Download as docx, pdf, or txt
You might also like
- Nursing Care Plan Post Op & Intra OpDocument2 pagesNursing Care Plan Post Op & Intra OpLei Ortega85% (48)
- NURSING CARE PLAN of Hodgkin's Lymphoma: Assessment Nursing Diagnosis Planning Nursing Interventions Rationale EvaluationDocument5 pagesNURSING CARE PLAN of Hodgkin's Lymphoma: Assessment Nursing Diagnosis Planning Nursing Interventions Rationale Evaluationjoyrena ochondraNo ratings yet
- Sac Training Guide 2019 Final PDFDocument49 pagesSac Training Guide 2019 Final PDFArmando Santos100% (1)
- Nursing Care Plan For The Patient With Burn Injury - Acute Pain Related To Tissue and Nerve InjuryDocument2 pagesNursing Care Plan For The Patient With Burn Injury - Acute Pain Related To Tissue and Nerve InjuryAngel Garcia67% (3)
- Selenium Interview Questions - CognizantDocument20 pagesSelenium Interview Questions - CognizantJessie SokhiNo ratings yet
- AWS Vs Azure Vs Google Cloud - A Detailed Comparison of The Cloud Services Giants PDFDocument10 pagesAWS Vs Azure Vs Google Cloud - A Detailed Comparison of The Cloud Services Giants PDFSakthivel PNo ratings yet
- Manguiat, Ncma 111 RomeoDocument4 pagesManguiat, Ncma 111 RomeoCiara ManguiatNo ratings yet
- Brain Surgery Post Op NCPDocument6 pagesBrain Surgery Post Op NCPunnamed personNo ratings yet
- "I Don't Have An Infection in My Gallbladder Which Is Good, But I Do Feel The Pain," As Verbalized by TheDocument2 pages"I Don't Have An Infection in My Gallbladder Which Is Good, But I Do Feel The Pain," As Verbalized by Theunnamed person100% (1)
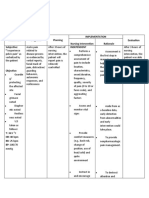
- Nursing Care Plan: Assessmen T (Cues / Clues) Nursing Diagnosis Rationale Planning Intervention Rationale Evaluatio NDocument7 pagesNursing Care Plan: Assessmen T (Cues / Clues) Nursing Diagnosis Rationale Planning Intervention Rationale Evaluatio NNajla Kaye PerezNo ratings yet
- Ms II NCPDocument2 pagesMs II NCPABIL ABU BAKARNo ratings yet
- DR OutputsDocument2 pagesDR OutputsRomm JacobNo ratings yet
- Acute PainDocument2 pagesAcute PainNicole Genevie MallariNo ratings yet
- NCP Case Pres Post OpDocument2 pagesNCP Case Pres Post OpKuda Gene LorenNo ratings yet
- Acute PainDocument4 pagesAcute PainIvan Jules P. PALMARESNo ratings yet
- NCP TemplateDocument4 pagesNCP TemplatebaleteaprileuniceNo ratings yet
- Vii. Nursing Care Plan Assessment Nursing Diagnosis Plan of Care Expected Outcome Evaluation Subjective: Independent: Short Term GoalDocument1 pageVii. Nursing Care Plan Assessment Nursing Diagnosis Plan of Care Expected Outcome Evaluation Subjective: Independent: Short Term Goalapi-3828211No ratings yet
- PBL1Document3 pagesPBL1clarNo ratings yet
- Cues Nursing Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Planning Intervention Rationale EvaluationBiancaGabatinoAbarcaNo ratings yet
- UntitledDocument22 pagesUntitledTheo Roi MusniNo ratings yet
- Nursing Care Plan Data NSG Diagnoses Goals & Outcomes NSG Interventions Rationale Evaluation Goal MetDocument3 pagesNursing Care Plan Data NSG Diagnoses Goals & Outcomes NSG Interventions Rationale Evaluation Goal MetClaudineNo ratings yet
- Acutepain RevisedDocument3 pagesAcutepain RevisedAndrea AutorNo ratings yet
- "Naga Pan Luya Lang Ang Lawas Ko"as Verbalized by The PatientDocument3 pages"Naga Pan Luya Lang Ang Lawas Ko"as Verbalized by The PatientJamie Grace AbitNo ratings yet
- NCPDocument3 pagesNCPHarland EstebanNo ratings yet
- NCP Acute Pain RT CancerDocument3 pagesNCP Acute Pain RT CancerCharissa Magistrado De LeonNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Short Term GoalDocument2 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Short Term GoalCayla Mae CarlosNo ratings yet
