2015ilkerkozturk100% (2)
- 2 Material HandlingDocument218 pages2 Material HandlingJon Blac100% (1)
- Heroin - Infofacts - NidaDocument5 pagesHeroin - Infofacts - NidaLee GaylordNo ratings yet
- Heroina - EnglezaDocument3 pagesHeroina - EnglezaLylyshor LylyNo ratings yet
- Downloaded From FILIPINO NURSES CENTRALDocument13 pagesDownloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralNo ratings yet
- Heroin: Ashlee SartoriDocument20 pagesHeroin: Ashlee Sartoriapi-302578196No ratings yet
- West Chester University of Pennsylvania's Opioid Education Webinar Series - September 2020Document22 pagesWest Chester University of Pennsylvania's Opioid Education Webinar Series - September 2020WCU-PsychologyNo ratings yet
- Heroin Research ReportDocument16 pagesHeroin Research ReportAbas Njarkhatir100% (1)
- Heroin: Research Report SeriesDocument8 pagesHeroin: Research Report SerieswaterprincessNo ratings yet
- Opioid Management 2Document31 pagesOpioid Management 2Susan RashidNo ratings yet
- CHAPTER 53 OpiatesDocument15 pagesCHAPTER 53 OpiatesSusan RashidNo ratings yet
- RRHeroinDocument8 pagesRRHeroinlosangelesNo ratings yet
- Dangerous Drug InteractionsDocument27 pagesDangerous Drug InteractionsriniambarwatiNo ratings yet
- Buprenorphine Maintenance: A New Treatment For Opioid DependenceDocument7 pagesBuprenorphine Maintenance: A New Treatment For Opioid DependenceFaza1006No ratings yet
- National Drug Court Institute: Fact SheetDocument4 pagesNational Drug Court Institute: Fact SheetMistor Dupois WilliamsNo ratings yet
- Bupren4 PDFDocument12 pagesBupren4 PDFPatrick Michael PerezNo ratings yet
- Narcotics: (Opioids)Document32 pagesNarcotics: (Opioids)Roman MamunNo ratings yet
- Drug Abuse Among The Students PDFDocument7 pagesDrug Abuse Among The Students PDFTed MosbyNo ratings yet
- Circulatorio y Óseo MicrobiologiaDocument13 pagesCirculatorio y Óseo MicrobiologiaLinaMejiaNo ratings yet
- Drug Abuse Among The Students: June 2015Document8 pagesDrug Abuse Among The Students: June 2015deependra kumar100% (1)
- Medications To Treat Opioid Use Disorder Research ReportDocument34 pagesMedications To Treat Opioid Use Disorder Research ReportBakthika KumarageNo ratings yet
- Health Promotion Paper - Amanda NorthDocument13 pagesHealth Promotion Paper - Amanda Northapi-351310106No ratings yet
- Fischer, Rehm, Kirst Et AlDocument7 pagesFischer, Rehm, Kirst Et AlCraig Patrich AshtonNo ratings yet
- Federal Research Efforts On AddictionDocument50 pagesFederal Research Efforts On AddictionNational Press FoundationNo ratings yet
- Community Drug Alert: Prescription DrugsDocument4 pagesCommunity Drug Alert: Prescription DrugslosangelesNo ratings yet
- Comprehensive Drug Education and Vice Control - 075640Document46 pagesComprehensive Drug Education and Vice Control - 075640Gerome DariaNo ratings yet
- Guidelines+ +Opioids+ChapterDocument16 pagesGuidelines+ +Opioids+ChapterRajinder Kumar BassanNo ratings yet
- Opioid Withdrawal in AdolescentsDocument21 pagesOpioid Withdrawal in Adolescentsmayteveronica1000No ratings yet
- Research PaperDocument10 pagesResearch Paperapi-339029088100% (1)
- Harm Reduction: Shifting From A War On Drugs To A War On Drug Related DeathsDocument20 pagesHarm Reduction: Shifting From A War On Drugs To A War On Drug Related DeathsCato InstituteNo ratings yet
- Substance Use DisorderDocument13 pagesSubstance Use Disorderapi-591817398No ratings yet
- HIV and Substance Use: Hiv Mental Health Treatment IssuesDocument2 pagesHIV and Substance Use: Hiv Mental Health Treatment IssuesClave T DanielsNo ratings yet
