
1042 Full PDF
1042 Full PDF
You might also like
- Dai 2001Document5 pagesDai 2001Sri MahadhanaNo ratings yet
- Schick2006 Treatment PDFDocument7 pagesSchick2006 Treatment PDFRifqi FNo ratings yet
- OTA Highlight Paper Predicting Future Displacement of Nonoperatively Managed Lateral Compression Sacral Fractures - Can It Be DoneDocument6 pagesOTA Highlight Paper Predicting Future Displacement of Nonoperatively Managed Lateral Compression Sacral Fractures - Can It Be Doneakb601No ratings yet
- Spinal Epidural Cavernous Hemangiomas in The 2024 International Journal of SDocument3 pagesSpinal Epidural Cavernous Hemangiomas in The 2024 International Journal of SRonald QuezadaNo ratings yet
- Dickman Classification (1996)Document7 pagesDickman Classification (1996)João Pedro ZenattoNo ratings yet
- Fractures of The Scapular Neck: Diagnosis, Classifications and TreatmentDocument11 pagesFractures of The Scapular Neck: Diagnosis, Classifications and Treatmentsoheil ostovanNo ratings yet
- Posterior Lumbar Interbody Fusion (PLIF) With Cages and Local Bone Graft in The Treatment of Spinal StenosisDocument7 pagesPosterior Lumbar Interbody Fusion (PLIF) With Cages and Local Bone Graft in The Treatment of Spinal StenosisMd.Shafiul EzazNo ratings yet
- The Use of A Transolecranon Pin in The Treatment of Flexion-Type SCFsDocument6 pagesThe Use of A Transolecranon Pin in The Treatment of Flexion-Type SCFsBariša KiršnerNo ratings yet
- Fuchs 2005Document5 pagesFuchs 2005BudhiNo ratings yet
- 264 2014 Article 2282Document4 pages264 2014 Article 2282fm123165464No ratings yet
- J Neurol Sci (Turk)Document9 pagesJ Neurol Sci (Turk)nulaeli Siti ANo ratings yet
- Endoscopic Resection of Symptomatic Osteochondroma of The Distal FemurDocument4 pagesEndoscopic Resection of Symptomatic Osteochondroma of The Distal FemurAlex CirlanNo ratings yet
- Foramen Huschke PatologicoDocument7 pagesForamen Huschke PatologicoLM AdrianneNo ratings yet
- Tur CicaDocument8 pagesTur CicazubayetarkoNo ratings yet
- Intramedullary K-Wire Fixation of Metacarpal Fractures: Georg Kelsch Christoph UlrichDocument4 pagesIntramedullary K-Wire Fixation of Metacarpal Fractures: Georg Kelsch Christoph UlrichVolcNo ratings yet
- Spinous Process Fractures in Osteoporotic Thoracolumbar Vertebral FracturesDocument4 pagesSpinous Process Fractures in Osteoporotic Thoracolumbar Vertebral FracturesAditya Arya PutraNo ratings yet
- Percutaneous Endoscopic Decompression Via Transforaminal Approach For Lumbar Lateral Recess Stenosis in Geriatric PatientsDocument7 pagesPercutaneous Endoscopic Decompression Via Transforaminal Approach For Lumbar Lateral Recess Stenosis in Geriatric PatientsAmina GoharyNo ratings yet
- Hip Arthroplasty in Failed Intertrochanteric Fract 103652Document6 pagesHip Arthroplasty in Failed Intertrochanteric Fract 103652seatrrtleNo ratings yet
- 5-Level Spondylectomy For en Bloc Resection of Thoracic Chordoma: Case ReportDocument9 pages5-Level Spondylectomy For en Bloc Resection of Thoracic Chordoma: Case Reportholt linNo ratings yet
- Free Hand Pedicle Screw Placement in The Thoracic KIM LENKE 2004 Spine PDFDocument10 pagesFree Hand Pedicle Screw Placement in The Thoracic KIM LENKE 2004 Spine PDFOlgerAlarconCasanovaNo ratings yet
- PCL Avulsion Fracture 2Document2 pagesPCL Avulsion Fracture 2harpreet singhNo ratings yet
- Variability in Olecranon Ao Fracture Fixation: A Radiological StudyDocument6 pagesVariability in Olecranon Ao Fracture Fixation: A Radiological StudyFhietry Idrus ScaftweeNo ratings yet
- Ganesh 2011Document5 pagesGanesh 2011Giang Nguyễn NgânNo ratings yet
- Paper 38Document6 pagesPaper 38Dr Vineet KumarNo ratings yet
- Phillips 2013Document6 pagesPhillips 2013thanawatsimaNo ratings yet
