Download as pdf or txt
You might also like
- Manuskrip PDFDocument156 pagesManuskrip PDFFarhan FaturrohmanNo ratings yet
- Lactation Risk CategoriesDocument9 pagesLactation Risk CategoriesHandre PutraNo ratings yet
- Pe 10 Q2Document152 pagesPe 10 Q2Lanie Tamacio Baday85% (20)
- Explore Style, Books, and More!: InterpersonalDocument1 pageExplore Style, Books, and More!: InterpersonalMuhammad YusufNo ratings yet
- The Magnesium MiracleDocument8 pagesThe Magnesium Miracleapi-296898673100% (7)
- Diet Penyakit Ginjal Dan Saluran KemihDocument73 pagesDiet Penyakit Ginjal Dan Saluran KemihNurul AlfatarisyaNo ratings yet
- D070415 PDFDocument5 pagesD070415 PDFRosyid PrasetyoNo ratings yet
- Tugas Artikel AgustinDocument8 pagesTugas Artikel AgustinMiko WidiatmokoNo ratings yet
- Obat Dan Kehamilan, Drugs, Aman Untuk Ibu Hamil, FarmasiDocument13 pagesObat Dan Kehamilan, Drugs, Aman Untuk Ibu Hamil, FarmasifrankysukwendyNo ratings yet
- Effects of Adulterated Palm Cooking Oil On The Quality of Fried Chicken NuggetsDocument11 pagesEffects of Adulterated Palm Cooking Oil On The Quality of Fried Chicken NuggetsKiruthick DonNo ratings yet
- Typhoid Management Guidelines - 2019 - MMIDSPDocument14 pagesTyphoid Management Guidelines - 2019 - MMIDSPhasnah shintaNo ratings yet
- Gambaran Histopatologi Hepatosit Tikus Putih Setelah Pemberian Jintan Hitam Dosis 500mgkgbb, 1000mgkgbb, Dan 1500mgkgbb Selama 21 Hari (Subkronik)Document5 pagesGambaran Histopatologi Hepatosit Tikus Putih Setelah Pemberian Jintan Hitam Dosis 500mgkgbb, 1000mgkgbb, Dan 1500mgkgbb Selama 21 Hari (Subkronik)Mokhammad Faisol AbdullahNo ratings yet
- PhysioEx Exercise 5 Activity 1Document3 pagesPhysioEx Exercise 5 Activity 1villanuevaparedesaracely4No ratings yet
- Makalah 4 CMLDocument28 pagesMakalah 4 CMLMentari100% (1)
- Kolestasis Intrahepatal Vs EkstrahepatalDocument4 pagesKolestasis Intrahepatal Vs EkstrahepatalrikarikaNo ratings yet
- Anamnesis in EnglishDocument2 pagesAnamnesis in EnglishShania FikraNo ratings yet
- Daftar Obat Aman Dan Berbahaya Untuk Ibu Hamil DanDocument4 pagesDaftar Obat Aman Dan Berbahaya Untuk Ibu Hamil Daninne_fNo ratings yet
- Bhagani 2018Document7 pagesBhagani 2018rifky kurniawanNo ratings yet
- Patofisiologi Peptic UlcerDocument29 pagesPatofisiologi Peptic Ulceranindini winda amaliaNo ratings yet
- Farmakodinamik Obat Anti DiabetesDocument24 pagesFarmakodinamik Obat Anti DiabetesAsma Somadayo100% (1)
- Artikel Kesehatan Bahasa Inggris: Keeping Skin Healthy and Beautiful, Do Not Need Expensive!Document2 pagesArtikel Kesehatan Bahasa Inggris: Keeping Skin Healthy and Beautiful, Do Not Need Expensive!Anonymous IKgbeVoNo ratings yet
- Jurnal - Komponen DarahDocument6 pagesJurnal - Komponen Darahvivi maykasariNo ratings yet
- Konsensus DM Perkeni 2006 PDFDocument55 pagesKonsensus DM Perkeni 2006 PDFDenny LukasNo ratings yet
- Rehabilitasi AGA AGBDocument40 pagesRehabilitasi AGA AGBalwy sugiartoNo ratings yet
- Kalium KloratDocument6 pagesKalium KloratAnnisa Nur JNo ratings yet
- JNC 6 Vs 7Document2 pagesJNC 6 Vs 7Diwan AyuNo ratings yet
- Diagnosis Kanker Paru AzDocument20 pagesDiagnosis Kanker Paru AzTryanda SaidNo ratings yet
- n378.008 Iris Website Staging of CKD PDFDocument8 pagesn378.008 Iris Website Staging of CKD PDFrutebeufNo ratings yet
- ACLS Pointers Acute Pulmonary Edema Hypotension .7 PDFDocument2 pagesACLS Pointers Acute Pulmonary Edema Hypotension .7 PDFRisa HerlianitaNo ratings yet
- Signs, Symptoms and Health Problems: Etty Komariah S, S.Kp.,M.KepDocument14 pagesSigns, Symptoms and Health Problems: Etty Komariah S, S.Kp.,M.KepHimatul AliyahNo ratings yet
- Assignments For Inborn Errors of Metabolism (DR - DR Damayanti R.Sjarif, SpA (K)Document2 pagesAssignments For Inborn Errors of Metabolism (DR - DR Damayanti R.Sjarif, SpA (K)clementNo ratings yet
