Download as docx, pdf, or txt
You might also like
- McKay Moore Sohlberg Justine Hamilton Lyn S. Turkstra Transforming Cognitive Rehabilitation - Effective Instructional Methods The Guilford Press 2022 X3qkyyDocument355 pagesMcKay Moore Sohlberg Justine Hamilton Lyn S. Turkstra Transforming Cognitive Rehabilitation - Effective Instructional Methods The Guilford Press 2022 X3qkyyerfan.izadpanahNo ratings yet
- Medical Terminology Pre TestDocument4 pagesMedical Terminology Pre TestJo Hn Vengz100% (2)
- Alexanders Care of The Patient in Surgery Rothrock 16th Edition Test BankDocument9 pagesAlexanders Care of The Patient in Surgery Rothrock 16th Edition Test Bankjoshuabakergpctsonbwj100% (41)
- Elm DGPDocument14 pagesElm DGPJo Hn VengzNo ratings yet
- Chapter 132 Total Penectomy. Hinman. 4th Ed. 2017Document3 pagesChapter 132 Total Penectomy. Hinman. 4th Ed. 2017Urologi Juli100% (1)
- How Social Status Shapes Person Perception and Evaluation A Social Neuroscience PerspectiveDocument40 pagesHow Social Status Shapes Person Perception and Evaluation A Social Neuroscience Perspectivejosephalbert3141592gmail.comNo ratings yet
- Step-By-Step Guide - Minimally Invasive Lumbar Spine Decompression and Dural RepairDocument10 pagesStep-By-Step Guide - Minimally Invasive Lumbar Spine Decompression and Dural RepairPankaj Vatsa100% (1)
- Basic Principles in Management of Patients With Maxillofacial InjuriesDocument11 pagesBasic Principles in Management of Patients With Maxillofacial InjuriesVishnu S PattathNo ratings yet
- Medical Terminology Post TestDocument4 pagesMedical Terminology Post TestJo Hn Vengz100% (1)
- CHN RatioDocument8 pagesCHN RatioJo Hn VengzNo ratings yet
- SssDocument5 pagesSssDerianti NurhidayahNo ratings yet
- Hemorrhoidectomy ManuscriptDocument5 pagesHemorrhoidectomy ManuscriptMa. Ydela MeradoresNo ratings yet
- Care in The Operating RoomDocument24 pagesCare in The Operating Roomjohn.berensonNo ratings yet
- SS 2015052610553699 PDFDocument7 pagesSS 2015052610553699 PDFLeny MeiriyanaNo ratings yet
- FrenectomyDocument22 pagesFrenectomyPallav Ganatra100% (3)
- Intra-Operative Nursing 2Document10 pagesIntra-Operative Nursing 2gbongatNo ratings yet
- How I Do ItDocument13 pagesHow I Do ItvennyherlenapsNo ratings yet
- Case Study HemorrhoidsDocument4 pagesCase Study HemorrhoidsTeanu Jose Gabrillo TamayoNo ratings yet
- HemorrhoidsDocument10 pagesHemorrhoidsTazkiyatul Asma'iNo ratings yet
- 6 Surgical Periodontal TherapyDocument38 pages6 Surgical Periodontal TherapyPriya SargunanNo ratings yet
- SkinGrafting-Rivera RobinDocument15 pagesSkinGrafting-Rivera RobinMonette Abalos MendovaNo ratings yet
- Skin Grafting ManuscriptDocument6 pagesSkin Grafting ManuscriptMa. Ydela MeradoresNo ratings yet
- Development of Hemorrhoids: Anal Canal AnatomyDocument20 pagesDevelopment of Hemorrhoids: Anal Canal AnatomyKris TejereroNo ratings yet
- Treatment of Nipple Hypertrophy by A Simplified Reduction TechniqueDocument7 pagesTreatment of Nipple Hypertrophy by A Simplified Reduction TechniqueАндрей ПетровNo ratings yet
- HemmorhoidectomyDocument3 pagesHemmorhoidectomyAbegail AbaygarNo ratings yet
- Difficulties in Lap HerniaDocument9 pagesDifficulties in Lap HerniarajeshNo ratings yet
- The Rectum and Anus: TrunkDocument11 pagesThe Rectum and Anus: TrunkAsish GeiorgeNo ratings yet
- College of Medicine Surgical Department: Basic Surgical Skills and AnastomosesDocument68 pagesCollege of Medicine Surgical Department: Basic Surgical Skills and AnastomosesDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Maxillectomy A ReviewDocument17 pagesMaxillectomy A ReviewDr. T. Balasubramanian100% (3)