- Songcharoen 1995Document5 pagesSongcharoen 1995Le Manh ThuongNo ratings yet
- Nakamichi 1997Document10 pagesNakamichi 1997miguelNo ratings yet
- Art3a10 10072fs00256-014-1842-5Document9 pagesArt3a10 10072fs00256-014-1842-5api-253958760No ratings yet
- Süleyman Alp Çölbe Mert Çiftdemir Fethi Emre Ustabaşıoğlu Cihan ÖzgürDocument10 pagesSüleyman Alp Çölbe Mert Çiftdemir Fethi Emre Ustabaşıoğlu Cihan Özgüraymanelhoudali6911No ratings yet
- Short Versus Long Outcome RadiologisDocument7 pagesShort Versus Long Outcome Radiologisandy ardiansyahNo ratings yet
- Fluoroscopic Analysis of The Kinematics of Deep Exion in Total Knee ArthroplastyDocument4 pagesFluoroscopic Analysis of The Kinematics of Deep Exion in Total Knee Arthroplastyjmhinos4833No ratings yet
- 3 Column AnkleDocument8 pages3 Column AnkleJosé Eduardo Fernandez RodriguezNo ratings yet
- Ueki 2007Document7 pagesUeki 2007abhishekjha0082No ratings yet
- Pedicle Screw Fixation in Fracture of Thoraco-Lumbar SpineDocument21 pagesPedicle Screw Fixation in Fracture of Thoraco-Lumbar SpineNiyati SharmaNo ratings yet
- Haglund's Syndrome Schneider2000Document5 pagesHaglund's Syndrome Schneider2000emrahaltuntasNo ratings yet
- iCVTPFDocument5 pagesiCVTPFErwin Chiquete, MD, PhDNo ratings yet
- 1413 7852 Aob 24 03 00159Document5 pages1413 7852 Aob 24 03 00159Rakesh KumarNo ratings yet
- Effects On Inadvertent Endplate Fracture Following Lateral Cage Placement On Range of Motion and Indirect Spine Decompression in Lumbar Spine Fusion Constructs: A Cadaveric StudyDocument8 pagesEffects On Inadvertent Endplate Fracture Following Lateral Cage Placement On Range of Motion and Indirect Spine Decompression in Lumbar Spine Fusion Constructs: A Cadaveric Studysiti hanifahNo ratings yet
- Zygomatic Fractures: Classification and Complications: TveterasDocument7 pagesZygomatic Fractures: Classification and Complications: TveterasBriando Stevano LinelejanNo ratings yet
- Rodilla Inervación Tran2018 PDFDocument8 pagesRodilla Inervación Tran2018 PDFLore BarreraNo ratings yet
- Discrimination of Metastatic From Acute Osteoporotic Compression Spinal Fractures With MRIDocument9 pagesDiscrimination of Metastatic From Acute Osteoporotic Compression Spinal Fractures With MRIChow Tat SingNo ratings yet
- Using The Endoscopic Transconjunctival and Transcaruncular Approach To Repair Combined Orbital Floor and Medial Wall Blowout FracturesDocument4 pagesUsing The Endoscopic Transconjunctival and Transcaruncular Approach To Repair Combined Orbital Floor and Medial Wall Blowout Fracturesstoia_sebiNo ratings yet
- Unstable Burst Fractures of The Thoraco-Lumbar Junction TreatmentDocument8 pagesUnstable Burst Fractures of The Thoraco-Lumbar Junction TreatmentRafael Jardim de MouraNo ratings yet
- Yulisa 2Document7 pagesYulisa 2Ardi WidiatmikaNo ratings yet
- A Long Term Follow Up Study of Total Meniscectomy.30Document5 pagesA Long Term Follow Up Study of Total Meniscectomy.30Anshal GuptaNo ratings yet
- (10920684 - Neurosurgical Focus) Surgical Treatment of Primary Sacral Tumors - Complications Associated With SacrectomyDocument8 pages(10920684 - Neurosurgical Focus) Surgical Treatment of Primary Sacral Tumors - Complications Associated With Sacrectomyfloroiu.ioana.valeriaNo ratings yet
- Anterior Decompression Techniques For Thoracic and Lumbar FracturesDocument10 pagesAnterior Decompression Techniques For Thoracic and Lumbar Fracturesmetasoniko81No ratings yet
- Operative Treatment of Peritrochanteric Osteoporotic Fractures With Proximal Femur Locking Compression Plate A Consecutive StudyDocument6 pagesOperative Treatment of Peritrochanteric Osteoporotic Fractures With Proximal Femur Locking Compression Plate A Consecutive StudyAthenaeum Scientific PublishersNo ratings yet