- MARIHUANADocument2 pagesMARIHUANAPiya FernandezNo ratings yet
- Policybrief EffectivetreatmentsDocument2 pagesPolicybrief EffectivetreatmentsMaritsa EngelbrechtNo ratings yet
- Drug AddictionDocument23 pagesDrug AddictionsjvNo ratings yet
- Methods of Detoxification and Their Role in Treating Patients With Opioid DependenceDocument3 pagesMethods of Detoxification and Their Role in Treating Patients With Opioid DependenceAndy PurnomoNo ratings yet
- Subutex Quick-Start-GuideDocument6 pagesSubutex Quick-Start-GuideDanNo ratings yet
- Hassan Project Orginal 11Document90 pagesHassan Project Orginal 11michaelduru027No ratings yet
- Narcotics Types AssignmentDocument10 pagesNarcotics Types AssignmentUsamakhan009No ratings yet
- Artikel - Filippini Anestesia para Pacinete Scon Drogas IlicitasDocument10 pagesArtikel - Filippini Anestesia para Pacinete Scon Drogas IlicitasAndresPimentelAlvarezNo ratings yet
- Drug Abuse 3Document3 pagesDrug Abuse 3Aldora OktavianaNo ratings yet
- Am J Public Health 1999 p662Document4 pagesAm J Public Health 1999 p662Handris SupriadiNo ratings yet
- RX DrugsDocument39 pagesRX Drugstesfayesisay990No ratings yet
- OutDocument9 pagesOutAsyifaRizkiNo ratings yet
- DOG (Drugs of Abuse)Document6 pagesDOG (Drugs of Abuse)Faith G. FloresNo ratings yet
- Heroin FactsDocument6 pagesHeroin FactsRobert ClarkNo ratings yet
- Bja Substance Abuse in AnaesthesistDocument6 pagesBja Substance Abuse in AnaesthesistaleizaNo ratings yet
- Final Literary ReviewDocument19 pagesFinal Literary ReviewrojorakheeNo ratings yet
- Heroin Addiction in Albuquerque 2014Document8 pagesHeroin Addiction in Albuquerque 2014api-247762674No ratings yet
- 2018 - Prevention and Treatment of Opioid Misuse and Addiction A ReviewDocument9 pages2018 - Prevention and Treatment of Opioid Misuse and Addiction A ReviewÂngela MarreiroNo ratings yet
- Drug Abuse Among The Students: June 2015Document8 pagesDrug Abuse Among The Students: June 2015Swati ShuklaNo ratings yet
- Meth 347Document18 pagesMeth 347Jeffry BoikeNo ratings yet
- 2014 CONTINUUM Neurologic Complications of Illicit Drug AbuseDocument15 pages2014 CONTINUUM Neurologic Complications of Illicit Drug AbuseKarl Jimenez SeparaNo ratings yet
- Preventing Overdose, Saving LivesDocument24 pagesPreventing Overdose, Saving Liveswebmaster@drugpolicy.orgNo ratings yet
- Non-Pcol TX For AddictionDocument9 pagesNon-Pcol TX For AddictionAdelyneNo ratings yet
- Note On Drug AbuseDocument2 pagesNote On Drug AbuseBabatunde JonathanNo ratings yet
- Silent KillerDocument12 pagesSilent KillerMike MaybayNo ratings yet
- Prescription Painkillers: History, Pharmacology, and TreatmentFrom EverandPrescription Painkillers: History, Pharmacology, and TreatmentNo ratings yet
- Omb Bulletin No. 06-01Document2 pagesOmb Bulletin No. 06-01losangeles100% (1)
- 02359-b04-03 AppendixDocument146 pages02359-b04-03 AppendixlosangelesNo ratings yet
- 02360-b04-03 AttachmentDocument5 pages02360-b04-03 AttachmentlosangelesNo ratings yet
- Executive Office of The President: Attachment BDocument5 pagesExecutive Office of The President: Attachment Blosangeles100% (1)
- 02368-b06-01 CorrectionDocument1 page02368-b06-01 Correctionlosangeles100% (1)
- 02358-b04-02 Supp1Document7 pages02358-b04-02 Supp1losangelesNo ratings yet
- Executive Office of The President Executive Office of The PresidentDocument4 pagesExecutive Office of The President Executive Office of The Presidentlosangeles100% (1)
- Executive Office of The PresidentDocument23 pagesExecutive Office of The Presidentlosangeles100% (1)
