
Plexo Lumbar
Plexo Lumbar
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- Stephen M. Kosslyn, Robin S Rosenberg - Introducing Psychology - Brain, Person, Group (Pearson New International Edition) - Pearson (2013)Document549 pagesStephen M. Kosslyn, Robin S Rosenberg - Introducing Psychology - Brain, Person, Group (Pearson New International Edition) - Pearson (2013)Hinduism Ebooks67% (3)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Deloviar Cell Organelle Review Worksheet 1Document4 pagesDeloviar Cell Organelle Review Worksheet 1daRain100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Donovans Brain - Curt-Siodmak PDFDocument66 pagesDonovans Brain - Curt-Siodmak PDFBob AvocadoNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- NASA - Guidelines For Management of Circadian DesynchronyDocument47 pagesNASA - Guidelines For Management of Circadian DesynchronyJab100% (1)
- Dental and Medical MnemonicsDocument5 pagesDental and Medical MnemonicsRoshni GehlotNo ratings yet
- Module 5 Death 3Document25 pagesModule 5 Death 3Nhelly Anne NiedoNo ratings yet
- Science Material - Plants Move (Nasti) (III) PDFDocument2 pagesScience Material - Plants Move (Nasti) (III) PDFFransiska ArethaNo ratings yet
- Stimuli & Responses in PlantsDocument3 pagesStimuli & Responses in PlantsNasiruddin KutatNo ratings yet
- TSCUH Trachy Bed Head PDFDocument4 pagesTSCUH Trachy Bed Head PDFTudistef Analize SanatateNo ratings yet
- Cell Structure and Functions PDFDocument92 pagesCell Structure and Functions PDFAishaizl100% (1)
- SARS PowerpointDocument44 pagesSARS PowerpointXinn Xinn Vanzandt100% (1)
- What Is Physical FitnessDocument10 pagesWhat Is Physical FitnessMaria Cassandra O. RamosNo ratings yet
- Presenter: Dr. Nishant Shah M.V.Sc. (Medicine)Document104 pagesPresenter: Dr. Nishant Shah M.V.Sc. (Medicine)Santosh BhandariNo ratings yet
- Exocrine GlandsDocument9 pagesExocrine GlandsooiszehuiNo ratings yet
- Biology Practical For Class 11 CBSEDocument13 pagesBiology Practical For Class 11 CBSEHarmanpreet SinghNo ratings yet
- A Summary Table of Reabsorption and Secretion Along The Nephron - Anatomy & PhysiologyDocument2 pagesA Summary Table of Reabsorption and Secretion Along The Nephron - Anatomy & Physiologyshirley118650% (2)
- GE1137 Movies and Psychology: EmotionDocument45 pagesGE1137 Movies and Psychology: EmotionHenry LawNo ratings yet
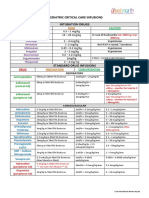
- Paediatric Critical Care Infusions Intubation DrugsDocument2 pagesPaediatric Critical Care Infusions Intubation DrugsА. Сосорбарам100% (1)
- Respiration ProcessDocument25 pagesRespiration ProcessSheena Talento GumbaNo ratings yet
- Invertebrates 1 @chetanbhagatDocument269 pagesInvertebrates 1 @chetanbhagatEka Dyah ANo ratings yet
- Agosto - Pe101 HandoutDocument17 pagesAgosto - Pe101 HandoutIvan AlcomendrasNo ratings yet
- Heredotary NeuropathiesDocument14 pagesHeredotary NeuropathiesRabecca Banda GrayNo ratings yet
- Brain TumorDocument18 pagesBrain TumorSKSAIDINESH100% (1)
- DeliriumDocument53 pagesDeliriumakinpe1No ratings yet
- (Surg2) 5.1b Introduction To Anesthesia-Part 2Document16 pages(Surg2) 5.1b Introduction To Anesthesia-Part 2AlloiBialbaNo ratings yet
- Omsb Part I - 2010Document10 pagesOmsb Part I - 2010Firyal Balushi100% (1)
- Art Therapy. and MindfulnessdocxDocument14 pagesArt Therapy. and MindfulnessdocxcarmellaNo ratings yet
- JBMT-2010-Muscle Fascia and Force TransmissionDocument7 pagesJBMT-2010-Muscle Fascia and Force TransmissionludimilaGNo ratings yet
- Skin - Structure and Function Flashcards - QuizletDocument5 pagesSkin - Structure and Function Flashcards - QuizletDani AnyikaNo ratings yet
- CHOLECYSTITISDocument13 pagesCHOLECYSTITISdolly joy100% (1)





































