- Dosis Obat LengkapDocument52 pagesDosis Obat LengkapropusanNo ratings yet
- RL Vs NaclDocument12 pagesRL Vs NaclTri MaryantiNo ratings yet
- Stroke Disability and Physiotherapy Interventions: A Quantitative Evaluation of Physiotherapy Treatment Approaches' in ZambiaDocument9 pagesStroke Disability and Physiotherapy Interventions: A Quantitative Evaluation of Physiotherapy Treatment Approaches' in ZambiaPaulomds1991No ratings yet
- Hipertensi: Tekanan Darah TinggiDocument33 pagesHipertensi: Tekanan Darah TinggiErika SetyodiharjoNo ratings yet
- Laporan Faal RespirasiDocument18 pagesLaporan Faal RespirasiLatifah RBNo ratings yet
- Gigantisme Dan AkromegaliDocument20 pagesGigantisme Dan AkromegaliNovia Sari Andriati MertosonoNo ratings yet
- Daftar Obat Aman Dan Berbahaya Untuk Ibu Hamil Dan MenyusuiDocument17 pagesDaftar Obat Aman Dan Berbahaya Untuk Ibu Hamil Dan MenyusuiFirda LestariNo ratings yet
- Gir (Glucose Infussion Rate)Document9 pagesGir (Glucose Infussion Rate)arawindahaniastriNo ratings yet
- Fisiologis Lapar Dan KenyangDocument30 pagesFisiologis Lapar Dan Kenyangtamara hannestoNo ratings yet
- Guideline - Training New Trainer ISMKI 2016Document18 pagesGuideline - Training New Trainer ISMKI 2016Dhery Dev WhitterNo ratings yet
- Transplantasi Sumsum TulangDocument32 pagesTransplantasi Sumsum TulangSatria Yosi HernawanNo ratings yet
- Microgest InsertDocument1 pageMicrogest InsertChodhur BhodhurNo ratings yet
- GNA GNC PNC - PPSXDocument31 pagesGNA GNC PNC - PPSXMira AstutiNo ratings yet
- DIS IPD Ceftriaxone KonsulDocument28 pagesDIS IPD Ceftriaxone KonsulTriana MaulidyahNo ratings yet
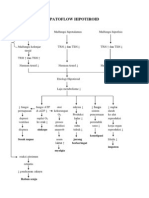
- Patoflow Hipotiroid: Sinkope Konstipasi Sesak Napas Jarang Berkeringat Impoten MyalgiaDocument1 pagePatoflow Hipotiroid: Sinkope Konstipasi Sesak Napas Jarang Berkeringat Impoten MyalgiaDessyana Paulus50% (2)
- Steroid Tapering and Supportive Treatment Guidance V1.0 PDFDocument1 pageSteroid Tapering and Supportive Treatment Guidance V1.0 PDFErwin Novia RachmawatiNo ratings yet
- Approach To The Patient With Postmenopausal Uterine Bleeding - UpToDateDocument18 pagesApproach To The Patient With Postmenopausal Uterine Bleeding - UpToDateCHINDY REPA REPANo ratings yet
- Patofisiologi BatukDocument53 pagesPatofisiologi BatukGd PadmawijayaNo ratings yet
- AST by The CDS Methode PDFDocument88 pagesAST by The CDS Methode PDFari_nuswantoroNo ratings yet
- Timebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisFrom EverandTimebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisRating: 3.5 out of 5 stars3.5/5 (2)
- Hypertension Pocket Guide: Classification of Blood Pressure Levels For People 18 and OlderDocument2 pagesHypertension Pocket Guide: Classification of Blood Pressure Levels For People 18 and OlderMuhammad Mubeen Iqbal PuriNo ratings yet
- Diabetes Kit HCP PocketDocument2 pagesDiabetes Kit HCP PocketjoepinoxNo ratings yet
- Europea GuiaDocument12 pagesEuropea GuiaSindy VergaraNo ratings yet
- HypertensionDocument39 pagesHypertensionMa. Jewon LAGGUINo ratings yet
- Hypertension FamcoDocument42 pagesHypertension FamcoMusleh Al MusalhiNo ratings yet
- JNC-7CE 2hoursDocument91 pagesJNC-7CE 2hourslusiachristinaNo ratings yet
- Hypertension Guidelines 2014: Jason A. Smith, DO Associated Cardiovascular Consultants at Lourdes Cardiology ServicesDocument33 pagesHypertension Guidelines 2014: Jason A. Smith, DO Associated Cardiovascular Consultants at Lourdes Cardiology ServicesRido MaulanaNo ratings yet
- Hypetension FinalDocument32 pagesHypetension FinalGerome ManantanNo ratings yet
- Hypertension - Detection, Diagnosis and Management: ScopeDocument32 pagesHypertension - Detection, Diagnosis and Management: ScopeRudini Thung TungNo ratings yet
- HypertensionDocument44 pagesHypertensionasadcabdi613No ratings yet