- Relación Flujo y Fractura ClinicaDocument5 pagesRelación Flujo y Fractura ClinicaPedro TorresNo ratings yet
- Nasional 3 NIC:KOE Penetrating Cervial Spine Injury ENDocument6 pagesNasional 3 NIC:KOE Penetrating Cervial Spine Injury ENHeru Sutanto KNo ratings yet
- Syndesmotic Screw Removed Verusus Retained: A Comparative Functional AnalysisDocument4 pagesSyndesmotic Screw Removed Verusus Retained: A Comparative Functional AnalysisSarath KumarNo ratings yet
- Core Decompression With Bone Grafting For Osteonecrosis of The Femoral HeadDocument8 pagesCore Decompression With Bone Grafting For Osteonecrosis of The Femoral Headmuhammad0umar-4No ratings yet
- Clinical Outcome of A Precontoured Symphysis Pubis Plate With Tension Band Wiring For Traumatic Symphysis Pubis Rupture in Pelvic FracturesDocument6 pagesClinical Outcome of A Precontoured Symphysis Pubis Plate With Tension Band Wiring For Traumatic Symphysis Pubis Rupture in Pelvic FracturesodyNo ratings yet
- Surgical Management of Sacral Chordomas - Illustrative Cases and Current Management ParadigmsDocument7 pagesSurgical Management of Sacral Chordomas - Illustrative Cases and Current Management ParadigmsHugo JBNo ratings yet
- Treatment of Distal Humerus FracturedDocument10 pagesTreatment of Distal Humerus Fracturedauliya ningsihNo ratings yet
- Ojo 2013112116194629 PDFDocument5 pagesOjo 2013112116194629 PDFYash SharmaNo ratings yet
- "A To P" Screw Versus Posterolateral Plate For PosteriorDocument6 pages"A To P" Screw Versus Posterolateral Plate For PosteriorErlin EsauNo ratings yet
- (10920684 - Neurosurgical Focus) Percutaneous Pedicle Screw Fixation of The Lumbar SpineDocument9 pages(10920684 - Neurosurgical Focus) Percutaneous Pedicle Screw Fixation of The Lumbar Spineefancoolhand09No ratings yet
- Giacalone 2015Document7 pagesGiacalone 2015Joseval FilhoNo ratings yet
- Surgery of the Cranio-Vertebral JunctionFrom EverandSurgery of the Cranio-Vertebral JunctionEnrico TessitoreNo ratings yet
- 586 2009 Article 1037Document7 pages586 2009 Article 1037Ramy ElmasryNo ratings yet
- Versus Overall Sagittal AlignmentDocument7 pagesVersus Overall Sagittal AlignmentRamy ElmasryNo ratings yet
- Spontaneous Height Restoration of Vertebral Compression FractureDocument4 pagesSpontaneous Height Restoration of Vertebral Compression FractureRamy ElmasryNo ratings yet
- Pediatrics With Answers and ExplanationsDocument77 pagesPediatrics With Answers and ExplanationsRamy Elmasry100% (6)
- Significance of Dynamic Mobility in Restoring Vertebral Body Height in VertebroplastyDocument4 pagesSignificance of Dynamic Mobility in Restoring Vertebral Body Height in VertebroplastyRamy ElmasryNo ratings yet
- 16-Zhou Et AlDocument6 pages16-Zhou Et AlRamy ElmasryNo ratings yet
- 86 D 8Document7 pages86 D 8Ramy ElmasryNo ratings yet
- Leakage of Cement in Percutaneous Transpedicular Vertebroplasty For Painful Osteoporotic Compression FracturesDocument7 pagesLeakage of Cement in Percutaneous Transpedicular Vertebroplasty For Painful Osteoporotic Compression FracturesRamy ElmasryNo ratings yet
- MainDocument8 pagesMainRamy ElmasryNo ratings yet
- Acute Osteoporotic Vertebral Collapse: Open Study On Percutaneous Injection of Acrylic Surgical Cement in 20 PatientsDocument6 pagesAcute Osteoporotic Vertebral Collapse: Open Study On Percutaneous Injection of Acrylic Surgical Cement in 20 PatientsRamy ElmasryNo ratings yet
- Percutaneous Vertebroplasty and Balloon Kyphoplasty For The Treatment of Osteoporotic Vertebral Compression Fractures and Osteolytic TumoursDocument10 pagesPercutaneous Vertebroplasty and Balloon Kyphoplasty For The Treatment of Osteoporotic Vertebral Compression Fractures and Osteolytic TumoursRamy ElmasryNo ratings yet
