Download as pdf or txt
You might also like
- Freebie Bundle-50 PagesDocument75 pagesFreebie Bundle-50 PagesKarla Seravalli86% (7)
- DigestiveSystemSE - Activity CDocument11 pagesDigestiveSystemSE - Activity CYang Yang50% (2)
- (3F) Pediatrics - Pediatric HistoryDocument9 pages(3F) Pediatrics - Pediatric HistoryNomar Nonato100% (2)
- Group 1 Urinarytractinfections 2Document34 pagesGroup 1 Urinarytractinfections 2blessiejamNo ratings yet
- To Promote Good Hygiene and Physical Comfort.: Coli (E. Coli), NormallyDocument2 pagesTo Promote Good Hygiene and Physical Comfort.: Coli (E. Coli), NormallyFran LanNo ratings yet
- Benign Prostatic Hyperplasia. NCM 109Document16 pagesBenign Prostatic Hyperplasia. NCM 109Niña Jean Tormis AldabaNo ratings yet
- Funda Sample ScenarioDocument2 pagesFunda Sample ScenarioGadez JeanpelNo ratings yet
- Is Antibiotic Treatment Indicated in A Patient With A Positive Urine Culture But No SymptomsDocument4 pagesIs Antibiotic Treatment Indicated in A Patient With A Positive Urine Culture But No Symptomstsiko111No ratings yet
- Risk For Fluid VolumeDocument1 pageRisk For Fluid VolumeMariella BadongenNo ratings yet
- Nursing Care Plan TemplateDocument4 pagesNursing Care Plan TemplatetonnifritzcutamoraNo ratings yet
- Urinary Tract Infections Core Curriculum 2024Document11 pagesUrinary Tract Infections Core Curriculum 2024Amanda EscorciaNo ratings yet
- Urinary Tract Infection Core Curriculum 2024Document11 pagesUrinary Tract Infection Core Curriculum 2024JESSICA VELAZQUEZNo ratings yet
- Recurrent Urinary Tract Infection in Adult WomenDocument15 pagesRecurrent Urinary Tract Infection in Adult WomenSEPTIANA SAPUTRINo ratings yet
- Urinary Tract Infections Core Curriculum 2024 American Journal KidneyDocument11 pagesUrinary Tract Infections Core Curriculum 2024 American Journal Kidneycharliz diazNo ratings yet
- Iaat12i5p615 PDFDocument6 pagesIaat12i5p615 PDFsuresh kumar bakhtianiNo ratings yet
- Pyelonephritis 508Document8 pagesPyelonephritis 508Dery ZhibharanyNo ratings yet
- M1 - Urinary DisordersDocument2 pagesM1 - Urinary DisordersjuiceNo ratings yet
- Silvaqueenie Rose Multiple SclerosisDocument5 pagesSilvaqueenie Rose Multiple SclerosisQueenie SilvaNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Goals Intervention Rationale EvaluationDocument2 pagesNursing Care Plan: Assessment Diagnosis Goals Intervention Rationale EvaluationLeizel ApolonioNo ratings yet
- Peritonitis Bacteriana EspontaneaDocument1 pagePeritonitis Bacteriana EspontaneaInstituto Mexicano Seguro SocialNo ratings yet
- Impaired Urinary EliminationDocument2 pagesImpaired Urinary EliminationSiafei RabeNo ratings yet
- Case Study - Urinary Tract InfectionDocument10 pagesCase Study - Urinary Tract InfectionJiffy198867% (3)
- UTIsDocument25 pagesUTIsAnamul MasumNo ratings yet
- Case Study of Cholecystitis (Gallbladder Inflammation) ObjectiveDocument17 pagesCase Study of Cholecystitis (Gallbladder Inflammation) Objectivetalia hamedNo ratings yet
- Aquino NCP UtiDocument3 pagesAquino NCP UtiGianne ObaldoNo ratings yet
- Pharmacotherapy of Infectious Disease:: 6. Urinary Tract Infections and ProstatitisDocument26 pagesPharmacotherapy of Infectious Disease:: 6. Urinary Tract Infections and ProstatitisDigafe TolaNo ratings yet