- Booklet Bcu Revisi 5Document8 pagesBooklet Bcu Revisi 5irza nasutionNo ratings yet
- Jurnal Yoga Jantung 1Document9 pagesJurnal Yoga Jantung 1Riska ApriliaNo ratings yet
- Booklet InaPrevent 3Document10 pagesBooklet InaPrevent 3Hendra TPNo ratings yet
- Aerobics - Daniels Project FinalDocument12 pagesAerobics - Daniels Project FinalDaniel John D. VelascoNo ratings yet
- 2 Canadian Network For Mood and Anxiety Treatments CANMAT 2016 ClinicalDocument14 pages2 Canadian Network For Mood and Anxiety Treatments CANMAT 2016 ClinicalGino Garavito CriolloNo ratings yet
- HypertensionDocument109 pagesHypertensionmburukalex100% (1)
- Diagnostic Test q1 Grade 11Document8 pagesDiagnostic Test q1 Grade 11Maria benedicta BenitoNo ratings yet
- PN-1150653405 OCHOL Sellsheet DISTDocument4 pagesPN-1150653405 OCHOL Sellsheet DISTMarin MarianNo ratings yet
- Lifestyle Medicine - 2019Document1,473 pagesLifestyle Medicine - 2019Vic_jvpNo ratings yet
- Asian Management of Hypertension: Current Status, Home Blood Pressure, and Specific Concerns in Philippines (A Country Report)Document4 pagesAsian Management of Hypertension: Current Status, Home Blood Pressure, and Specific Concerns in Philippines (A Country Report)DORINNE KINDAONo ratings yet
- Vitamin DDocument38 pagesVitamin DRabailRaajputNo ratings yet
- Aam 5Document65 pagesAam 5iosifpaulNo ratings yet
- Cardiovascular Drug GuidelinesDocument182 pagesCardiovascular Drug GuidelinesSonishNo ratings yet
- Samuel Christian College: Senior High School DepartmentDocument10 pagesSamuel Christian College: Senior High School DepartmentJulie ArcillaNo ratings yet
- Banana Peels As A Bioactive Ingredient and Its Potential Application in The Food IndustryDocument13 pagesBanana Peels As A Bioactive Ingredient and Its Potential Application in The Food IndustryMico BillonesNo ratings yet
- ARTIGO Accelerometer-Derived "Weekend Warrior" Physical ActivityDocument6 pagesARTIGO Accelerometer-Derived "Weekend Warrior" Physical Activitylucas.ec.sousa25No ratings yet
- 2022 - Book - PrecisionMedicineInDiabetes Precision Medicine in DiabeteSDocument340 pages2022 - Book - PrecisionMedicineInDiabetes Precision Medicine in DiabeteSmnqpdewi100% (3)
- Dietary Guidelines Allowances For Americans 2010 USDADocument112 pagesDietary Guidelines Allowances For Americans 2010 USDAkiki_scrabsNo ratings yet
- Medical Equipment Manufacturing Business Plan ExampleDocument34 pagesMedical Equipment Manufacturing Business Plan ExamplePrabha GuptaNo ratings yet
- Lipid GuidelinesDocument78 pagesLipid GuidelinesAryo Damar DjatiNo ratings yet
- Abstrac 2222Document19 pagesAbstrac 2222josephmainam9No ratings yet
- Malaysia Elderly Care Market Report - Industry Trends and Forecast To 2027 - Data Bridge Market ResearchDocument5 pagesMalaysia Elderly Care Market Report - Industry Trends and Forecast To 2027 - Data Bridge Market ResearchTNNo ratings yet
- Anantara Famed BiruDocument53 pagesAnantara Famed BiruMochamadAriWibowoNo ratings yet
- Annotated BibliographyDocument6 pagesAnnotated BibliographyRiley WilliamsNo ratings yet
- Knapen 2014 Disabil Rehabil ExercisetherapyimprovesbothmentalandphysicalhealthinpatientswithmajordepressionDocument7 pagesKnapen 2014 Disabil Rehabil ExercisetherapyimprovesbothmentalandphysicalhealthinpatientswithmajordepressionShweta KateNo ratings yet
- ?overview of Secondary Prevention of Ischemic Stroke - UpToDateDocument40 pages?overview of Secondary Prevention of Ischemic Stroke - UpToDateJorgeNo ratings yet
- Fitness, Sports and Recreation Leadership: Quarter 3 - Module 2Document27 pagesFitness, Sports and Recreation Leadership: Quarter 3 - Module 2Elvin Sajulla Bulalong100% (1)
- Second Quarterly Examination in CaregivingDocument4 pagesSecond Quarterly Examination in CaregivingJasonS.FlavianoNo ratings yet