- Adenoidectomy and Tosillectomy MethodsDocument5 pagesAdenoidectomy and Tosillectomy MethodsBkas GrgNo ratings yet
- Open HemorrhoidectomyDocument4 pagesOpen HemorrhoidectomyCaesar Rio Julyanto PutraNo ratings yet
- Becker 1959 Pre Operative and Post Operative Care of The Hemorrhoidectomy PatientDocument3 pagesBecker 1959 Pre Operative and Post Operative Care of The Hemorrhoidectomy PatientrumasadraunaNo ratings yet
- Maxilectomia TotalDocument18 pagesMaxilectomia TotalmonitosmaxilosNo ratings yet
- Module 6 - General SurgeryDocument18 pagesModule 6 - General Surgerysoft241No ratings yet
- Surgical Periodontal TherapyDocument37 pagesSurgical Periodontal Therapyperiodontics07No ratings yet
- Mucocele and Ranula Treatment & Management - Approach Considerations, Medical Care, Surgical CareDocument9 pagesMucocele and Ranula Treatment & Management - Approach Considerations, Medical Care, Surgical Careirshan HaniefNo ratings yet
- Inguinal Hernia - Yash PatodiaDocument12 pagesInguinal Hernia - Yash Patodiakhushisinghal.cse22No ratings yet
- General Principles of Periodontal SurgeryDocument20 pagesGeneral Principles of Periodontal SurgerysevattapillaiNo ratings yet
- Nephrectomy ProcedureDocument4 pagesNephrectomy ProcedureRon Java FantillanNo ratings yet
- Incision and DrainageDocument8 pagesIncision and DrainageAbraham ChiuNo ratings yet
- Dr. Zaid Surgical Phase-2Document39 pagesDr. Zaid Surgical Phase-2Abdelrahman GalalNo ratings yet
- Principles of Oral SurgeryDocument56 pagesPrinciples of Oral SurgeryJayeshNo ratings yet
- Abcesele Spațiilor SuperficialeDocument60 pagesAbcesele Spațiilor SuperficialeSalameh Abu MUSSANo ratings yet
- 5phase II Periodontal TherapyDocument54 pages5phase II Periodontal TherapyKaraz StudiosNo ratings yet
- 2 Clinicopathological Comparative Vs Surgical 2018Document6 pages2 Clinicopathological Comparative Vs Surgical 2018solikin ikinNo ratings yet
- Oral Surgery Lec. 9Document4 pagesOral Surgery Lec. 9Maysaa AbbasNo ratings yet
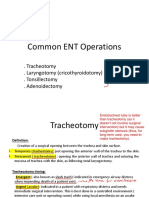
- 24 Common ENT OperationsDocument21 pages24 Common ENT OperationsMariam QaisNo ratings yet
- Or Write Up (Appendectomy) : Pines City Colleges College of NursingDocument9 pagesOr Write Up (Appendectomy) : Pines City Colleges College of Nursingthomasfinley44No ratings yet
- Surgery Instruments The Kiko Bridgewater DraftDocument237 pagesSurgery Instruments The Kiko Bridgewater DraftShandev IndoiNo ratings yet
- Surgical and Medical Emergencies UpDocument80 pagesSurgical and Medical Emergencies Upyvettefankam82No ratings yet
- Post Op Complication and ManagementDocument5 pagesPost Op Complication and ManagementElectricken21No ratings yet
- 4 Oral Cavity ProceduresDocument10 pages4 Oral Cavity ProceduresAnne MarieNo ratings yet
- Gingival CurettageDocument29 pagesGingival Curettagesahad100% (2)
- MedSurg RecitDocument3 pagesMedSurg RecitnicoleNo ratings yet
- Functional Endoscopic Sinus SurgeryDocument3 pagesFunctional Endoscopic Sinus SurgeryDanielicah CruzNo ratings yet
- Trephination For AcuteDocument3 pagesTrephination For AcuteDr.Ibrahim Al-QwizanyNo ratings yet
- Moult 2015Document7 pagesMoult 2015Amriansyah PranowoNo ratings yet
- Reasons For TonsillectomyDocument8 pagesReasons For TonsillectomyRasdumi100% (1)
- Incision & Drainage of Abscess Group 9 4bDocument5 pagesIncision & Drainage of Abscess Group 9 4bGUDISELA ramyaNo ratings yet