- Morning Endorsements: MAY 15-16, 2019 Coc: Dr. Arriola Rod: Dr. Oyas Iod: Co & DickinaDocument11 pagesMorning Endorsements: MAY 15-16, 2019 Coc: Dr. Arriola Rod: Dr. Oyas Iod: Co & DickinaNeil Victor Ongco PajugotNo ratings yet
- Surgical Management in LeprosyDocument33 pagesSurgical Management in Leprosynsv.epicNo ratings yet
- Brochure of ICE SHAPING IV PRODocument15 pagesBrochure of ICE SHAPING IV PROUniforrmes ArcoirisNo ratings yet
- Perioperative Care For CABG PatientsDocument32 pagesPerioperative Care For CABG PatientsAya EyadNo ratings yet
- HIATAL HERNIA PPT Final PDFDocument49 pagesHIATAL HERNIA PPT Final PDFregysujit60% (5)
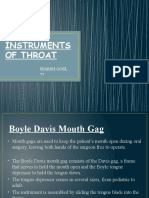
- Instruments of Throat: Sparsh Goel 77Document19 pagesInstruments of Throat: Sparsh Goel 77Sparsh GoelNo ratings yet
- Hernia QuestionsDocument6 pagesHernia QuestionsNica Lopez Fernandez100% (1)
- LAPORAN TUTORIAL SKENARIO 5 B.3-DikompresiDocument30 pagesLAPORAN TUTORIAL SKENARIO 5 B.3-DikompresiKrishna Dava Putra SNo ratings yet
- Frozen Shoulder - Adhesive CapsulitisDocument8 pagesFrozen Shoulder - Adhesive CapsulitisfriskaNo ratings yet
- Product Catalog Bauerfeind Usa 0312Document88 pagesProduct Catalog Bauerfeind Usa 0312Guillermo Carpio FloriaNo ratings yet
- Atls Pre Test 1 PDFDocument72 pagesAtls Pre Test 1 PDFmary011danielNo ratings yet
- Intestinal Ostomy: Classification, Indications, Ostomy Care and Complication ManagementDocument8 pagesIntestinal Ostomy: Classification, Indications, Ostomy Care and Complication ManagementEriekafebriayana RNo ratings yet
- BD-11097 UltraCor BrochureDocument3 pagesBD-11097 UltraCor Brochurepo leongNo ratings yet
- 6.6) Diagnostic and Therapeutic Abdominal Paracentesis - UpToDateDocument18 pages6.6) Diagnostic and Therapeutic Abdominal Paracentesis - UpToDatefedericoNo ratings yet
- Arn Report List 20200505Document305 pagesArn Report List 20200505zoheir salmaniNo ratings yet
- PTBD 2Document4 pagesPTBD 2Alcntara AllenNo ratings yet
- ORDocument4 pagesORJoana Marie A. LaoNo ratings yet
- Spiritual Needs of A Patient With Acute IllnessDocument3 pagesSpiritual Needs of A Patient With Acute IllnessMarimiel PagulayanNo ratings yet
- V3 WEREWOLF Tech Bro Flo 0720Document6 pagesV3 WEREWOLF Tech Bro Flo 0720hongyuan xuNo ratings yet
- Laparoscopic Cholecystectomy Perioperative Management: An UpdateDocument5 pagesLaparoscopic Cholecystectomy Perioperative Management: An UpdateNurlailah AliNo ratings yet
- Pearls Nov Dec 2010Document3 pagesPearls Nov Dec 2010Nhật LongNo ratings yet
- Laser Technolas 217 - Excimer Laser SystemDocument34 pagesLaser Technolas 217 - Excimer Laser Systemrubens.nascimento213No ratings yet
- Cone-Beam Computed Tomography and Its Applications in DentistryDocument4 pagesCone-Beam Computed Tomography and Its Applications in DentistryMeris JugadorNo ratings yet
- Karnatka 2023Document3 pagesKarnatka 2023bvkarthik.99No ratings yet
- Appleby OperationDocument9 pagesAppleby OperationPeter Paul PascualNo ratings yet
- Helland L Nursing ChecklistDocument6 pagesHelland L Nursing Checklistapi-703155063No ratings yet
- Complications of The Arteriovenous Fistula: A Systematic ReviewDocument45 pagesComplications of The Arteriovenous Fistula: A Systematic ReviewAnonymous ATdLPZNo ratings yet
- Hernia 1Document28 pagesHernia 1Aminatulhuda SulaimanNo ratings yet
- យល់ដឹងអំពីតួនាទីរបស់ខ្នែងពោះវៀនDocument4 pagesយល់ដឹងអំពីតួនាទីរបស់ខ្នែងពោះវៀនReal Madrid FCNo ratings yet
- Intra Operative Allowable Blood Loss: Estimation Made Easy: Original Research ArticleDocument5 pagesIntra Operative Allowable Blood Loss: Estimation Made Easy: Original Research ArticlesafwanNo ratings yet



































































































