Download as docx, pdf, or txt
You might also like
- Med Bed Info From Skye PrinceDocument9 pagesMed Bed Info From Skye PrinceTim0% (1)
- Child Abuse Thesis (Introduction)Document4 pagesChild Abuse Thesis (Introduction)van83% (24)
- Research Topic:: Child Abuse As A Reason For Psychological Drawback of Children in Later LifeDocument15 pagesResearch Topic:: Child Abuse As A Reason For Psychological Drawback of Children in Later Life41-ISHRTA JAHAN LLM 11TH BATCH jahanNo ratings yet
- Pasi CalculatorDocument4 pagesPasi CalculatorBimo Aryo TejoNo ratings yet
- Annotated BibliographyDocument5 pagesAnnotated Bibliographyapi-399404406100% (2)
- Child AbuseDocument8 pagesChild AbuseUzair RiazNo ratings yet
- Case Write Up-DengueDocument16 pagesCase Write Up-DengueSyafi'ie Syukri100% (1)
- The Effect of Abuse Among Children in Conflict With The Law in Bahay Pag-AsaDocument13 pagesThe Effect of Abuse Among Children in Conflict With The Law in Bahay Pag-AsaMarlone Clint CamilonNo ratings yet
- Sample 1Document5 pagesSample 1gjplineNo ratings yet
- ThesisDocument7 pagesThesisKim Nguyễn Mai ThiênNo ratings yet
- Child Abuse Final DraftDocument10 pagesChild Abuse Final Draftapi-272816863No ratings yet
- Spanking Debate Term Paper Rough Draft-1Document7 pagesSpanking Debate Term Paper Rough Draft-1Krystal Mae LopezNo ratings yet
- Aggression in ChildrenDocument5 pagesAggression in ChildrenRizki TiyasNo ratings yet
- The Impacts of Child Abuse On Mental Health - EditedDocument9 pagesThe Impacts of Child Abuse On Mental Health - EditedJohn Muthama MbathiNo ratings yet
- Attachment Theory and Child AbuseDocument7 pagesAttachment Theory and Child AbuseAlan Challoner100% (3)
- Project Proposal MathDocument5 pagesProject Proposal MathLorenz Philip AriasNo ratings yet
- Assignment 2 - Siblings ViolenceDocument9 pagesAssignment 2 - Siblings Violencewafin wardahNo ratings yet
- Origins of Violent BehaviorDocument5 pagesOrigins of Violent BehaviorCatherineNo ratings yet
- BullyingDocument9 pagesBullyingGreer LevendalNo ratings yet
- Effects of Domestic Violence To Children: A Literature ReviewDocument13 pagesEffects of Domestic Violence To Children: A Literature ReviewJoefritzVaronNo ratings yet
- Defining Child Sexual AbuseDocument14 pagesDefining Child Sexual AbuseAndreas Springfield GleasonNo ratings yet
- DCFS: Medical Lens IRRDocument6 pagesDCFS: Medical Lens IRRdiyaNo ratings yet
- Research Paper On Emotional AbuseDocument8 pagesResearch Paper On Emotional Abusevehysad1s1w3100% (1)
- Research Final g11Document45 pagesResearch Final g11Adrian CasajeNo ratings yet
- AggressionDocument9 pagesAggressionapi-645961517No ratings yet
- LX20221116 461Document11 pagesLX20221116 461Abdullah AkhtarNo ratings yet
- Self Esteem Research PaperDocument4 pagesSelf Esteem Research Paperapi-36216667480% (5)
- Index: SR No. ParticularsDocument10 pagesIndex: SR No. Particularstarang1994No ratings yet
- Digitized Text Final Draft 2Document7 pagesDigitized Text Final Draft 2api-253375096No ratings yet
- Juvenile DelinquencyDocument5 pagesJuvenile DelinquencyIsaac AbrahamsonNo ratings yet
- 1302 Essay 3 Draft 3 CompleteDocument6 pages1302 Essay 3 Draft 3 Completeapi-667528548No ratings yet
- Review of Related Literature This Chapter We Will Present The Related Topics in Our Study. The Topics Here WillDocument5 pagesReview of Related Literature This Chapter We Will Present The Related Topics in Our Study. The Topics Here WillJohnLloyd O. Aviles100% (1)
- Spanking/Corporal PunishmentDocument6 pagesSpanking/Corporal Punishmentchamp8174782No ratings yet