- Test Bank Alexanders Care of The Patient in Surgery 16th Edition Rothrock DownloadDocument9 pagesTest Bank Alexanders Care of The Patient in Surgery 16th Edition Rothrock Downloadlaurafloresejzawnptxr100% (32)
- Principles of Laparoscopic & Robotic Surgery: Aaquila Sherin Bismi J J Blessy OommanDocument46 pagesPrinciples of Laparoscopic & Robotic Surgery: Aaquila Sherin Bismi J J Blessy OommanAsif AbbasNo ratings yet
- Drainage Through Periodontal Pocket.: Acute AbscessDocument2 pagesDrainage Through Periodontal Pocket.: Acute AbscessShirmayne TangNo ratings yet
- Types of Sutures and Their IndicationsDocument6 pagesTypes of Sutures and Their IndicationsAdina BurciuNo ratings yet
- Case Studies of Postoperative Complications after Digestive SurgeryFrom EverandCase Studies of Postoperative Complications after Digestive SurgeryNo ratings yet
- Manual of Ambulatory General Surgery: A Step-by-Step Guide to Minor and Intermediate SurgeryFrom EverandManual of Ambulatory General Surgery: A Step-by-Step Guide to Minor and Intermediate SurgeryNo ratings yet
- Assessing The Ears and HearingDocument2 pagesAssessing The Ears and HearingJo Hn VengzNo ratings yet
- Assessing The Nose and SinusesDocument2 pagesAssessing The Nose and SinusesJo Hn VengzNo ratings yet
- Assessing The Eye Structures and Visual AcuityDocument4 pagesAssessing The Eye Structures and Visual AcuityJo Hn VengzNo ratings yet
- NPVDocument15 pagesNPVJo Hn Vengz100% (3)
- NLE Reading MaterialDocument99 pagesNLE Reading MaterialJo Hn Vengz100% (2)
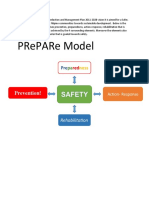
- Prepare ModelDocument1 pagePrepare ModelJo Hn VengzNo ratings yet
- NLE Reading MaterialDocument99 pagesNLE Reading MaterialJo Hn Vengz100% (1)
- Anatomy Booster HODocument59 pagesAnatomy Booster HOJo Hn VengzNo ratings yet
- FormatDocument3 pagesFormatJo Hn Vengz0% (1)
- VC ExamDocument16 pagesVC ExamJo Hn VengzNo ratings yet
- Handout UltrasoundDocument14 pagesHandout UltrasoundJo Hn VengzNo ratings yet
- BME 595 - Medical Imaging Applications Part 2: Introduction To Mri Fundamentals of Magnetic Resonance Feb. 16, 2005Document42 pagesBME 595 - Medical Imaging Applications Part 2: Introduction To Mri Fundamentals of Magnetic Resonance Feb. 16, 2005Jo Hn VengzNo ratings yet
- The Vertebal Column.Document259 pagesThe Vertebal Column.Jo Hn VengzNo ratings yet
- Chapter 1 Disasters: I.Typhoon/Hurricane/Cyclone Roger Pombo Sir HiquianaDocument2 pagesChapter 1 Disasters: I.Typhoon/Hurricane/Cyclone Roger Pombo Sir HiquianaJo Hn VengzNo ratings yet
- Cerebral Aerobics: Alveolar Process of The MaxillaDocument2 pagesCerebral Aerobics: Alveolar Process of The MaxillaJo Hn VengzNo ratings yet
- Cerebral Aerobics: and & LDocument2 pagesCerebral Aerobics: and & LJo Hn VengzNo ratings yet
- Child and Adolescent Development Prof - EdDocument8 pagesChild and Adolescent Development Prof - EdTin SottoNo ratings yet
- Be-Pandemic-Argues-Rsf? Fbclid Iwar0Pmj27Xhlbeouvb5Rnadh6Iwnudconng - Z - Wvjy3W Dhmnovdmnkplb6Nq Purpose of This GuideDocument27 pagesBe-Pandemic-Argues-Rsf? Fbclid Iwar0Pmj27Xhlbeouvb5Rnadh6Iwnudconng - Z - Wvjy3W Dhmnovdmnkplb6Nq Purpose of This GuideJo Hn VengzNo ratings yet
- Biological Science Reviewer 2Document20 pagesBiological Science Reviewer 2Jo Hn VengzNo ratings yet
- Immunology and SerologyDocument1 pageImmunology and SerologyJo Hn VengzNo ratings yet
- CHN RationDocument8 pagesCHN RationJo Hn VengzNo ratings yet
- CHN RationDocument8 pagesCHN RationJo Hn VengzNo ratings yet
- Community Health NursingDocument5 pagesCommunity Health NursingJo Hn VengzNo ratings yet
