Download as docx, pdf, or txt
You might also like
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- UWorld Notes - Peds 2Document38 pagesUWorld Notes - Peds 2Dylan GerlachNo ratings yet
- Curs 14.1 Insuficienta Mitrala 03.2013Document62 pagesCurs 14.1 Insuficienta Mitrala 03.2013Anonymous CQmrhq1O7No ratings yet
- Maths On The Move' - Effectiveness of Physically-Active Lessons For Learning Maths and Increasing Physical Activity in Primary School StudentsDocument22 pagesMaths On The Move' - Effectiveness of Physically-Active Lessons For Learning Maths and Increasing Physical Activity in Primary School Studentsiisu-cmse libraryNo ratings yet
- Peds Shelf NotesDocument73 pagesPeds Shelf NotesTanyaMusonza100% (1)
- Peds Shelf NotesDocument88 pagesPeds Shelf Notesγιαννης παπαςNo ratings yet
- Congenital Heart DiseaseDocument74 pagesCongenital Heart DiseaseKeith LajotNo ratings yet
- Congenital Heart DiseaseDocument3 pagesCongenital Heart DiseaseKarisaNo ratings yet
- Penyakit KatupDocument31 pagesPenyakit KatupAdinda Suci MaghfiraNo ratings yet
- Acyanotic Congenital Heart DiseaseDocument2 pagesAcyanotic Congenital Heart DiseaseZiyad100% (1)
- Congenital Heart Defects - CyanoticDocument3 pagesCongenital Heart Defects - Cyanoticr5ss7pq9tpNo ratings yet
- INTRO CARDIOLOGY LECTURE FinalDocument38 pagesINTRO CARDIOLOGY LECTURE FinalFlorencio D. Santos IVNo ratings yet
- Clinical Congenital Heart Disease: Prof M S Ranjit MD DCH Senior Consultant Paed. Cardiologist ChennaiDocument78 pagesClinical Congenital Heart Disease: Prof M S Ranjit MD DCH Senior Consultant Paed. Cardiologist ChennaiAnişoara FrunzeNo ratings yet
- Basic Cardiac Structure and FunctionDocument13 pagesBasic Cardiac Structure and FunctiondeaNo ratings yet
- Curs 4 Urgente in Cardiologie Anul VI Seriile A B C DDocument35 pagesCurs 4 Urgente in Cardiologie Anul VI Seriile A B C DBoţu AlexandruNo ratings yet
- Obstructive LesionsDocument7 pagesObstructive LesionsMaikka IlaganNo ratings yet
- Cardiology CardiovascularExaminationDocument5 pagesCardiology CardiovascularExaminationSalifyanji SimpambaNo ratings yet
- Cardiopatii Congenitale 17-18 enDocument74 pagesCardiopatii Congenitale 17-18 enMatei PopescuNo ratings yet
- Physical Diagnosis CVS BCCM Second Year Lecture MARKMDDocument26 pagesPhysical Diagnosis CVS BCCM Second Year Lecture MARKMDJoseph De JoyaNo ratings yet
- Pediatric Cardiology Part 2Document3 pagesPediatric Cardiology Part 2carlosNo ratings yet
- CCHDDocument69 pagesCCHDchebetnaomi945No ratings yet
- Valvular 2005Document32 pagesValvular 2005rajeeNo ratings yet
- Valvular Heart Disease: Chalinee Pravarnpat, M.DDocument49 pagesValvular Heart Disease: Chalinee Pravarnpat, M.DChalee InkateNo ratings yet
- Mumurs Summary PDFDocument6 pagesMumurs Summary PDFykteo323No ratings yet
- Anak 2Document107 pagesAnak 2Nency PurmayaNo ratings yet
- Pericardial Disease: Adel Hasanin Ahmed 1Document5 pagesPericardial Disease: Adel Hasanin Ahmed 1Shaz ChindhyNo ratings yet
- K9. Penyakit Kardiovaskuler BawaanDocument70 pagesK9. Penyakit Kardiovaskuler Bawaanjulis muharamNo ratings yet
- Cardiogenic Shock FinalDocument73 pagesCardiogenic Shock FinalksugamoNo ratings yet
- Valvular Heart Disease and The Cardiac Exam: Charlotte Bai, M.D. Internal Medicine Board Review May 28, 2009Document42 pagesValvular Heart Disease and The Cardiac Exam: Charlotte Bai, M.D. Internal Medicine Board Review May 28, 2009Ami DhaniaNo ratings yet
- Valvular Heart Disease and The Cardiac ExamDocument42 pagesValvular Heart Disease and The Cardiac ExamJuwanto WakiminNo ratings yet
- Valvular Heart Disease: Hakim AlkatiriDocument84 pagesValvular Heart Disease: Hakim AlkatiriFNo ratings yet