Download as pdf or txt
You might also like
- Dai 2001Document5 pagesDai 2001Sri MahadhanaNo ratings yet
- Schick2006 Treatment PDFDocument7 pagesSchick2006 Treatment PDFRifqi FNo ratings yet
- OTA Highlight Paper Predicting Future Displacement of Nonoperatively Managed Lateral Compression Sacral Fractures - Can It Be DoneDocument6 pagesOTA Highlight Paper Predicting Future Displacement of Nonoperatively Managed Lateral Compression Sacral Fractures - Can It Be Doneakb601No ratings yet
- Spinal Epidural Cavernous Hemangiomas in The 2024 International Journal of SDocument3 pagesSpinal Epidural Cavernous Hemangiomas in The 2024 International Journal of SRonald QuezadaNo ratings yet
- Dickman Classification (1996)Document7 pagesDickman Classification (1996)João Pedro ZenattoNo ratings yet
- Fractures of The Scapular Neck: Diagnosis, Classifications and TreatmentDocument11 pagesFractures of The Scapular Neck: Diagnosis, Classifications and Treatmentsoheil ostovanNo ratings yet
- Posterior Lumbar Interbody Fusion (PLIF) With Cages and Local Bone Graft in The Treatment of Spinal StenosisDocument7 pagesPosterior Lumbar Interbody Fusion (PLIF) With Cages and Local Bone Graft in The Treatment of Spinal StenosisMd.Shafiul EzazNo ratings yet
- The Use of A Transolecranon Pin in The Treatment of Flexion-Type SCFsDocument6 pagesThe Use of A Transolecranon Pin in The Treatment of Flexion-Type SCFsBariša KiršnerNo ratings yet
- Fuchs 2005Document5 pagesFuchs 2005BudhiNo ratings yet
- 264 2014 Article 2282Document4 pages264 2014 Article 2282fm123165464No ratings yet
- J Neurol Sci (Turk)Document9 pagesJ Neurol Sci (Turk)nulaeli Siti ANo ratings yet
- Endoscopic Resection of Symptomatic Osteochondroma of The Distal FemurDocument4 pagesEndoscopic Resection of Symptomatic Osteochondroma of The Distal FemurAlex CirlanNo ratings yet
- Foramen Huschke PatologicoDocument7 pagesForamen Huschke PatologicoLM AdrianneNo ratings yet
- Tur CicaDocument8 pagesTur CicazubayetarkoNo ratings yet
- Intramedullary K-Wire Fixation of Metacarpal Fractures: Georg Kelsch Christoph UlrichDocument4 pagesIntramedullary K-Wire Fixation of Metacarpal Fractures: Georg Kelsch Christoph UlrichVolcNo ratings yet
- Spinous Process Fractures in Osteoporotic Thoracolumbar Vertebral FracturesDocument4 pagesSpinous Process Fractures in Osteoporotic Thoracolumbar Vertebral FracturesAditya Arya PutraNo ratings yet
- Percutaneous Endoscopic Decompression Via Transforaminal Approach For Lumbar Lateral Recess Stenosis in Geriatric PatientsDocument7 pagesPercutaneous Endoscopic Decompression Via Transforaminal Approach For Lumbar Lateral Recess Stenosis in Geriatric PatientsAmina GoharyNo ratings yet
- Hip Arthroplasty in Failed Intertrochanteric Fract 103652Document6 pagesHip Arthroplasty in Failed Intertrochanteric Fract 103652seatrrtleNo ratings yet
- 5-Level Spondylectomy For en Bloc Resection of Thoracic Chordoma: Case ReportDocument9 pages5-Level Spondylectomy For en Bloc Resection of Thoracic Chordoma: Case Reportholt linNo ratings yet
- Free Hand Pedicle Screw Placement in The Thoracic KIM LENKE 2004 Spine PDFDocument10 pagesFree Hand Pedicle Screw Placement in The Thoracic KIM LENKE 2004 Spine PDFOlgerAlarconCasanovaNo ratings yet
- PCL Avulsion Fracture 2Document2 pagesPCL Avulsion Fracture 2harpreet singhNo ratings yet
- Variability in Olecranon Ao Fracture Fixation: A Radiological StudyDocument6 pagesVariability in Olecranon Ao Fracture Fixation: A Radiological StudyFhietry Idrus ScaftweeNo ratings yet
- Ganesh 2011Document5 pagesGanesh 2011Giang Nguyễn NgânNo ratings yet
- Paper 38Document6 pagesPaper 38Dr Vineet KumarNo ratings yet