- Domestic Violence RP Final - Abby JollayDocument9 pagesDomestic Violence RP Final - Abby Jollayapi-510559624No ratings yet
- Community Problem ReportDocument9 pagesCommunity Problem Reportapi-385897772No ratings yet
- Pakistan Journal of Social SciencesDocument5 pagesPakistan Journal of Social SciencesJessica Marie Borromeo DHumNo ratings yet
- Psychology Scholarly Paper 1Document11 pagesPsychology Scholarly Paper 1Danial HassanNo ratings yet
- Research Paper 2Document7 pagesResearch Paper 2api-242357005No ratings yet
- ArticleDocument19 pagesArticleNhpa foundationNo ratings yet
- Psychological Effects of BullyingDocument11 pagesPsychological Effects of BullyingnyunsNo ratings yet
- Sofia Ailyn Navarro - Literature Review Final DraftDocument7 pagesSofia Ailyn Navarro - Literature Review Final Draftapi-710656920No ratings yet
- Chapter 1 BookbindDocument12 pagesChapter 1 Bookbindej.lucasan15No ratings yet
- Soc Research PaperDocument8 pagesSoc Research Paperapi-317705401No ratings yet
- Running Head: Etiology of Bullying 1Document5 pagesRunning Head: Etiology of Bullying 1Kamau RobertNo ratings yet
- The Impact of Bullying in School On The ChildrenDocument29 pagesThe Impact of Bullying in School On The ChildrenJumaryse Marabut100% (5)
- Child AbuseDocument6 pagesChild Abuseghanta007No ratings yet
- Foster Care IrrDocument7 pagesFoster Care Irrapi-530384945100% (1)
- Literary Criticism PaperDocument21 pagesLiterary Criticism PaperJasper De TorresNo ratings yet
- Childhood Bullying: Implications For PhysiciansDocument6 pagesChildhood Bullying: Implications For PhysiciansMaría Susana López G.No ratings yet
- Research Project On Domestic Violence (Autosaved) 2Document7 pagesResearch Project On Domestic Violence (Autosaved) 2Elvis MangisiNo ratings yet
- Reasearch Proposal Group Work (AutoRecovered)Document13 pagesReasearch Proposal Group Work (AutoRecovered)SSENYANGENo ratings yet
- Child Maltreatment: MessingerDocument46 pagesChild Maltreatment: MessingerjzariziNo ratings yet
- Childhood Trauma:Impact On Personality/Role in Personality DisordersDocument13 pagesChildhood Trauma:Impact On Personality/Role in Personality DisordersNancee Y.No ratings yet
- Effects of Bad Parenting On Children: Love KnowDocument3 pagesEffects of Bad Parenting On Children: Love KnowStudent1010No ratings yet
- Team Anonymous FInal ProposalDocument10 pagesTeam Anonymous FInal ProposalAdhaNo ratings yet
- Is Criminal Behavior Innate or Shaped by EnvironmentDocument5 pagesIs Criminal Behavior Innate or Shaped by EnvironmentAnia TimashkovaNo ratings yet
- Correlation Between Child Abuse and Future Violent BehaviourDocument6 pagesCorrelation Between Child Abuse and Future Violent BehaviourNathan RonoNo ratings yet
- Psychological Studies Captones: Student's Name Instructor's Name Course DateDocument21 pagesPsychological Studies Captones: Student's Name Instructor's Name Course DatejobNo ratings yet
- Senior PaperDocument7 pagesSenior Paperapi-300517496No ratings yet
- Consequences of Child Abuse On Psychological Well-BeingDocument22 pagesConsequences of Child Abuse On Psychological Well-Being4tfhfbwcptNo ratings yet
- RESEARCH2 CompleteChaptersDocument38 pagesRESEARCH2 CompleteChaptersZairah SantosNo ratings yet
- Generational Shadows: Breaking the Cycle of Parental DysfunctionFrom EverandGenerational Shadows: Breaking the Cycle of Parental DysfunctionNo ratings yet
- Shaping Your Child's Healthy Self-Esteem-Self-Worth: Emotional IntelligenceFrom EverandShaping Your Child's Healthy Self-Esteem-Self-Worth: Emotional IntelligenceNo ratings yet
- CVDocument5 pagesCVapi-347484976No ratings yet