- VSDDocument34 pagesVSDMerlina Wijayawati100% (2)
- Midterm Reviewer NCM 109Document6 pagesMidterm Reviewer NCM 109Maria JuanilloNo ratings yet
- Acyanotic CHDDocument83 pagesAcyanotic CHDmrinmayee deshmukhNo ratings yet
- Dr. RSK - Cyanotic Congenital Heart DiseaseDocument44 pagesDr. RSK - Cyanotic Congenital Heart Diseasemanjunath182019No ratings yet
- Congenital Heart DiseaseDocument20 pagesCongenital Heart DiseaseAbhishek KumarNo ratings yet
- Congenital Heart Disease - Dr. HabibieDocument43 pagesCongenital Heart Disease - Dr. HabibieNanda Kurnia RamadhanNo ratings yet
- Pediatric Nursing Reviewer CardiovascularDocument4 pagesPediatric Nursing Reviewer CardiovascularnieacatleyaNo ratings yet
- Peds Shelf NotesDocument74 pagesPeds Shelf NotesRandy BornmannNo ratings yet
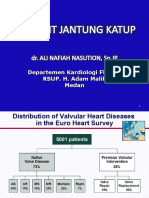
- Penyakit Jantung KatupDocument35 pagesPenyakit Jantung Katupdwi ariskaNo ratings yet
- Acyanotic Congenital Heart Disease: Pediatric Cardiology Division University of Sumatera UtaraDocument40 pagesAcyanotic Congenital Heart Disease: Pediatric Cardiology Division University of Sumatera UtaraHanda YaniNo ratings yet
- Congenital Heart Defects - AcyanoticDocument6 pagesCongenital Heart Defects - Acyanoticr5ss7pq9tpNo ratings yet
- Valvular Heart DiseaseDocument85 pagesValvular Heart DiseaseWilliam Lie100% (2)
- PULSEDocument84 pagesPULSEVivek JaganathanNo ratings yet
- PANCE Prep Pearls Valvular Disease PDFDocument4 pagesPANCE Prep Pearls Valvular Disease PDFkatNo ratings yet
- Aortic Stenosis and Aortic RegugitationDocument3 pagesAortic Stenosis and Aortic RegugitationAndrassy Twinkle AlineaNo ratings yet
- Congenital Heart DiseaseDocument6 pagesCongenital Heart DiseaseSamah KhanNo ratings yet
- 7 PENYAKIT JANTUNG BAWAAN DR - YusraDocument57 pages7 PENYAKIT JANTUNG BAWAAN DR - YusraSurya ArhNo ratings yet
- 28 Valvular Heart Disease DR - YusraDocument46 pages28 Valvular Heart Disease DR - YusraSurya ArhNo ratings yet
- KP 2.3.1.6Document42 pagesKP 2.3.1.6Taufiqurrahman HabibNo ratings yet
- Mitral StenosisDocument37 pagesMitral StenosisInsan IlmanNo ratings yet
- VHD Inter FinalDocument84 pagesVHD Inter Finalfitrah fajrianiNo ratings yet
- (Medbook4u Com) IllBaby1Document693 pages(Medbook4u Com) IllBaby1Certificate SurrenderNo ratings yet
- Valvular UpdateDocument44 pagesValvular UpdateUlmi FadillahNo ratings yet
- Slide Untuk SabtuDocument35 pagesSlide Untuk SabtuAgustinus FatollaNo ratings yet
- Cardio ReviewDocument25 pagesCardio ReviewHarini PrayagaNo ratings yet
- Pulmonary RegurgitationDocument3 pagesPulmonary RegurgitationTaniaNo ratings yet
- Management of Cyanotic Child BivinDocument48 pagesManagement of Cyanotic Child BivinChippy BivinNo ratings yet
- ch28 Notes Part 2Document9 pagesch28 Notes Part 2Monica JubaneNo ratings yet
- Tetrology of FallotDocument55 pagesTetrology of FallotShravani ShagapuramNo ratings yet
- Epidemology: Saas Have A Female:Male Ratio of 4:1 and Have Been Found To Be Associated With MultiparityDocument1 pageEpidemology: Saas Have A Female:Male Ratio of 4:1 and Have Been Found To Be Associated With MultiparityAlvin De LunaNo ratings yet
- SOHA PROJECT PROPOSAL Newly EditedDocument8 pagesSOHA PROJECT PROPOSAL Newly EditedAlvin De LunaNo ratings yet
- Cary David Richards - Peter G. Hanson: "If Stress Is The Villain, Humor Is The Superhero."Document2 pagesCary David Richards - Peter G. Hanson: "If Stress Is The Villain, Humor Is The Superhero."Alvin De LunaNo ratings yet
- Neuroanatomy of Language-lonelybitterEDITTED1Document6 pagesNeuroanatomy of Language-lonelybitterEDITTED1Alvin De LunaNo ratings yet