- Phillips 2013Document6 pagesPhillips 2013thanawatsimaNo ratings yet
- Songcharoen 1995Document5 pagesSongcharoen 1995Le Manh ThuongNo ratings yet
- Nakamichi 1997Document10 pagesNakamichi 1997miguelNo ratings yet
- Art3a10 10072fs00256-014-1842-5Document9 pagesArt3a10 10072fs00256-014-1842-5api-253958760No ratings yet
- Süleyman Alp Çölbe Mert Çiftdemir Fethi Emre Ustabaşıoğlu Cihan ÖzgürDocument10 pagesSüleyman Alp Çölbe Mert Çiftdemir Fethi Emre Ustabaşıoğlu Cihan Özgüraymanelhoudali6911No ratings yet
- Short Versus Long Outcome RadiologisDocument7 pagesShort Versus Long Outcome Radiologisandy ardiansyahNo ratings yet
- Fluoroscopic Analysis of The Kinematics of Deep Exion in Total Knee ArthroplastyDocument4 pagesFluoroscopic Analysis of The Kinematics of Deep Exion in Total Knee Arthroplastyjmhinos4833No ratings yet
- 3 Column AnkleDocument8 pages3 Column AnkleJosé Eduardo Fernandez RodriguezNo ratings yet
- Ueki 2007Document7 pagesUeki 2007abhishekjha0082No ratings yet
- Pedicle Screw Fixation in Fracture of Thoraco-Lumbar SpineDocument21 pagesPedicle Screw Fixation in Fracture of Thoraco-Lumbar SpineNiyati SharmaNo ratings yet
- Haglund's Syndrome Schneider2000Document5 pagesHaglund's Syndrome Schneider2000emrahaltuntasNo ratings yet
- iCVTPFDocument5 pagesiCVTPFErwin Chiquete, MD, PhDNo ratings yet
- 1413 7852 Aob 24 03 00159Document5 pages1413 7852 Aob 24 03 00159Rakesh KumarNo ratings yet
- Effects On Inadvertent Endplate Fracture Following Lateral Cage Placement On Range of Motion and Indirect Spine Decompression in Lumbar Spine Fusion Constructs: A Cadaveric StudyDocument8 pagesEffects On Inadvertent Endplate Fracture Following Lateral Cage Placement On Range of Motion and Indirect Spine Decompression in Lumbar Spine Fusion Constructs: A Cadaveric Studysiti hanifahNo ratings yet
- Zygomatic Fractures: Classification and Complications: TveterasDocument7 pagesZygomatic Fractures: Classification and Complications: TveterasBriando Stevano LinelejanNo ratings yet
- Rodilla Inervación Tran2018 PDFDocument8 pagesRodilla Inervación Tran2018 PDFLore BarreraNo ratings yet
- Discrimination of Metastatic From Acute Osteoporotic Compression Spinal Fractures With MRIDocument9 pagesDiscrimination of Metastatic From Acute Osteoporotic Compression Spinal Fractures With MRIChow Tat SingNo ratings yet
- Using The Endoscopic Transconjunctival and Transcaruncular Approach To Repair Combined Orbital Floor and Medial Wall Blowout FracturesDocument4 pagesUsing The Endoscopic Transconjunctival and Transcaruncular Approach To Repair Combined Orbital Floor and Medial Wall Blowout Fracturesstoia_sebiNo ratings yet
- Unstable Burst Fractures of The Thoraco-Lumbar Junction TreatmentDocument8 pagesUnstable Burst Fractures of The Thoraco-Lumbar Junction TreatmentRafael Jardim de MouraNo ratings yet
- Yulisa 2Document7 pagesYulisa 2Ardi WidiatmikaNo ratings yet
- A Long Term Follow Up Study of Total Meniscectomy.30Document5 pagesA Long Term Follow Up Study of Total Meniscectomy.30Anshal GuptaNo ratings yet
- (10920684 - Neurosurgical Focus) Surgical Treatment of Primary Sacral Tumors - Complications Associated With SacrectomyDocument8 pages(10920684 - Neurosurgical Focus) Surgical Treatment of Primary Sacral Tumors - Complications Associated With Sacrectomyfloroiu.ioana.valeriaNo ratings yet
- Anterior Decompression Techniques For Thoracic and Lumbar FracturesDocument10 pagesAnterior Decompression Techniques For Thoracic and Lumbar Fracturesmetasoniko81No ratings yet
- Operative Treatment of Peritrochanteric Osteoporotic Fractures With Proximal Femur Locking Compression Plate A Consecutive StudyDocument6 pagesOperative Treatment of Peritrochanteric Osteoporotic Fractures With Proximal Femur Locking Compression Plate A Consecutive StudyAthenaeum Scientific PublishersNo ratings yet