- Urinary Incontinence - DiagnosisDocument2 pagesUrinary Incontinence - DiagnosisHoney Roselle MorenoNo ratings yet
- CC Orina PurpuraDocument2 pagesCC Orina PurpuraSusan RamosNo ratings yet
- Group Iv - Urinary Elimination PDFDocument96 pagesGroup Iv - Urinary Elimination PDFMeshezabel AsentistaNo ratings yet
- Pancreatic Pseudocyst Mimicking A Left Kidney Abscess: A Case ReportDocument3 pagesPancreatic Pseudocyst Mimicking A Left Kidney Abscess: A Case Reportdarlen bahriNo ratings yet
- Urinary Tract Infection UTI and Dementia FactsheetDocument10 pagesUrinary Tract Infection UTI and Dementia FactsheettoobaziNo ratings yet
- Does My Patient Need To Be Screened or Treated For A Urinary Tract InfectionDocument4 pagesDoes My Patient Need To Be Screened or Treated For A Urinary Tract Infectiontsiko111No ratings yet
- F. NCP ProperDocument4 pagesF. NCP ProperAle SandraNo ratings yet
- Rinary Ract Nfections: Classification Pathophysiology Risk Factors Clinical Manifestation DiagnosticsDocument27 pagesRinary Ract Nfections: Classification Pathophysiology Risk Factors Clinical Manifestation DiagnosticsDARYmagpantayNo ratings yet
- Constipation: Patient Name: Shehzad Age: 45 Ward: Emergency BDocument2 pagesConstipation: Patient Name: Shehzad Age: 45 Ward: Emergency BShafiq Ur RahmanNo ratings yet
- Benign Prostatic HyperplasiaDocument9 pagesBenign Prostatic Hyperplasiamardsz100% (1)
- Educational Module For Nursing Assistants in Long-Term Care Facilities: Urinary Tract Infections and Asymptomatic BacteriuriaDocument35 pagesEducational Module For Nursing Assistants in Long-Term Care Facilities: Urinary Tract Infections and Asymptomatic BacteriuriaPH Ph GnsoNo ratings yet
- Coralie Therese D. Dimacali, MD, FPCP, FPSNDocument48 pagesCoralie Therese D. Dimacali, MD, FPCP, FPSNJose Ph YuNo ratings yet
- Awais - Revision. 2015Document24 pagesAwais - Revision. 2015Michael Stevent Cuellar RodriguezNo ratings yet
- IVU en El Adulto MayorDocument8 pagesIVU en El Adulto MayorAndres Sebastian TorresNo ratings yet
- Davao Doctors College Nursing Program Nursing Care PlanDocument3 pagesDavao Doctors College Nursing Program Nursing Care PlanPRINCESS KOBAYASHINo ratings yet
- Subjective: Nephrolithiasis Is STO: After 8 Diagnostics: STO: Fully MetDocument3 pagesSubjective: Nephrolithiasis Is STO: After 8 Diagnostics: STO: Fully MetSebastianNo ratings yet
- CDU Care Plan. UTIDocument7 pagesCDU Care Plan. UTImutiso mutieNo ratings yet
- Urinary Tract Infection in Children: DR Nada Qawasmi Alquds Faculty of MedicineDocument25 pagesUrinary Tract Infection in Children: DR Nada Qawasmi Alquds Faculty of Medicineولاء إبراهيمNo ratings yet
- OB - Renal and Urinary Tract Disorders (RCB)Document5 pagesOB - Renal and Urinary Tract Disorders (RCB)Darren Mae MosadaNo ratings yet
- Pregnancy Induced Urinary Tract Changes Urinary Tract InfectionsDocument5 pagesPregnancy Induced Urinary Tract Changes Urinary Tract InfectionsDilausan B MolukNo ratings yet
- Notes On Urinary DisordersDocument3 pagesNotes On Urinary DisordersJAY TOM BOLIVARNo ratings yet
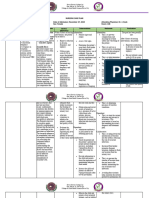
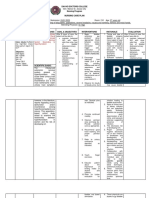