- b04 04Document16 pagesb04 04losangeles100% (1)
- Executive Office of The President Executive Office of The PresidentDocument13 pagesExecutive Office of The President Executive Office of The Presidentlosangeles100% (1)
- 02352-b03-04 AttachDocument141 pages02352-b03-04 AttachlosangelesNo ratings yet
- Executive Office of The President: What Are The Legal Authorities Under Which OMB Is Requiring Agency Action?Document3 pagesExecutive Office of The President: What Are The Legal Authorities Under Which OMB Is Requiring Agency Action?losangelesNo ratings yet
- SpecDocument424 pagesSpeclosangelesNo ratings yet
- Attachment BDocument4 pagesAttachment BlosangelesNo ratings yet
- Executive Office of The President Executive Office of The PresidentDocument5 pagesExecutive Office of The President Executive Office of The PresidentlosangelesNo ratings yet
- Major Savings and Reforms in The President's 2008 Budget: EbruaryDocument211 pagesMajor Savings and Reforms in The President's 2008 Budget: EbruarylosangelesNo ratings yet
- Executive Office of The PresidentDocument20 pagesExecutive Office of The PresidentlosangelesNo ratings yet
- 02338-Expanding Egov 2005Document12 pages02338-Expanding Egov 2005losangelesNo ratings yet
- Bulletin No. 00 - 03 To The Heads of Executive Departments and Establishments SubjectDocument13 pagesBulletin No. 00 - 03 To The Heads of Executive Departments and Establishments SubjectlosangelesNo ratings yet
- Object Class Analysis: Budget of The U.S. GovernmentDocument128 pagesObject Class Analysis: Budget of The U.S. GovernmentlosangelesNo ratings yet
- Department of Transportation: Since 2001, The AdministrationDocument5 pagesDepartment of Transportation: Since 2001, The AdministrationlosangelesNo ratings yet
- Director Rob Portman February 5, 2007Document8 pagesDirector Rob Portman February 5, 2007losangelesNo ratings yet
- Program Assessment Rating Tool (PART) 2008 Budget: This PDF Is Also Available in Excel Format atDocument31 pagesProgram Assessment Rating Tool (PART) 2008 Budget: This PDF Is Also Available in Excel Format atlosangelesNo ratings yet
- TreasuryDocument4 pagesTreasurylosangelesNo ratings yet
- HistDocument336 pagesHistlosangeles100% (1)
- SDL Atlas Catalog 23 2015Document150 pagesSDL Atlas Catalog 23 2015Tahir NizamNo ratings yet
- Final Management Project On Geo TVDocument35 pagesFinal Management Project On Geo TVAli Malik100% (1)
- Chapter 2: Decision MakingDocument16 pagesChapter 2: Decision Makingafzal_aNo ratings yet
- A Conversation Explaining BiomimicryDocument6 pagesA Conversation Explaining Biomimicryapi-3703075100% (2)
- Steering System (Notes On Tom)Document8 pagesSteering System (Notes On Tom)Vaibhav Vithoba Naik100% (1)
- Atharva Vediya Gopala-Tapani Upanishad KRISHNA PrayersDocument3 pagesAtharva Vediya Gopala-Tapani Upanishad KRISHNA PrayersТимур ГнедовскийNo ratings yet
- Annexure-10b) MA5620 & MA5626 Product Description PDFDocument52 pagesAnnexure-10b) MA5620 & MA5626 Product Description PDFFares DamNo ratings yet
- Nucleic Acid Metabolism Adapted From Zhihong Li Material - May 2024Document79 pagesNucleic Acid Metabolism Adapted From Zhihong Li Material - May 2024Black RavenoidNo ratings yet
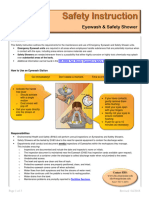
- Eyewash and Safety Shower SiDocument3 pagesEyewash and Safety Shower SiAli EsmaeilbeygiNo ratings yet
- SAS Macro Tutorial ImpDocument27 pagesSAS Macro Tutorial ImpArijit DasNo ratings yet
- PEER Report On MS ESA ProgramDocument69 pagesPEER Report On MS ESA ProgramRuss LatinoNo ratings yet