- Initial Assessment and ManagementDocument8 pagesInitial Assessment and ManagementAlvin De LunaNo ratings yet
- Spina Bifida Is The Most Common of Congenital Anomalies of The Central Nervous System That Are Compatible With LifeDocument9 pagesSpina Bifida Is The Most Common of Congenital Anomalies of The Central Nervous System That Are Compatible With LifeAlvin De LunaNo ratings yet
- RRLDocument4 pagesRRLGlessySeguillaBumanglagNo ratings yet
- Basic Wheelchair Assessment FormDocument2 pagesBasic Wheelchair Assessment FormdshanejNo ratings yet
- Paper 1 - Medicine Through Time - Revision BookDocument54 pagesPaper 1 - Medicine Through Time - Revision BookDylan DanovNo ratings yet
- EssixDocument5 pagesEssixdent in dentistNo ratings yet
- O Poder de Cura Do AmorDocument3 pagesO Poder de Cura Do AmorDoido MineiroNo ratings yet
- Regulatory Compliance Pharmacy Manager in Tampa FL Resume John HawesDocument2 pagesRegulatory Compliance Pharmacy Manager in Tampa FL Resume John HawesJohnHawesNo ratings yet
- DVT DR Moses KazeevuDocument24 pagesDVT DR Moses KazeevuMoses Jr KazevuNo ratings yet
- Comat NotesDocument33 pagesComat NotesVee Mend100% (1)
- IB10-442 Dental Benefits For Veterans 2 14Document3 pagesIB10-442 Dental Benefits For Veterans 2 14jim912No ratings yet
- Gerke Pildora - Preciosa Nov20 PDFDocument22 pagesGerke Pildora - Preciosa Nov20 PDFgonzalez1No ratings yet
- A History of Manipulative Therapy Through The Ages and Up To The Current Controversy in The United StatesDocument13 pagesA History of Manipulative Therapy Through The Ages and Up To The Current Controversy in The United Statesliz100% (1)
- 099 - VaccinesDocument4 pages099 - VaccinesArjan LallNo ratings yet
- Traditional Chinese Medicine in Taiwan 2021-7-6Document23 pagesTraditional Chinese Medicine in Taiwan 2021-7-6yandi permanaNo ratings yet
- OTC Ingredient List (Alphabetical by Ingredient) 9-21-10aDocument88 pagesOTC Ingredient List (Alphabetical by Ingredient) 9-21-10awindeleta0% (1)
- Natures Pharmacy E-BookDocument505 pagesNatures Pharmacy E-Bookcas100% (3)
- Koate DVIDocument7 pagesKoate DVIagnesroNo ratings yet
- Jurnal Triangle SpiderDocument17 pagesJurnal Triangle SpiderZuhdi Mahendra KotoNo ratings yet
- Clinical Practice Guidelines Critical Appraisal GuideDocument2 pagesClinical Practice Guidelines Critical Appraisal GuideWijitha VarenniNo ratings yet
- Accessory Guide Puritan Bennett 980 VentilatorDocument10 pagesAccessory Guide Puritan Bennett 980 VentilatortomNo ratings yet
- HIV Infection - Opportunistic InfectionsDocument21 pagesHIV Infection - Opportunistic InfectionszawadiNo ratings yet
- Gynecological ProceduresDocument17 pagesGynecological Proceduresjeelani saima100% (5)
- Partial E-Tool HA - Abdomen PDFDocument2 pagesPartial E-Tool HA - Abdomen PDFNicole BertulfoNo ratings yet
- List of Surgical ProceduresDocument3 pagesList of Surgical ProceduresAtto AmpereNo ratings yet
- FAQs Safe Practices For Medical InjectionsDocument7 pagesFAQs Safe Practices For Medical Injectionsjamesan00No ratings yet
- PiperacillinDocument3 pagesPiperacillinmyer pasandalanNo ratings yet
- Frudakis CV 09 19 2019 PharDocument14 pagesFrudakis CV 09 19 2019 PharTonyNo ratings yet
- Cancer Colon and Rectum (Wardah)Document23 pagesCancer Colon and Rectum (Wardah)WardahAliNo ratings yet
- Nursing Care Plan: Nursing Diagnosis Analysis Goal and Objectives Nursing Interventions Rationale EvaluationDocument3 pagesNursing Care Plan: Nursing Diagnosis Analysis Goal and Objectives Nursing Interventions Rationale EvaluationPaul Cubacub100% (1)
- Refractory Anaphylaxis Algorithm 2021Document1 pageRefractory Anaphylaxis Algorithm 2021BejinaruOanaSiCristiNo ratings yet