Download as docx, pdf, or txt
You might also like
- Short Cases in Clinical Exams of Internal Medicine (PDFDrive)Document185 pagesShort Cases in Clinical Exams of Internal Medicine (PDFDrive)Nadhirah ZulkifliNo ratings yet
- Don Goldenberg, Marc Dichter - Unravelling Long COVID-Wiley-Blackwell (2023) PDFDocument259 pagesDon Goldenberg, Marc Dichter - Unravelling Long COVID-Wiley-Blackwell (2023) PDFStefanNo ratings yet
- Expanded Dengue Syndrome: Zukmianty SuaibDocument45 pagesExpanded Dengue Syndrome: Zukmianty SuaibclaraNo ratings yet
- Kraniotomi DekompresiDocument17 pagesKraniotomi DekompresianamselNo ratings yet
- Retractile TestisDocument7 pagesRetractile TestisAhmad Rahmat Ramadhan TantuNo ratings yet
- UHS Dental Examination Form PDFDocument1 pageUHS Dental Examination Form PDFReaStephanieCidNo ratings yet
- Epilepsia EpicongressDocument245 pagesEpilepsia EpicongressВасилий КоптеловNo ratings yet
- Allergen Preparation and Standardization An UpdatDocument5 pagesAllergen Preparation and Standardization An UpdatMa. Femina Lucas100% (1)
- Jurnal GastroenterohepatologiDocument18 pagesJurnal GastroenterohepatologiRarasRachmandiarNo ratings yet
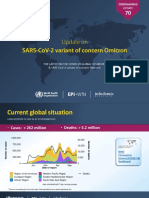
- WHO Update70 OmicronDocument16 pagesWHO Update70 Omicronsuryadev s24No ratings yet
- RozerplastyDocument4 pagesRozerplastyLutfi Aulia RahmanNo ratings yet
- Lapkas Hymen ImperforataDocument27 pagesLapkas Hymen ImperforataKhairida Hafni LbsNo ratings yet
- Onkologi Orthopedi - DR RynDocument27 pagesOnkologi Orthopedi - DR RynyanmedNo ratings yet
- Lapsus IFADocument18 pagesLapsus IFAifaNo ratings yet
- The Effect of Zinc Supplementation in Adult Patients With Acute Diarrhea PDFDocument5 pagesThe Effect of Zinc Supplementation in Adult Patients With Acute Diarrhea PDFAsrori AzharNo ratings yet
- Laporan Kasus Preeklampsia: Disusun Oleh: Dr. Muhammad Fadlan PulunganDocument1 pageLaporan Kasus Preeklampsia: Disusun Oleh: Dr. Muhammad Fadlan PulunganDebora Angelina TobingNo ratings yet
- Aspek Klinis Dan Tatalaksana Gagal Jantung Pada Anak: Tinjauan PustakaDocument11 pagesAspek Klinis Dan Tatalaksana Gagal Jantung Pada Anak: Tinjauan PustakaRafael David MaitimuNo ratings yet
- What Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)Document39 pagesWhat Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)laurentiaNo ratings yet
- Flaps: BY:-Dr. P. Koushik GUIDE: - DR (Brig.) B. B. DograDocument27 pagesFlaps: BY:-Dr. P. Koushik GUIDE: - DR (Brig.) B. B. DograSumit HadgaonkarNo ratings yet
- Trauma KepalaDocument43 pagesTrauma KepalaAray Al-AfiqahNo ratings yet
- Syok Hypovolemik-IH FK UMSU2012Document45 pagesSyok Hypovolemik-IH FK UMSU2012Ratika Ayu PiliangNo ratings yet
- Guildelines For Hiv Testing NacoDocument165 pagesGuildelines For Hiv Testing NacoNagendra Singh BeniwalNo ratings yet
- 11 - 206memahami DispareuniaDocument8 pages11 - 206memahami DispareuniaResti Puteri Apriyuslim0% (1)
- Pembahasan CBT COMBO 3Document802 pagesPembahasan CBT COMBO 3Sari Dewi WiratsihNo ratings yet
- Final 2nd Announcement Konas Perdatin Perdici 2019 - WebsiteDocument67 pagesFinal 2nd Announcement Konas Perdatin Perdici 2019 - WebsiteWirjapratama PutraNo ratings yet
- Jurnal Bedah PlastikDocument3 pagesJurnal Bedah PlastikBilly Shan LastKagerooboroNo ratings yet
- Diabetes Mellitus Pada Anak KuliahDocument51 pagesDiabetes Mellitus Pada Anak KuliahNisha AnggiaNo ratings yet
- Modul Otologi Gangguan Nervus FasialisDocument65 pagesModul Otologi Gangguan Nervus FasialisHERIZALNo ratings yet