- Relación Flujo y Fractura ClinicaDocument5 pagesRelación Flujo y Fractura ClinicaPedro TorresNo ratings yet
- Nasional 3 NIC:KOE Penetrating Cervial Spine Injury ENDocument6 pagesNasional 3 NIC:KOE Penetrating Cervial Spine Injury ENHeru Sutanto KNo ratings yet
- Syndesmotic Screw Removed Verusus Retained: A Comparative Functional AnalysisDocument4 pagesSyndesmotic Screw Removed Verusus Retained: A Comparative Functional AnalysisSarath KumarNo ratings yet
- Core Decompression With Bone Grafting For Osteonecrosis of The Femoral HeadDocument8 pagesCore Decompression With Bone Grafting For Osteonecrosis of The Femoral Headmuhammad0umar-4No ratings yet
- Clinical Outcome of A Precontoured Symphysis Pubis Plate With Tension Band Wiring For Traumatic Symphysis Pubis Rupture in Pelvic FracturesDocument6 pagesClinical Outcome of A Precontoured Symphysis Pubis Plate With Tension Band Wiring For Traumatic Symphysis Pubis Rupture in Pelvic FracturesodyNo ratings yet
- Surgical Management of Sacral Chordomas - Illustrative Cases and Current Management ParadigmsDocument7 pagesSurgical Management of Sacral Chordomas - Illustrative Cases and Current Management ParadigmsHugo JBNo ratings yet
- Treatment of Distal Humerus FracturedDocument10 pagesTreatment of Distal Humerus Fracturedauliya ningsihNo ratings yet
- Ojo 2013112116194629 PDFDocument5 pagesOjo 2013112116194629 PDFYash SharmaNo ratings yet
- "A To P" Screw Versus Posterolateral Plate For PosteriorDocument6 pages"A To P" Screw Versus Posterolateral Plate For PosteriorErlin EsauNo ratings yet
- (10920684 - Neurosurgical Focus) Percutaneous Pedicle Screw Fixation of The Lumbar SpineDocument9 pages(10920684 - Neurosurgical Focus) Percutaneous Pedicle Screw Fixation of The Lumbar Spineefancoolhand09No ratings yet
- Giacalone 2015Document7 pagesGiacalone 2015Joseval FilhoNo ratings yet
- Surgery of the Cranio-Vertebral JunctionFrom EverandSurgery of the Cranio-Vertebral JunctionEnrico TessitoreNo ratings yet
- 586 2009 Article 1037Document7 pages586 2009 Article 1037Ramy ElmasryNo ratings yet
- Versus Overall Sagittal AlignmentDocument7 pagesVersus Overall Sagittal AlignmentRamy ElmasryNo ratings yet
- Spontaneous Height Restoration of Vertebral Compression FractureDocument4 pagesSpontaneous Height Restoration of Vertebral Compression FractureRamy ElmasryNo ratings yet
- Pediatrics With Answers and ExplanationsDocument77 pagesPediatrics With Answers and ExplanationsRamy Elmasry100% (6)
- Significance of Dynamic Mobility in Restoring Vertebral Body Height in VertebroplastyDocument4 pagesSignificance of Dynamic Mobility in Restoring Vertebral Body Height in VertebroplastyRamy ElmasryNo ratings yet
- 16-Zhou Et AlDocument6 pages16-Zhou Et AlRamy ElmasryNo ratings yet
- 86 D 8Document7 pages86 D 8Ramy ElmasryNo ratings yet
- Leakage of Cement in Percutaneous Transpedicular Vertebroplasty For Painful Osteoporotic Compression FracturesDocument7 pagesLeakage of Cement in Percutaneous Transpedicular Vertebroplasty For Painful Osteoporotic Compression FracturesRamy ElmasryNo ratings yet
- MainDocument8 pagesMainRamy ElmasryNo ratings yet
- Acute Osteoporotic Vertebral Collapse: Open Study On Percutaneous Injection of Acrylic Surgical Cement in 20 PatientsDocument6 pagesAcute Osteoporotic Vertebral Collapse: Open Study On Percutaneous Injection of Acrylic Surgical Cement in 20 PatientsRamy ElmasryNo ratings yet
- Percutaneous Vertebroplasty and Balloon Kyphoplasty For The Treatment of Osteoporotic Vertebral Compression Fractures and Osteolytic TumoursDocument10 pagesPercutaneous Vertebroplasty and Balloon Kyphoplasty For The Treatment of Osteoporotic Vertebral Compression Fractures and Osteolytic TumoursRamy ElmasryNo ratings yet