- Steamshovel Press Issue 04Document60 pagesSteamshovel Press Issue 04liondog1No ratings yet
- Day 2UNQ3-1.docx..bakDocument13 pagesDay 2UNQ3-1.docx..bakAurellia Shafitri100% (1)
- CFP Registration Process (Final) - 3Document39 pagesCFP Registration Process (Final) - 3nishiNo ratings yet
- Abhinavagupta (C. 950 - 1016 CEDocument8 pagesAbhinavagupta (C. 950 - 1016 CEthewitness3No ratings yet
- How Do Homes Provide Safe ShelterDocument10 pagesHow Do Homes Provide Safe ShelterInda KusumawatiNo ratings yet
- Philosophical Issues in TourismDocument2 pagesPhilosophical Issues in TourismLana Talita100% (1)
- English For Nursing Topic 12 Reinforcing A Dietary ProgramDocument6 pagesEnglish For Nursing Topic 12 Reinforcing A Dietary ProgramEha Huwaida HayatiNo ratings yet
- Invented EdensDocument201 pagesInvented EdensLeslie López100% (3)
- FG StackDocument15 pagesFG StackTahir Sapsal100% (1)
- Monitoring Times 1998 03Document116 pagesMonitoring Times 1998 03Benjamin DoverNo ratings yet
- Law and IT Assignment SEM IXDocument18 pagesLaw and IT Assignment SEM IXrenu tomarNo ratings yet
- Panadent SystemDocument70 pagesPanadent SystemDhananjay GandageNo ratings yet
- Light Sport Aircraft: Standard Terminology ForDocument6 pagesLight Sport Aircraft: Standard Terminology ForAhmad Zubair RasulyNo ratings yet
- Tve 8 Shielded Metal Arc WeldingDocument11 pagesTve 8 Shielded Metal Arc WeldingJOHN ALFRED MANANGGITNo ratings yet
- Mesina V Meer PDFDocument3 pagesMesina V Meer PDFColee StiflerNo ratings yet
















































































































Download as pdf or txt
You might also like
- Types of Drugs and Their Effects PDFDocument28 pagesTypes of Drugs and Their Effects PDFAnonymous hF5zAdvwCC50% (2)
- Muslim Rajputs of RajouriDocument10 pagesMuslim Rajputs of RajouriEPILOGUE MAGAZINE100% (2)
- The Gods of Greece PDFDocument224 pagesThe Gods of Greece PDFCiro Formicola100% (2)
- Offshore Engineer-February 2015Document84 pagesOffshore Engineer-February 2015ilkerkozturk100% (2)
- 2 Material HandlingDocument218 pages2 Material HandlingJon Blac100% (1)
- Heroin - Infofacts - NidaDocument5 pagesHeroin - Infofacts - NidaLee GaylordNo ratings yet
- Heroina - EnglezaDocument3 pagesHeroina - EnglezaLylyshor LylyNo ratings yet
- Downloaded From FILIPINO NURSES CENTRALDocument13 pagesDownloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralNo ratings yet
- Heroin: Ashlee SartoriDocument20 pagesHeroin: Ashlee Sartoriapi-302578196No ratings yet
- West Chester University of Pennsylvania's Opioid Education Webinar Series - September 2020Document22 pagesWest Chester University of Pennsylvania's Opioid Education Webinar Series - September 2020WCU-PsychologyNo ratings yet
- Heroin Research ReportDocument16 pagesHeroin Research ReportAbas Njarkhatir100% (1)
- Heroin: Research Report SeriesDocument8 pagesHeroin: Research Report SerieswaterprincessNo ratings yet
- Opioid Management 2Document31 pagesOpioid Management 2Susan RashidNo ratings yet
- CHAPTER 53 OpiatesDocument15 pagesCHAPTER 53 OpiatesSusan RashidNo ratings yet
- RRHeroinDocument8 pagesRRHeroinlosangelesNo ratings yet
- Dangerous Drug InteractionsDocument27 pagesDangerous Drug InteractionsriniambarwatiNo ratings yet
- Buprenorphine Maintenance: A New Treatment For Opioid DependenceDocument7 pagesBuprenorphine Maintenance: A New Treatment For Opioid DependenceFaza1006No ratings yet
- National Drug Court Institute: Fact SheetDocument4 pagesNational Drug Court Institute: Fact SheetMistor Dupois WilliamsNo ratings yet
