
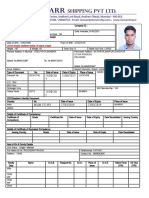
Application Form For Employment
Application Form For Employment
You might also like
- OBDII Codes PDFDocument238 pagesOBDII Codes PDFedhuam50% (6)
- MSC Application FormDocument4 pagesMSC Application FormSneha ChatterjeeNo ratings yet
- Case Analysis ON GlossierDocument8 pagesCase Analysis ON GlossierMadhusmita PattanayakNo ratings yet
- Stowage Plan of Chem TankersDocument21 pagesStowage Plan of Chem TankersKunal Singh100% (1)
- Daily, Monthly and Weekly Tests of GMDSS Equipment On Board ShipsDocument32 pagesDaily, Monthly and Weekly Tests of GMDSS Equipment On Board ShipsKunal Singh100% (1)
- The Pathophysiology of CancerDocument1 pageThe Pathophysiology of Cancermisskitcat100% (11)
- Ship Management Pvt. LTD.: Application Form / Personal Data Update FormDocument5 pagesShip Management Pvt. LTD.: Application Form / Personal Data Update FormViorel StanNo ratings yet
- (Tanker) CVDocument5 pages(Tanker) CVMMS SNo ratings yet
- Am S ApplicationformDocument5 pagesAm S ApplicationformDivay BakshiNo ratings yet
- YUAM Application FormDocument5 pagesYUAM Application FormPrabhu DevaNo ratings yet
- Off. 012 Crew Data Application FormDocument7 pagesOff. 012 Crew Data Application Formsuyashchanne2142No ratings yet
- Seastar Ship Management Private Limited: Application / Personal Data Form For Officer'S & RatingsDocument4 pagesSeastar Ship Management Private Limited: Application / Personal Data Form For Officer'S & RatingsrupalNo ratings yet
- P&W Application FormDocument6 pagesP&W Application FormDeeshalni SivabalanNo ratings yet
- Application For Employment: PhotoDocument6 pagesApplication For Employment: PhotoEzat RahmanNo ratings yet
- Skylark Dasos BrochureDocument12 pagesSkylark Dasos BrochureSuresh CANo ratings yet
- Application Form: RPSL-MUM-167Document3 pagesApplication Form: RPSL-MUM-167Meghanath AdkonkarNo ratings yet
- MBA ApplicationDocument2 pagesMBA ApplicationVarshaNo ratings yet
- C 05 - Seafarer Employment Application Form ABDUL RAHMANDocument4 pagesC 05 - Seafarer Employment Application Form ABDUL RAHMANSoekhaidir SuripnoNo ratings yet
- 02 - Application FormDocument3 pages02 - Application FormMohamed El SheikhNo ratings yet
- WSMKR Application Blank NewDocument4 pagesWSMKR Application Blank Newevander.lazarteNo ratings yet
- Msccs - Application FormDocument4 pagesMsccs - Application FormanitttaNo ratings yet
- 1.1 A CNCO SPSM Application Form - Crew OCT 2020 VersionDocument11 pages1.1 A CNCO SPSM Application Form - Crew OCT 2020 VersionCharlemaigne Josef DolorielNo ratings yet
- 1216 - CareerPDF2 - Appendix-I - Medical OfficerDocument3 pages1216 - CareerPDF2 - Appendix-I - Medical OfficermvprakashNo ratings yet
- Application Form Rev 4Document4 pagesApplication Form Rev 4MARK ANTHONY TIONGSONNo ratings yet
- OIS Application FormDocument6 pagesOIS Application FormShanidu MalshanNo ratings yet
- SPSM ASSM Application FormDocument10 pagesSPSM ASSM Application FormCharlemaigne Josef Cuartero DolorielNo ratings yet
- 1.officers Application Form RiomarrDocument5 pages1.officers Application Form RiomarrÁřvíňď PřášáďNo ratings yet
- Notification DMHO West Godavari Staff Nurse Lab Technician Other PostsDocument3 pagesNotification DMHO West Godavari Staff Nurse Lab Technician Other PostsrajaNo ratings yet
- UPDATED CRW13 - Application Form 6.1Document2 pagesUPDATED CRW13 - Application Form 6.1jeffNo ratings yet
- Draftsperson Registration Application Form PDFDocument13 pagesDraftsperson Registration Application Form PDFKaterina KaradikNo ratings yet
- NHSRCL-APPLICATION-FORM-1539150837-Application FormDocument5 pagesNHSRCL-APPLICATION-FORM-1539150837-Application FormGaurav SinghNo ratings yet
- Appln Format Cso 01102010Document3 pagesAppln Format Cso 01102010asherraniNo ratings yet
- Application Form MSDocument3 pagesApplication Form MSravi12b2006No ratings yet
- PF012.3 Application and Induction PackDocument14 pagesPF012.3 Application and Induction PackJide SeyiNo ratings yet
- Ussl001en - PM0302 - CV Ussl - EngDocument4 pagesUssl001en - PM0302 - CV Ussl - Engsifat.8712.khanNo ratings yet
- 2021 SSPL Application Form - Crew OCT 2021 VersionDocument4 pages2021 SSPL Application Form - Crew OCT 2021 VersionjeffNo ratings yet