- Telaah Kritis JurnalDocument13 pagesTelaah Kritis JurnalfebrinaNo ratings yet
- Skripsi Tanpa Bab Pembahasan PDFDocument67 pagesSkripsi Tanpa Bab Pembahasan PDFaaaaNo ratings yet
- Contoh Soal Residen CardioDocument13 pagesContoh Soal Residen CardioLusyAlwiNo ratings yet
- Tinjauan Pustaka Rehabilitasi Medik Pada Pasien Geriatriulkus DecubitusDocument6 pagesTinjauan Pustaka Rehabilitasi Medik Pada Pasien Geriatriulkus Decubitusrinaldy prayudhiaNo ratings yet
- Crs Abses PeritonsilDocument8 pagesCrs Abses PeritonsilannisaNo ratings yet
- Measles (Campak, Rubeola, Gabak, Kerumut)Document20 pagesMeasles (Campak, Rubeola, Gabak, Kerumut)Michael WijayaNo ratings yet
- Mapping Bedah Urologi Selasa 05/09/2017: Hb/Ht/E/L/TDocument6 pagesMapping Bedah Urologi Selasa 05/09/2017: Hb/Ht/E/L/TfitarayusdaNo ratings yet
- Post Operative DR MarshalDocument20 pagesPost Operative DR MarshalPrastia StratosNo ratings yet
- Pencegahan HivDocument17 pagesPencegahan HivJH ELIS RNo ratings yet
- Jadwal Jaga Ppds April 2017Document3 pagesJadwal Jaga Ppds April 2017josephNo ratings yet
- Case Report - NC TraumaDocument14 pagesCase Report - NC TraumaibunqumairaNo ratings yet
- Pengwas Sitasi VancouverDocument27 pagesPengwas Sitasi VancouverPrameswari ZahraNo ratings yet
- Akreditasi Trisakti PDFDocument1 pageAkreditasi Trisakti PDFMargaret SimmonsNo ratings yet
- Mengenal COVID-19 Revisi Juli 2020Document42 pagesMengenal COVID-19 Revisi Juli 2020Yusufa Fil ArdyNo ratings yet
- PratikPatel - Duodenal AtresiaDocument1 pagePratikPatel - Duodenal AtresiaIkhlasia Amali MahzumNo ratings yet
- Diagnosis and Management of Infantile HemangiomaDocument47 pagesDiagnosis and Management of Infantile HemangiomaSteph FergusonNo ratings yet
- RiNDU2 - First AnnoucementDocument6 pagesRiNDU2 - First AnnoucementMuhammad Hikmah AdhaNo ratings yet
- MorbiliDocument30 pagesMorbiliMjNo ratings yet
- Double Lumen Catheter Dr. Ahmad GhozaliDocument20 pagesDouble Lumen Catheter Dr. Ahmad GhozaliastarimediantoNo ratings yet
- k.42 Tension PneumothoraxDocument20 pagesk.42 Tension Pneumothoraxjamaliganteng88No ratings yet
- Sejawat - Idn - Sistem Saraf Dan MuskuloskeletalDocument85 pagesSejawat - Idn - Sistem Saraf Dan MuskuloskeletalAinaya Miftia Asy'aristaNo ratings yet
- Circular Gips (Casting)Document14 pagesCircular Gips (Casting)frank runtuboiNo ratings yet
- 357-Article Text-1187-1-10-20190419 PDFDocument4 pages357-Article Text-1187-1-10-20190419 PDFwidyaNo ratings yet
- Leprosy: Pathogenesis Updated: ReviewDocument15 pagesLeprosy: Pathogenesis Updated: ReviewagneselimNo ratings yet
- Ketoasidosis DiabetikumDocument13 pagesKetoasidosis DiabetikumAdindapauliaNo ratings yet
- Classification of Head InjuryDocument8 pagesClassification of Head InjuryAkshaya MistryNo ratings yet
- Inotropic and Vasoactive Drugs in Pediatric ICUDocument6 pagesInotropic and Vasoactive Drugs in Pediatric ICUCandy RevolloNo ratings yet
- Anatomi Dan Fisiologi GinjalDocument33 pagesAnatomi Dan Fisiologi GinjalRizha Zhetira100% (1)
- K-5 Pathophysiology of Cyanotic Congenital Heart DefectsDocument15 pagesK-5 Pathophysiology of Cyanotic Congenital Heart DefectsJessica GintingNo ratings yet
- Board Ujian NeuroDocument2 pagesBoard Ujian NeuroTrisna RizkiNo ratings yet
- Kasus Trauma ICDDocument16 pagesKasus Trauma ICDIntan Eklesiana NapitupuluNo ratings yet
- Lapsus Fraktur Neck FemurDocument32 pagesLapsus Fraktur Neck FemurZóélkårnåín PhåntómhívéNo ratings yet
- Erna Case ReportDocument26 pagesErna Case ReportWahidah MusliminNo ratings yet