- Bupren4 PDFDocument12 pagesBupren4 PDFPatrick Michael PerezNo ratings yet
- Narcotics: (Opioids)Document32 pagesNarcotics: (Opioids)Roman MamunNo ratings yet
- Drug Abuse Among The Students PDFDocument7 pagesDrug Abuse Among The Students PDFTed MosbyNo ratings yet
- Circulatorio y Óseo MicrobiologiaDocument13 pagesCirculatorio y Óseo MicrobiologiaLinaMejiaNo ratings yet
- Drug Abuse Among The Students: June 2015Document8 pagesDrug Abuse Among The Students: June 2015deependra kumar100% (1)
- Medications To Treat Opioid Use Disorder Research ReportDocument34 pagesMedications To Treat Opioid Use Disorder Research ReportBakthika KumarageNo ratings yet
- Health Promotion Paper - Amanda NorthDocument13 pagesHealth Promotion Paper - Amanda Northapi-351310106No ratings yet
- Fischer, Rehm, Kirst Et AlDocument7 pagesFischer, Rehm, Kirst Et AlCraig Patrich AshtonNo ratings yet
- Federal Research Efforts On AddictionDocument50 pagesFederal Research Efforts On AddictionNational Press FoundationNo ratings yet
- Community Drug Alert: Prescription DrugsDocument4 pagesCommunity Drug Alert: Prescription DrugslosangelesNo ratings yet
- Comprehensive Drug Education and Vice Control - 075640Document46 pagesComprehensive Drug Education and Vice Control - 075640Gerome DariaNo ratings yet
- Guidelines+ +Opioids+ChapterDocument16 pagesGuidelines+ +Opioids+ChapterRajinder Kumar BassanNo ratings yet
- Opioid Withdrawal in AdolescentsDocument21 pagesOpioid Withdrawal in Adolescentsmayteveronica1000No ratings yet
- Research PaperDocument10 pagesResearch Paperapi-339029088100% (1)
- Harm Reduction: Shifting From A War On Drugs To A War On Drug Related DeathsDocument20 pagesHarm Reduction: Shifting From A War On Drugs To A War On Drug Related DeathsCato InstituteNo ratings yet
- Substance Use DisorderDocument13 pagesSubstance Use Disorderapi-591817398No ratings yet
- HIV and Substance Use: Hiv Mental Health Treatment IssuesDocument2 pagesHIV and Substance Use: Hiv Mental Health Treatment IssuesClave T DanielsNo ratings yet
- MARIHUANADocument2 pagesMARIHUANAPiya FernandezNo ratings yet
- Policybrief EffectivetreatmentsDocument2 pagesPolicybrief EffectivetreatmentsMaritsa EngelbrechtNo ratings yet
- Drug AddictionDocument23 pagesDrug AddictionsjvNo ratings yet
- Methods of Detoxification and Their Role in Treating Patients With Opioid DependenceDocument3 pagesMethods of Detoxification and Their Role in Treating Patients With Opioid DependenceAndy PurnomoNo ratings yet
- Subutex Quick-Start-GuideDocument6 pagesSubutex Quick-Start-GuideDanNo ratings yet
- Hassan Project Orginal 11Document90 pagesHassan Project Orginal 11michaelduru027No ratings yet
- Narcotics Types AssignmentDocument10 pagesNarcotics Types AssignmentUsamakhan009No ratings yet
- Artikel - Filippini Anestesia para Pacinete Scon Drogas IlicitasDocument10 pagesArtikel - Filippini Anestesia para Pacinete Scon Drogas IlicitasAndresPimentelAlvarezNo ratings yet
- Drug Abuse 3Document3 pagesDrug Abuse 3Aldora OktavianaNo ratings yet
- Am J Public Health 1999 p662Document4 pagesAm J Public Health 1999 p662Handris SupriadiNo ratings yet
- RX DrugsDocument39 pagesRX Drugstesfayesisay990No ratings yet
- OutDocument9 pagesOutAsyifaRizkiNo ratings yet
- DOG (Drugs of Abuse)Document6 pagesDOG (Drugs of Abuse)Faith G. FloresNo ratings yet
- Heroin FactsDocument6 pagesHeroin FactsRobert ClarkNo ratings yet
- Bja Substance Abuse in AnaesthesistDocument6 pagesBja Substance Abuse in AnaesthesistaleizaNo ratings yet