- University of The Assumption: College of Nursing Level Ii Related Nursing Experience Nursing Care PlanDocument3 pagesUniversity of The Assumption: College of Nursing Level Ii Related Nursing Experience Nursing Care PlanEugene MananganNo ratings yet
- Benign Prostatic Hyperplasia (BPH) : Free Nursing LecturesDocument8 pagesBenign Prostatic Hyperplasia (BPH) : Free Nursing Lecturesmeshael_29No ratings yet
- Clinical Analysis: I. Patient's ProfileDocument19 pagesClinical Analysis: I. Patient's ProfileKathleen DimacaliNo ratings yet
- Deficient Knowledge Related To Urinary Tract Infection: "Di Ako Aware About Sa UTI"as Verbalized by The ClientDocument2 pagesDeficient Knowledge Related To Urinary Tract Infection: "Di Ako Aware About Sa UTI"as Verbalized by The ClientSeanmarie CabralesNo ratings yet
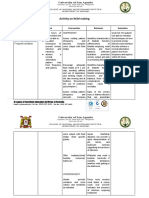
- Activity On NCM MakingDocument4 pagesActivity On NCM MakingJollan Marie BuenvenidaNo ratings yet
- Thesis Statement For Urinary Tract InfectionDocument7 pagesThesis Statement For Urinary Tract Infectionaflnbwmjhdinys100% (2)
- MONIS, Clemcy Pearl A. (NCP 103)Document5 pagesMONIS, Clemcy Pearl A. (NCP 103)Clemcy Pearl MonisNo ratings yet
- Uti Asbu Guidance FinalDocument14 pagesUti Asbu Guidance FinalJohn Vincent Dy OcampoNo ratings yet
- Evaluation of ConstipationDocument8 pagesEvaluation of ConstipationAndrea GallegoNo ratings yet
- Urinary Tract InfectionDocument14 pagesUrinary Tract InfectionSilva RahmaNo ratings yet
- Hematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesFrom EverandHematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesRating: 5 out of 5 stars5/5 (2)
- A Simple Guide to Pancreatitis, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Pancreatitis, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Comprehensive Insights into Acute Cystitis: Understanding, Management, and Future DirectionsFrom EverandComprehensive Insights into Acute Cystitis: Understanding, Management, and Future DirectionsNo ratings yet
- Post-cholecystectomy Bile Duct InjuryFrom EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorNo ratings yet
- A Simple Guide To Nocturia, (Excessive Night Urination) Diagnosis, Treatment And Related ConditionsFrom EverandA Simple Guide To Nocturia, (Excessive Night Urination) Diagnosis, Treatment And Related ConditionsNo ratings yet
- JAAPA Article - Staying Up To Date With JNC 8 HTN Guideline - H FeldmanDocument7 pagesJAAPA Article - Staying Up To Date With JNC 8 HTN Guideline - H FeldmanNomar NonatoNo ratings yet
- Wedding MassDocument19 pagesWedding MassNomar NonatoNo ratings yet
- Price ListDocument6 pagesPrice ListNomar NonatoNo ratings yet
- December 2010 Nurse Licensure Examination ResultsDocument595 pagesDecember 2010 Nurse Licensure Examination ResultsFilipino Nurses CentralNo ratings yet
- 11 Humss B Perdev Group 9 Brain Theory - 20231017 - 100244 - 0000Document22 pages11 Humss B Perdev Group 9 Brain Theory - 20231017 - 100244 - 0000Marilou PerochoNo ratings yet
- Mid Im 2020 AnatomyDocument178 pagesMid Im 2020 AnatomyXzailheene Dela FuenteNo ratings yet
- Acit TrainingDocument23 pagesAcit TrainingTheoNo ratings yet