- Neck Femur FixDocument20 pagesNeck Femur FixRichard WinardiNo ratings yet
- Congenital Talipes Equinovarus FinalDocument28 pagesCongenital Talipes Equinovarus FinalTibin Kavumkal ThomasNo ratings yet
- USG - Hip & Knee-Dr - NarayanDocument92 pagesUSG - Hip & Knee-Dr - NarayancmonmanNo ratings yet
- Lapsus Ortho Word - Id.enDocument17 pagesLapsus Ortho Word - Id.eninhaNo ratings yet
- Httpsclinicalinfo - Hiv.govsitesdefaultfilesguidelinesdocumentsadult - OI - PDF 4 PDFDocument450 pagesHttpsclinicalinfo - Hiv.govsitesdefaultfilesguidelinesdocumentsadult - OI - PDF 4 PDFAna María Ospina ZuletaNo ratings yet
- HK VTC 25-11-2006 Medicinal MushroomsDocument31 pagesHK VTC 25-11-2006 Medicinal MushroomsdeepthikuppuswamyNo ratings yet
- Localisation of Spinal Cord LesionsDocument218 pagesLocalisation of Spinal Cord LesionsGoh Sheen YeeNo ratings yet
- Reading: Hospital StaffDocument9 pagesReading: Hospital StaffPhạm Tuấn AnhNo ratings yet
- 3, Annex-3, Tables-13 A and B, 2018-19Document6 pages3, Annex-3, Tables-13 A and B, 2018-19Sumit BiswasNo ratings yet
- MRCS Essential ListDocument18 pagesMRCS Essential ListMahmoud Selim100% (1)
- Bisoprolol and Hypertension: Effects On Sexual Functioning in MenDocument8 pagesBisoprolol and Hypertension: Effects On Sexual Functioning in MenZahid MahmoodNo ratings yet
- Ultrasound Screening of Soft Tissue Masses in The Trunk and Extremity - A BSG Guide For Ultrasonographers and Primary CareDocument5 pagesUltrasound Screening of Soft Tissue Masses in The Trunk and Extremity - A BSG Guide For Ultrasonographers and Primary CareOmer FarooqNo ratings yet
- Sample DementiaDocument5 pagesSample DementiaAlina LazărNo ratings yet
- Form Strongkids NewDocument2 pagesForm Strongkids NewNovalia Taulanda100% (3)
- Recent Development of Probiotic Bifidobacteria For Treating Human DiseasesDocument17 pagesRecent Development of Probiotic Bifidobacteria For Treating Human DiseasesLinh HoangNo ratings yet
- National Guideline For Ipc in Hse Dental and Orthodontic ServicesDocument125 pagesNational Guideline For Ipc in Hse Dental and Orthodontic ServicesSimona BugaciuNo ratings yet
- 100 Item Obstetrics-Maternal and Child Health Nursing ExaminationDocument50 pages100 Item Obstetrics-Maternal and Child Health Nursing ExaminationMaria Ibarrola100% (1)
- Quasi Experimental Study To Assess The EffectivenessDocument13 pagesQuasi Experimental Study To Assess The EffectivenessInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- SD H.pylori-Ag-Insert 0Document2 pagesSD H.pylori-Ag-Insert 0Labor KaruniaNo ratings yet
- WC 500003409Document12 pagesWC 500003409TowhidulIslamNo ratings yet
- S. Aureus Pneumonia Often Complicates Illness Caused by Influenza VirusesDocument14 pagesS. Aureus Pneumonia Often Complicates Illness Caused by Influenza VirusesRia Dela CruzNo ratings yet
- Vexation and AgitationDocument2 pagesVexation and Agitationpeter911x2134No ratings yet
- Day 5 - APPEC 2021 PDFDocument643 pagesDay 5 - APPEC 2021 PDFGaurieNo ratings yet
- Maternal Child Nursing ExaminationDocument14 pagesMaternal Child Nursing Examinationjames_manuel11187084100% (1)
- Case Analysis Presentation CvaDocument82 pagesCase Analysis Presentation CvaVhince Norben PiscoNo ratings yet
- Cidera TulangDocument9 pagesCidera TulangGifanichan MvpshawolandromedaNo ratings yet
- A Presentation On BurnsDocument23 pagesA Presentation On BurnsMichael AdjeiNo ratings yet
- IMMUNIZATION LecDocument77 pagesIMMUNIZATION LecKavya ReddyNo ratings yet
- Linen and Laundry Pres IntroDocument5 pagesLinen and Laundry Pres IntroO.r. CadzNo ratings yet