- Justification Letter For Classification of MDsDocument3 pagesJustification Letter For Classification of MDshitham shehataNo ratings yet
- 2010.hye Ee. Development of Banana Peel Jelly and Its Antioxidant and TexturalDocument2 pages2010.hye Ee. Development of Banana Peel Jelly and Its Antioxidant and TexturalAndi NursantiNo ratings yet
- Reaction Paper (Education For All)Document1 pageReaction Paper (Education For All)jonalyn obina100% (1)
- Ocb Recent Trends and DevelopmentsDocument14 pagesOcb Recent Trends and DevelopmentsPhilip BenoyNo ratings yet
- STUDENTS Lecture 4 (Chapter 3)Document19 pagesSTUDENTS Lecture 4 (Chapter 3)Sirine AjourNo ratings yet
- Erik Erikson Developmental TheoryDocument15 pagesErik Erikson Developmental TheoryFoday H KalokohNo ratings yet
- Up, Up in The Ladder of CARRERDocument17 pagesUp, Up in The Ladder of CARRERrolly curiaNo ratings yet
- Hubungan Tingkat Pengetahuan Dan Sikap Masyarakat Dengan Penanganan Awal Gigitan BinatangDocument11 pagesHubungan Tingkat Pengetahuan Dan Sikap Masyarakat Dengan Penanganan Awal Gigitan BinatangRisa FebriantiNo ratings yet
- 4.double Standard of MoralityDocument12 pages4.double Standard of MoralityIvy DumadaraNo ratings yet
- Complementary Therapies in Medicine: SciencedirectDocument6 pagesComplementary Therapies in Medicine: SciencedirectSurya Puji KusumaNo ratings yet
- Introduction To Home Economics LiteracyDocument19 pagesIntroduction To Home Economics LiteracyClarice Gavilan100% (1)
- Myocardial Infarction (Stemi) - Tennessee: Statpearls PublishingDocument3 pagesMyocardial Infarction (Stemi) - Tennessee: Statpearls PublishingMery AlizaNo ratings yet
- LESSON EXEMPLAR IN TleDocument2 pagesLESSON EXEMPLAR IN TleChe'che Inabangan Icawalo100% (3)
- Learning Outcomes Nutrition 1020 and The Omnivores DilemmaDocument3 pagesLearning Outcomes Nutrition 1020 and The Omnivores Dilemmaapi-302583687No ratings yet
- Narrative Review of The LiteratureDocument5 pagesNarrative Review of The Literature우즈무즈No ratings yet
- Standard For Dried Floral Parts: Cloves CXS 344-2021Document5 pagesStandard For Dried Floral Parts: Cloves CXS 344-2021KHALIDNo ratings yet
- Research Paper Sports PsychologyDocument7 pagesResearch Paper Sports Psychologygqsrcuplg100% (1)
- Notes On The Cult of Domesticity and WomanhoodDocument7 pagesNotes On The Cult of Domesticity and Womanhood2077 HQNo ratings yet
- 3i-Winsome (4) Print BukasDocument12 pages3i-Winsome (4) Print Bukasbea pegadNo ratings yet
- "Be Trained To Be The Best, Be Linked To Success": Bestlink College of The PhilippinesDocument12 pages"Be Trained To Be The Best, Be Linked To Success": Bestlink College of The PhilippinesAngelica Faye Aquino100% (1)
- Rojo PTS 7 - BARTENDING NCII CORE SESSION PLAN Configure ComputeDocument4 pagesRojo PTS 7 - BARTENDING NCII CORE SESSION PLAN Configure Computegillian marbebeNo ratings yet
- EyemaxxingDocument9 pagesEyemaxxingxzt899188018No ratings yet
- HSE Site Instruction For Contractor FormDocument2 pagesHSE Site Instruction For Contractor Formابو محمد علي100% (1)
- NCM 117-Sexual DisordersDocument7 pagesNCM 117-Sexual DisordersJa Dimas100% (1)
- Blackbook ProjectDocument15 pagesBlackbook ProjectNamrata Gawde100% (2)
- Advances in Industrial Control: SpringerDocument235 pagesAdvances in Industrial Control: SpringerOuarib ZakariaNo ratings yet
- Case - Saint Bridget's HospitalDocument3 pagesCase - Saint Bridget's HospitalMohammad HajihasaniNo ratings yet
- Francis Collins Human Genome ProjectDocument12 pagesFrancis Collins Human Genome ProjectMihai SabadacNo ratings yet