- Final Literary ReviewDocument19 pagesFinal Literary ReviewrojorakheeNo ratings yet
- Heroin Addiction in Albuquerque 2014Document8 pagesHeroin Addiction in Albuquerque 2014api-247762674No ratings yet
- 2018 - Prevention and Treatment of Opioid Misuse and Addiction A ReviewDocument9 pages2018 - Prevention and Treatment of Opioid Misuse and Addiction A ReviewÂngela MarreiroNo ratings yet
- Drug Abuse Among The Students: June 2015Document8 pagesDrug Abuse Among The Students: June 2015Swati ShuklaNo ratings yet
- Meth 347Document18 pagesMeth 347Jeffry BoikeNo ratings yet
- 2014 CONTINUUM Neurologic Complications of Illicit Drug AbuseDocument15 pages2014 CONTINUUM Neurologic Complications of Illicit Drug AbuseKarl Jimenez SeparaNo ratings yet
- Preventing Overdose, Saving LivesDocument24 pagesPreventing Overdose, Saving Liveswebmaster@drugpolicy.orgNo ratings yet
- Non-Pcol TX For AddictionDocument9 pagesNon-Pcol TX For AddictionAdelyneNo ratings yet
- Note On Drug AbuseDocument2 pagesNote On Drug AbuseBabatunde JonathanNo ratings yet
- Silent KillerDocument12 pagesSilent KillerMike MaybayNo ratings yet
- Prescription Painkillers: History, Pharmacology, and TreatmentFrom EverandPrescription Painkillers: History, Pharmacology, and TreatmentNo ratings yet
- Omb Bulletin No. 06-01Document2 pagesOmb Bulletin No. 06-01losangeles100% (1)
- 02359-b04-03 AppendixDocument146 pages02359-b04-03 AppendixlosangelesNo ratings yet
- 02360-b04-03 AttachmentDocument5 pages02360-b04-03 AttachmentlosangelesNo ratings yet
- Executive Office of The President: Attachment BDocument5 pagesExecutive Office of The President: Attachment Blosangeles100% (1)
- 02368-b06-01 CorrectionDocument1 page02368-b06-01 Correctionlosangeles100% (1)
- 02358-b04-02 Supp1Document7 pages02358-b04-02 Supp1losangelesNo ratings yet
- Executive Office of The President Executive Office of The PresidentDocument4 pagesExecutive Office of The President Executive Office of The Presidentlosangeles100% (1)
- Executive Office of The PresidentDocument23 pagesExecutive Office of The Presidentlosangeles100% (1)
- b04 04Document16 pagesb04 04losangeles100% (1)
- Executive Office of The President Executive Office of The PresidentDocument13 pagesExecutive Office of The President Executive Office of The Presidentlosangeles100% (1)
- 02352-b03-04 AttachDocument141 pages02352-b03-04 AttachlosangelesNo ratings yet
- Executive Office of The President: What Are The Legal Authorities Under Which OMB Is Requiring Agency Action?Document3 pagesExecutive Office of The President: What Are The Legal Authorities Under Which OMB Is Requiring Agency Action?losangelesNo ratings yet
- SpecDocument424 pagesSpeclosangelesNo ratings yet
- Attachment BDocument4 pagesAttachment BlosangelesNo ratings yet
- Executive Office of The President Executive Office of The PresidentDocument5 pagesExecutive Office of The President Executive Office of The PresidentlosangelesNo ratings yet
- Major Savings and Reforms in The President's 2008 Budget: EbruaryDocument211 pagesMajor Savings and Reforms in The President's 2008 Budget: EbruarylosangelesNo ratings yet
- Executive Office of The PresidentDocument20 pagesExecutive Office of The PresidentlosangelesNo ratings yet
- 02338-Expanding Egov 2005Document12 pages02338-Expanding Egov 2005losangelesNo ratings yet
- Bulletin No. 00 - 03 To The Heads of Executive Departments and Establishments SubjectDocument13 pagesBulletin No. 00 - 03 To The Heads of Executive Departments and Establishments SubjectlosangelesNo ratings yet