- Resume2017 FinalDocument2 pagesResume2017 Finalapi-347484976No ratings yet
- Exec Sum FinalDocument4 pagesExec Sum Finalapi-347484976No ratings yet
- Final Policy BriefDocument4 pagesFinal Policy Briefapi-347484976No ratings yet
- Creating A Geriatric Emergency Department John Schumacher Full Chapter PDFDocument69 pagesCreating A Geriatric Emergency Department John Schumacher Full Chapter PDFmourdegoma100% (5)
- S M A R T: 201 A TEST #3 Define and Discuss The Purpose of Outcome IdentificationDocument6 pagesS M A R T: 201 A TEST #3 Define and Discuss The Purpose of Outcome IdentificationLindsay JonesNo ratings yet
- Pga 2014 ProspectusDocument31 pagesPga 2014 ProspectusKaranGargNo ratings yet
- Gibb's Reflective Cycle: DescriptionDocument3 pagesGibb's Reflective Cycle: DescriptionLarr SumalpongNo ratings yet
- 10besar Kode PenyakitDocument5 pages10besar Kode PenyakitDEWINo ratings yet
- EthicsDocument10 pagesEthicsMadhubala JNo ratings yet
- Table Tennis Lesson PlanDocument3 pagesTable Tennis Lesson Planapi-216084231No ratings yet
- HPLC Article - 1Document8 pagesHPLC Article - 1akkimipadmaNo ratings yet
- Mutagenèse Et Cancérogenèse: Gwenaëlle IarmarcovaiDocument10 pagesMutagenèse Et Cancérogenèse: Gwenaëlle Iarmarcovaibouchakour meryemNo ratings yet
- Deep Fat FryingDocument2 pagesDeep Fat FryingalinawidagdoNo ratings yet
- Determination 446 Pesticides Residue by GC Ms and LC MsDocument32 pagesDetermination 446 Pesticides Residue by GC Ms and LC MsMohammed ELAbadsaNo ratings yet
- Soal Inggris - 2Document6 pagesSoal Inggris - 2vivitrisami05No ratings yet
- The Effects of Emotion On Short-Term Power Spectrum Analysis of Heart RateDocument5 pagesThe Effects of Emotion On Short-Term Power Spectrum Analysis of Heart RateManuel Guerrero GómezNo ratings yet
- 3 - Chemical Reactions of Fat and OilsDocument16 pages3 - Chemical Reactions of Fat and Oilssha_bee100% (1)
- Rehabilitation MedicaleDocument458 pagesRehabilitation MedicaleactoneNo ratings yet
- Lp-Grade 10 HealthDocument17 pagesLp-Grade 10 HealthJovelyn TakilidNo ratings yet
- Which of The Following Is NOT True About Dust?Document3 pagesWhich of The Following Is NOT True About Dust?lucel palaca100% (1)
- Case Study 8 Construction SafetyDocument2 pagesCase Study 8 Construction SafetyJerome BricenioNo ratings yet
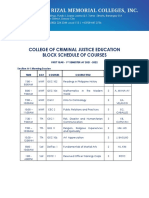
- College of Criminal Justice Education Block Schedule of CoursesDocument12 pagesCollege of Criminal Justice Education Block Schedule of CoursesKristel Ann ManlangitNo ratings yet
- 16012019FV4Q6RWBAnnexure documentofEIAEMP PDFDocument400 pages16012019FV4Q6RWBAnnexure documentofEIAEMP PDFJainam Shah100% (1)
- Managing Our Waste: Powerpoint Slides Prepared by Stephen TurnbullDocument59 pagesManaging Our Waste: Powerpoint Slides Prepared by Stephen TurnbullJulia HartNo ratings yet
- Medical Condition Report Free PDF TemplateDocument2 pagesMedical Condition Report Free PDF Templateapi-340236228No ratings yet
- The Manual of Ethiopian Medical History - People To People PDFDocument60 pagesThe Manual of Ethiopian Medical History - People To People PDFShiferaw Biru100% (1)
- Diet For Patient With Parkinson's DiseaseDocument2 pagesDiet For Patient With Parkinson's DiseaseNuzulina SafiraNo ratings yet
- Annual Barangay Youth Investment Program (Abyip)Document4 pagesAnnual Barangay Youth Investment Program (Abyip)Nhelyn Manuel0% (1)
- New Lipid PowerpointDocument113 pagesNew Lipid PowerpointMadane Jamila Amerol SaminNo ratings yet
- Swimming Pools and Spa Pools: Standard For The Operation ofDocument40 pagesSwimming Pools and Spa Pools: Standard For The Operation ofakramNo ratings yet