Download as docx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- Stephen M. Kosslyn, Robin S Rosenberg - Introducing Psychology - Brain, Person, Group (Pearson New International Edition) - Pearson (2013)Document549 pagesStephen M. Kosslyn, Robin S Rosenberg - Introducing Psychology - Brain, Person, Group (Pearson New International Edition) - Pearson (2013)Hinduism Ebooks67% (3)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Deloviar Cell Organelle Review Worksheet 1Document4 pagesDeloviar Cell Organelle Review Worksheet 1daRain100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Donovans Brain - Curt-Siodmak PDFDocument66 pagesDonovans Brain - Curt-Siodmak PDFBob AvocadoNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- NASA - Guidelines For Management of Circadian DesynchronyDocument47 pagesNASA - Guidelines For Management of Circadian DesynchronyJab100% (1)
- Dental and Medical MnemonicsDocument5 pagesDental and Medical MnemonicsRoshni GehlotNo ratings yet
- Module 5 Death 3Document25 pagesModule 5 Death 3Nhelly Anne NiedoNo ratings yet
- Science Material - Plants Move (Nasti) (III) PDFDocument2 pagesScience Material - Plants Move (Nasti) (III) PDFFransiska ArethaNo ratings yet
- Stimuli & Responses in PlantsDocument3 pagesStimuli & Responses in PlantsNasiruddin KutatNo ratings yet
- TSCUH Trachy Bed Head PDFDocument4 pagesTSCUH Trachy Bed Head PDFTudistef Analize SanatateNo ratings yet
- Cell Structure and Functions PDFDocument92 pagesCell Structure and Functions PDFAishaizl100% (1)
- SARS PowerpointDocument44 pagesSARS PowerpointXinn Xinn Vanzandt100% (1)
- What Is Physical FitnessDocument10 pagesWhat Is Physical FitnessMaria Cassandra O. RamosNo ratings yet
- Presenter: Dr. Nishant Shah M.V.Sc. (Medicine)Document104 pagesPresenter: Dr. Nishant Shah M.V.Sc. (Medicine)Santosh BhandariNo ratings yet
- Exocrine GlandsDocument9 pagesExocrine GlandsooiszehuiNo ratings yet
- Biology Practical For Class 11 CBSEDocument13 pagesBiology Practical For Class 11 CBSEHarmanpreet SinghNo ratings yet
- A Summary Table of Reabsorption and Secretion Along The Nephron - Anatomy & PhysiologyDocument2 pagesA Summary Table of Reabsorption and Secretion Along The Nephron - Anatomy & Physiologyshirley118650% (2)
- GE1137 Movies and Psychology: EmotionDocument45 pagesGE1137 Movies and Psychology: EmotionHenry LawNo ratings yet
- Paediatric Critical Care Infusions Intubation DrugsDocument2 pagesPaediatric Critical Care Infusions Intubation DrugsА. Сосорбарам100% (1)
- Respiration ProcessDocument25 pagesRespiration ProcessSheena Talento GumbaNo ratings yet
- Invertebrates 1 @chetanbhagatDocument269 pagesInvertebrates 1 @chetanbhagatEka Dyah ANo ratings yet
- Agosto - Pe101 HandoutDocument17 pagesAgosto - Pe101 HandoutIvan AlcomendrasNo ratings yet
- Heredotary NeuropathiesDocument14 pagesHeredotary NeuropathiesRabecca Banda GrayNo ratings yet
- Brain TumorDocument18 pagesBrain TumorSKSAIDINESH100% (1)
- DeliriumDocument53 pagesDeliriumakinpe1No ratings yet
- (Surg2) 5.1b Introduction To Anesthesia-Part 2Document16 pages(Surg2) 5.1b Introduction To Anesthesia-Part 2AlloiBialbaNo ratings yet
- Omsb Part I - 2010Document10 pagesOmsb Part I - 2010Firyal Balushi100% (1)
- Art Therapy. and MindfulnessdocxDocument14 pagesArt Therapy. and MindfulnessdocxcarmellaNo ratings yet
- JBMT-2010-Muscle Fascia and Force TransmissionDocument7 pagesJBMT-2010-Muscle Fascia and Force TransmissionludimilaGNo ratings yet
- Skin - Structure and Function Flashcards - QuizletDocument5 pagesSkin - Structure and Function Flashcards - QuizletDani AnyikaNo ratings yet
- CHOLECYSTITISDocument13 pagesCHOLECYSTITISdolly joy100% (1)