- Object Class Analysis: Budget of The U.S. GovernmentDocument128 pagesObject Class Analysis: Budget of The U.S. GovernmentlosangelesNo ratings yet
- Department of Transportation: Since 2001, The AdministrationDocument5 pagesDepartment of Transportation: Since 2001, The AdministrationlosangelesNo ratings yet
- Director Rob Portman February 5, 2007Document8 pagesDirector Rob Portman February 5, 2007losangelesNo ratings yet
- Program Assessment Rating Tool (PART) 2008 Budget: This PDF Is Also Available in Excel Format atDocument31 pagesProgram Assessment Rating Tool (PART) 2008 Budget: This PDF Is Also Available in Excel Format atlosangelesNo ratings yet
- TreasuryDocument4 pagesTreasurylosangelesNo ratings yet
- HistDocument336 pagesHistlosangeles100% (1)
- SDL Atlas Catalog 23 2015Document150 pagesSDL Atlas Catalog 23 2015Tahir NizamNo ratings yet
- Final Management Project On Geo TVDocument35 pagesFinal Management Project On Geo TVAli Malik100% (1)
- Chapter 2: Decision MakingDocument16 pagesChapter 2: Decision Makingafzal_aNo ratings yet
- A Conversation Explaining BiomimicryDocument6 pagesA Conversation Explaining Biomimicryapi-3703075100% (2)
- Steering System (Notes On Tom)Document8 pagesSteering System (Notes On Tom)Vaibhav Vithoba Naik100% (1)
- Atharva Vediya Gopala-Tapani Upanishad KRISHNA PrayersDocument3 pagesAtharva Vediya Gopala-Tapani Upanishad KRISHNA PrayersТимур ГнедовскийNo ratings yet
- Annexure-10b) MA5620 & MA5626 Product Description PDFDocument52 pagesAnnexure-10b) MA5620 & MA5626 Product Description PDFFares DamNo ratings yet
- Nucleic Acid Metabolism Adapted From Zhihong Li Material - May 2024Document79 pagesNucleic Acid Metabolism Adapted From Zhihong Li Material - May 2024Black RavenoidNo ratings yet
- Eyewash and Safety Shower SiDocument3 pagesEyewash and Safety Shower SiAli EsmaeilbeygiNo ratings yet
- SAS Macro Tutorial ImpDocument27 pagesSAS Macro Tutorial ImpArijit DasNo ratings yet
- PEER Report On MS ESA ProgramDocument69 pagesPEER Report On MS ESA ProgramRuss LatinoNo ratings yet
- Steamshovel Press Issue 04Document60 pagesSteamshovel Press Issue 04liondog1No ratings yet
- Day 2UNQ3-1.docx..bakDocument13 pagesDay 2UNQ3-1.docx..bakAurellia Shafitri100% (1)
- CFP Registration Process (Final) - 3Document39 pagesCFP Registration Process (Final) - 3nishiNo ratings yet
- Abhinavagupta (C. 950 - 1016 CEDocument8 pagesAbhinavagupta (C. 950 - 1016 CEthewitness3No ratings yet
- How Do Homes Provide Safe ShelterDocument10 pagesHow Do Homes Provide Safe ShelterInda KusumawatiNo ratings yet
- Philosophical Issues in TourismDocument2 pagesPhilosophical Issues in TourismLana Talita100% (1)
- English For Nursing Topic 12 Reinforcing A Dietary ProgramDocument6 pagesEnglish For Nursing Topic 12 Reinforcing A Dietary ProgramEha Huwaida HayatiNo ratings yet
- Invented EdensDocument201 pagesInvented EdensLeslie López100% (3)
- FG StackDocument15 pagesFG StackTahir Sapsal100% (1)
- Monitoring Times 1998 03Document116 pagesMonitoring Times 1998 03Benjamin DoverNo ratings yet
- Law and IT Assignment SEM IXDocument18 pagesLaw and IT Assignment SEM IXrenu tomarNo ratings yet
- Panadent SystemDocument70 pagesPanadent SystemDhananjay GandageNo ratings yet
- Light Sport Aircraft: Standard Terminology ForDocument6 pagesLight Sport Aircraft: Standard Terminology ForAhmad Zubair RasulyNo ratings yet
- Tve 8 Shielded Metal Arc WeldingDocument11 pagesTve 8 Shielded Metal Arc WeldingJOHN ALFRED MANANGGITNo ratings yet
- Mesina V Meer PDFDocument3 pagesMesina V Meer PDFColee StiflerNo ratings yet