- Morning Endorsements: MAY 15-16, 2019 Coc: Dr. Arriola Rod: Dr. Oyas Iod: Co & DickinaDocument11 pagesMorning Endorsements: MAY 15-16, 2019 Coc: Dr. Arriola Rod: Dr. Oyas Iod: Co & DickinaNeil Victor Ongco PajugotNo ratings yet
- Surgical Management in LeprosyDocument33 pagesSurgical Management in Leprosynsv.epicNo ratings yet
- Brochure of ICE SHAPING IV PRODocument15 pagesBrochure of ICE SHAPING IV PROUniforrmes ArcoirisNo ratings yet
- Perioperative Care For CABG PatientsDocument32 pagesPerioperative Care For CABG PatientsAya EyadNo ratings yet
- HIATAL HERNIA PPT Final PDFDocument49 pagesHIATAL HERNIA PPT Final PDFregysujit60% (5)
- Instruments of Throat: Sparsh Goel 77Document19 pagesInstruments of Throat: Sparsh Goel 77Sparsh GoelNo ratings yet
- Hernia QuestionsDocument6 pagesHernia QuestionsNica Lopez Fernandez100% (1)
- LAPORAN TUTORIAL SKENARIO 5 B.3-DikompresiDocument30 pagesLAPORAN TUTORIAL SKENARIO 5 B.3-DikompresiKrishna Dava Putra SNo ratings yet
- Frozen Shoulder - Adhesive CapsulitisDocument8 pagesFrozen Shoulder - Adhesive CapsulitisfriskaNo ratings yet
- Product Catalog Bauerfeind Usa 0312Document88 pagesProduct Catalog Bauerfeind Usa 0312Guillermo Carpio FloriaNo ratings yet
- Atls Pre Test 1 PDFDocument72 pagesAtls Pre Test 1 PDFmary011danielNo ratings yet
- Intestinal Ostomy: Classification, Indications, Ostomy Care and Complication ManagementDocument8 pagesIntestinal Ostomy: Classification, Indications, Ostomy Care and Complication ManagementEriekafebriayana RNo ratings yet
- BD-11097 UltraCor BrochureDocument3 pagesBD-11097 UltraCor Brochurepo leongNo ratings yet
- 6.6) Diagnostic and Therapeutic Abdominal Paracentesis - UpToDateDocument18 pages6.6) Diagnostic and Therapeutic Abdominal Paracentesis - UpToDatefedericoNo ratings yet
- Arn Report List 20200505Document305 pagesArn Report List 20200505zoheir salmaniNo ratings yet
- PTBD 2Document4 pagesPTBD 2Alcntara AllenNo ratings yet
- ORDocument4 pagesORJoana Marie A. LaoNo ratings yet
- Spiritual Needs of A Patient With Acute IllnessDocument3 pagesSpiritual Needs of A Patient With Acute IllnessMarimiel PagulayanNo ratings yet
- V3 WEREWOLF Tech Bro Flo 0720Document6 pagesV3 WEREWOLF Tech Bro Flo 0720hongyuan xuNo ratings yet
- Laparoscopic Cholecystectomy Perioperative Management: An UpdateDocument5 pagesLaparoscopic Cholecystectomy Perioperative Management: An UpdateNurlailah AliNo ratings yet
- Pearls Nov Dec 2010Document3 pagesPearls Nov Dec 2010Nhật LongNo ratings yet
- Laser Technolas 217 - Excimer Laser SystemDocument34 pagesLaser Technolas 217 - Excimer Laser Systemrubens.nascimento213No ratings yet
- Cone-Beam Computed Tomography and Its Applications in DentistryDocument4 pagesCone-Beam Computed Tomography and Its Applications in DentistryMeris JugadorNo ratings yet
- Karnatka 2023Document3 pagesKarnatka 2023bvkarthik.99No ratings yet
- Appleby OperationDocument9 pagesAppleby OperationPeter Paul PascualNo ratings yet
- Helland L Nursing ChecklistDocument6 pagesHelland L Nursing Checklistapi-703155063No ratings yet
- Complications of The Arteriovenous Fistula: A Systematic ReviewDocument45 pagesComplications of The Arteriovenous Fistula: A Systematic ReviewAnonymous ATdLPZNo ratings yet
- Hernia 1Document28 pagesHernia 1Aminatulhuda SulaimanNo ratings yet
- យល់ដឹងអំពីតួនាទីរបស់ខ្នែងពោះវៀនDocument4 pagesយល់ដឹងអំពីតួនាទីរបស់ខ្នែងពោះវៀនReal Madrid FCNo ratings yet
- Intra Operative Allowable Blood Loss: Estimation Made Easy: Original Research ArticleDocument5 pagesIntra Operative Allowable Blood Loss: Estimation Made Easy: Original Research ArticlesafwanNo ratings yet