- Psychology: Test Booklet NoDocument24 pagesPsychology: Test Booklet NokodalidhanaNo ratings yet
- O&G CompendiumDocument676 pagesO&G Compendiumwalefamous100% (1)
- ATCM JOURNAL September 2014 - 21Document60 pagesATCM JOURNAL September 2014 - 21Ivonne Flores FernándezNo ratings yet
- Yogic Sthula VyayamaDocument11 pagesYogic Sthula VyayamaGerardo Antonio Contreras Guerrero100% (7)
- Frog Dissection Worksheet With Virtual DissectionDocument3 pagesFrog Dissection Worksheet With Virtual DissectionTyrone Marius EarnestNo ratings yet
- Characteristics of Stabilizer Muscles A Systematic ReviewDocument11 pagesCharacteristics of Stabilizer Muscles A Systematic ReviewIvan MuñozNo ratings yet
- Ba MintonDocument15 pagesBa MintonKristel Joyce FortusNo ratings yet
- Mechanosensitive Ion Channels Contribute To MechanDocument9 pagesMechanosensitive Ion Channels Contribute To MechanHugues PetitjeanNo ratings yet
- DXN Ganoderma: Meet The King of HerbsDocument10 pagesDXN Ganoderma: Meet The King of HerbsBir Tamang TheengNo ratings yet
- Microbial Biopolymer: Pullulan Gellan Gum Dextran Xanthan GumDocument93 pagesMicrobial Biopolymer: Pullulan Gellan Gum Dextran Xanthan GumDewi WijayantiNo ratings yet
- Ophthalmology Lectures PDFDocument88 pagesOphthalmology Lectures PDFsharenNo ratings yet
- Teaching Plan 7Document61 pagesTeaching Plan 7dinman_rituraj1683No ratings yet
- Inotropic Drugs: DR S A Jayaratne Dept of PharmacologyDocument21 pagesInotropic Drugs: DR S A Jayaratne Dept of PharmacologyanojanNo ratings yet
- Nervous System and Sense Organ in FishDocument6 pagesNervous System and Sense Organ in FishAdarsh SenNo ratings yet
- Biomechanics in Total Hip Arthroplasty: Dr. Jose AustineDocument48 pagesBiomechanics in Total Hip Arthroplasty: Dr. Jose AustinePankaj VatsaNo ratings yet
- BIO.1.Test Bank (MEO) 2nd EditionDocument247 pagesBIO.1.Test Bank (MEO) 2nd Editionshady.1422026No ratings yet
- 39.2 Laparoscopic Adrenalectomy: Ahmad Assalia, M.D. Michel Gagner, M.D., FACS, FRCSCDocument13 pages39.2 Laparoscopic Adrenalectomy: Ahmad Assalia, M.D. Michel Gagner, M.D., FACS, FRCSCimherestudyingNo ratings yet
- Isolation and Characterization of CarbohydratesDocument4 pagesIsolation and Characterization of CarbohydratesJearweine FormaranNo ratings yet
- Haematology and Some Serum Parameters of BroilersDocument13 pagesHaematology and Some Serum Parameters of BroilersDanladi Idris HassanNo ratings yet
- Surgery I #3 - Fluid and ElectrolytesDocument9 pagesSurgery I #3 - Fluid and ElectrolytesCarl Earvin L. Favorito100% (1)
- Flowering Pathway in Arabidopsis-CouplandDocument3 pagesFlowering Pathway in Arabidopsis-CouplandJay Prakash MauryaNo ratings yet
- Nursing Care The Mechanical VentilatedDocument11 pagesNursing Care The Mechanical VentilatedIchal faisNo ratings yet
- EntomologyDocument50 pagesEntomologyapi-19960301100% (1)
- Read The Given Passage and Answer The Questions That FollowDocument3 pagesRead The Given Passage and Answer The Questions That Followapi-3850829No ratings yet
- Botanical Actions Reference Sheet: Botanical Action Description Physiology ExamplesDocument2 pagesBotanical Actions Reference Sheet: Botanical Action Description Physiology ExamplesDeo DoktorNo ratings yet