- NCP - GeriaDocument4 pagesNCP - GeriaMarielle J GarciaNo ratings yet
- NCP FormatDocument2 pagesNCP Formatheartberroya1721No ratings yet
- Acute Lymphocytic LeukemiaDocument2 pagesAcute Lymphocytic LeukemiaJustine ConuiNo ratings yet
- Concepcion NCPDocument2 pagesConcepcion NCPLevi ConcepcionNo ratings yet
- Pre-Operative (Incision & Drainage of Abscess)Document6 pagesPre-Operative (Incision & Drainage of Abscess)Eunice MañalacNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationRenea Joy ArruejoNo ratings yet
- Post-Operative Nursing Care Plan # 1Document14 pagesPost-Operative Nursing Care Plan # 1Vince John SevillaNo ratings yet
- Nursing Care Plan: University of San Jose-RecoletosDocument2 pagesNursing Care Plan: University of San Jose-RecoletosIvan A. EleginoNo ratings yet
- Alisa D&CDocument1 pageAlisa D&CJessmar AguirreNo ratings yet
- Nursing Care Plan Cesarian DeliveryDocument2 pagesNursing Care Plan Cesarian Deliveryderic97% (39)
- St. Paul University PhilippinesDocument3 pagesSt. Paul University PhilippinesMia Grace GarciaNo ratings yet
- Nursing Care Management: Assessment Diagnosis Goals and Objective Intervention and Rationale EvaluationDocument3 pagesNursing Care Management: Assessment Diagnosis Goals and Objective Intervention and Rationale EvaluationTyron ChuaNo ratings yet
- NCP FormatDocument1 pageNCP FormatNathaniel NograNo ratings yet
- Or - Nursing Care PlanDocument2 pagesOr - Nursing Care PlanDANIELLA MALARANG MELNo ratings yet
- NCPDocument6 pagesNCPKrishna Faith P. DelaraNo ratings yet
- Care PlanDocument2 pagesCare PlanAnonymous 9QBCcNNo ratings yet
- JoeoeoeoeDocument31 pagesJoeoeoeoeBSRT1A BERBANO, IAN JEWEL M.No ratings yet
- Sample Nursing Care PlanDocument1 pageSample Nursing Care PlanQuiannë Delos ReyesNo ratings yet
- NCP FractureDocument7 pagesNCP FractureMacris BondocNo ratings yet
- Nursing Care PlanDocument5 pagesNursing Care PlanLaceth Joyce T. LASATNo ratings yet
- NCP Drug Study KriziaDocument5 pagesNCP Drug Study KriziaAlexia AlbaniaNo ratings yet
- Pelagio, Shiena Mae B. BSN Ii-A CASE: Cervical Cancer Implementation Nursing Intervention Rationale Evaluation Subjective: "I Experience IndependentDocument2 pagesPelagio, Shiena Mae B. BSN Ii-A CASE: Cervical Cancer Implementation Nursing Intervention Rationale Evaluation Subjective: "I Experience IndependentShiena Mae PelagioNo ratings yet
- Postop Pain NcoDocument3 pagesPostop Pain NcofrizaNo ratings yet
- NCP PostpartumDocument6 pagesNCP PostpartumLovely Anne ArqueroNo ratings yet
- NCP-Septic Shock (Acute Pain)Document3 pagesNCP-Septic Shock (Acute Pain)Ted anadiloNo ratings yet
- AssessmentDocument1 pageAssessmentDianne ParungaoNo ratings yet
- Week 7 Careplan OnlyDocument2 pagesWeek 7 Careplan Onlyapi-381357393No ratings yet
- Fernandez NCP EditedDocument2 pagesFernandez NCP EditedRouwi DesiatcoNo ratings yet
- BSN 1 H Case Application Nursing Care PlanDocument3 pagesBSN 1 H Case Application Nursing Care PlanAntonio EscotoNo ratings yet
- NCP and Drug SheetDocument16 pagesNCP and Drug SheetLucil Jaine Abayan BellezaNo ratings yet
- Nursing Diagnosis: Impaired Physical Mobility Assessment Planning Intervention Rationale EvaluationDocument3 pagesNursing Diagnosis: Impaired Physical Mobility Assessment Planning Intervention Rationale EvaluationSheril Sularte CasanesNo ratings yet
- Assessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleDocument2 pagesAssessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleRhea Mae Valles - ReyesNo ratings yet
- Assessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsFrom EverandAssessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsNo ratings yet
- Mos-Installation Stainless Steel Eye Bolt Filter TankDocument5 pagesMos-Installation Stainless Steel Eye Bolt Filter Tankhabibullah.centroironNo ratings yet
- Statement of Principle Self-Care Including Self-Medication - The Professional Role of The PharmacistDocument5 pagesStatement of Principle Self-Care Including Self-Medication - The Professional Role of The PharmacistAprilia R. Permatasari0% (1)
- Jiabs 26-2Document197 pagesJiabs 26-2JIABSonline100% (1)
- TGDocument180 pagesTGavikram1984No ratings yet
- Indonesian Sign Language Visualization Model (BISINDO) Website-Based Oral Health On Tooth Brushing Behavior in Deaf ChildrenDocument6 pagesIndonesian Sign Language Visualization Model (BISINDO) Website-Based Oral Health On Tooth Brushing Behavior in Deaf ChildrenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- MTA uniVAL Technical Data Sheet v00Document1 pageMTA uniVAL Technical Data Sheet v00muhammetNo ratings yet
- ATS Kingston Heath CustomerDocument63 pagesATS Kingston Heath CustomerDevNo ratings yet
- CH 12Document31 pagesCH 12asin12336No ratings yet
- ClaytonDocument1 pageClaytonapi-3831340No ratings yet
- Understand Trading in 2 Hours SteveRyanDocument63 pagesUnderstand Trading in 2 Hours SteveRyanAkash Biswal100% (3)
- Glory To God Light From Light With LyricsDocument13 pagesGlory To God Light From Light With LyricsRodolfo DeriquitoNo ratings yet
- ICSE Class 10 Maths Chapter 14 Equation of A Straight LineDocument30 pagesICSE Class 10 Maths Chapter 14 Equation of A Straight LineAmit SharmaNo ratings yet
- Healthy Pregnancy Meals:: LAMB Doula and Birthing CenterDocument16 pagesHealthy Pregnancy Meals:: LAMB Doula and Birthing Centerapi-44273750No ratings yet
- CAPEX Acquisition ProcessDocument5 pagesCAPEX Acquisition ProcessRajaIshfaqHussainNo ratings yet
- Selection of Fuses For The Protection of TransformersDocument14 pagesSelection of Fuses For The Protection of Transformersgalaxyebn100% (11)
- GEC PE003 Module 1 CheckedDocument21 pagesGEC PE003 Module 1 CheckedJianica SalesNo ratings yet
- Tabel PeriodikDocument2 pagesTabel PeriodikNisrina KalyaNo ratings yet
- The Migration Industry and Future Directions For Migration PolicyDocument4 pagesThe Migration Industry and Future Directions For Migration PolicyGabriella VillaçaNo ratings yet
- S9 Safety Labeling For Electrical Equipment and Facilities ManagementDocument74 pagesS9 Safety Labeling For Electrical Equipment and Facilities Managementalfonzo.keilerNo ratings yet
- A Study of Emotional IntelligeDocument6 pagesA Study of Emotional Intelligekashish behlNo ratings yet
- Remanufactured Genuine Parts CatalogueDocument22 pagesRemanufactured Genuine Parts CatalogueHenrique CorreiaNo ratings yet
- System Development Invoice - Audit ToolDocument2 pagesSystem Development Invoice - Audit ToolVictorNo ratings yet
- Scala AccesoriesDocument27 pagesScala AccesoriesZiggy BussyNo ratings yet
- Pivot 4A Lesson Exemplar Using The Idea Instructional ProcessDocument14 pagesPivot 4A Lesson Exemplar Using The Idea Instructional ProcessJocelyn100% (1)
- Qi Project Poster Improving Nurse ResponsivnessDocument1 pageQi Project Poster Improving Nurse Responsivnessapi-446692943No ratings yet
- (THAAD) Five Failures and CountingDocument6 pages(THAAD) Five Failures and CountingGuilherme Da Silva CostaNo ratings yet
- Panasonic LCD TH-L32C30Document72 pagesPanasonic LCD TH-L32C30King King0% (1)