- Application Civil 01092010Document3 pagesApplication Civil 01092010dhanishNo ratings yet
- DTD.X: Sri Venkateswara Institute of Medical Sciences, Tirupati Notification Roc - No.C1/21/Cfar/Svims/18, Dtd.09.02.19Document2 pagesDTD.X: Sri Venkateswara Institute of Medical Sciences, Tirupati Notification Roc - No.C1/21/Cfar/Svims/18, Dtd.09.02.19Ramanje SirNo ratings yet
- CMA Ships Application Form Crewform 01aDocument9 pagesCMA Ships Application Form Crewform 01aNicu ScutaruNo ratings yet
- CMA Ships Application Form Crewform 01aDocument9 pagesCMA Ships Application Form Crewform 01aCfyt50% (2)
- Personal Particulars FormatDocument2 pagesPersonal Particulars Formatchandan kumar giriNo ratings yet
- Suntech Ship MGMT Employment FormDocument6 pagesSuntech Ship MGMT Employment FormAvinash Singh100% (1)
- CCF 015 Sea Staff Application FormDocument1 pageCCF 015 Sea Staff Application Formtharindu hasarangaNo ratings yet
- Aei-Fpd 01-New - Application FormDocument1 pageAei-Fpd 01-New - Application FormTarique MarchentNo ratings yet
- APPL030709Document1 pageAPPL030709svjnair100% (2)
- Application/Personal Data Form - No - : - Last Salary (USD) Propose VesselDocument1 pageApplication/Personal Data Form - No - : - Last Salary (USD) Propose VesselКирилл БуровNo ratings yet
- MSC ApplicationDocument4 pagesMSC ApplicationRathinavel001No ratings yet
- Brukaan Officers Application FormDocument5 pagesBrukaan Officers Application Formbaba maachoNo ratings yet
- Application Form: Chinar Shipping & Trading Co. Pvt. LTDDocument3 pagesApplication Form: Chinar Shipping & Trading Co. Pvt. LTDcaptdadwalNo ratings yet
- Rigel Marine Services Biodata / Pre Joining Form - Officers: Personal DataDocument4 pagesRigel Marine Services Biodata / Pre Joining Form - Officers: Personal DataSatyabrat GaanNo ratings yet
- ITF - SIWES Report Sheet - 1584379696Document2 pagesITF - SIWES Report Sheet - 1584379696Animonga HajimeNo ratings yet
- Application Form Rev 0320Document9 pagesApplication Form Rev 0320Deepak PandeyNo ratings yet
- Application For Rectt AMD1 2011Document4 pagesApplication For Rectt AMD1 2011Amod KumarNo ratings yet
- Application Form Winter 2012Document2 pagesApplication Form Winter 2012shehzaib tariqNo ratings yet
- Offline Applicatiion Format-PuducherryDocument5 pagesOffline Applicatiion Format-Puducherrykumaresanr812No ratings yet
- Polembros Shipping Limited Sea Staff Application and Interview FormDocument2 pagesPolembros Shipping Limited Sea Staff Application and Interview FormBilly NasaiosNo ratings yet
- Hiring Application FormDocument6 pagesHiring Application FormAnonymous QHfIVes9r100% (1)
- Revised JSC Employment Form 2021 UPDATED 29.03.2022Document5 pagesRevised JSC Employment Form 2021 UPDATED 29.03.2022tonysisseyNo ratings yet
- Part A. Application Form: Seaman S Application Prior Joining THE Vessel A ND Assessment ProfileDocument4 pagesPart A. Application Form: Seaman S Application Prior Joining THE Vessel A ND Assessment ProfileCap Karim ElSherbiniNo ratings yet
- Seafarer ApplicationDocument5 pagesSeafarer ApplicationAvais ManiyarNo ratings yet
- RP03 Seafarers Recruitment Proposal FormDocument4 pagesRP03 Seafarers Recruitment Proposal FormPETER BROWMNo ratings yet
- Job Application FormDocument4 pagesJob Application FormDinu EdirisingheNo ratings yet
- CEPTAM-03 Application FormDocument2 pagesCEPTAM-03 Application Formshenoy_ramakrishnaNo ratings yet
- Standard Application Form 6 Pager FATCA Change 31052016Document6 pagesStandard Application Form 6 Pager FATCA Change 31052016आज़ाद पटेलNo ratings yet
- Framo Hydraulic Cargo Pumping System On ShipsDocument3 pagesFramo Hydraulic Cargo Pumping System On ShipsKunal SinghNo ratings yet
- Submerged Pump SysDocument2 pagesSubmerged Pump SysKunal SinghNo ratings yet
- ACRYLONITRILE Characteristics & Handling MethodsDocument3 pagesACRYLONITRILE Characteristics & Handling MethodsKunal SinghNo ratings yet
- Survival Craft VHF 2Document7 pagesSurvival Craft VHF 2Kunal SinghNo ratings yet
- Types of PumpsDocument3 pagesTypes of PumpsKunal SinghNo ratings yet
- Safety Questions & AnswersDocument18 pagesSafety Questions & AnswersKunal Singh100% (2)
- ECDISDocument28 pagesECDISKunal SinghNo ratings yet
- Pilot Transfer Arrangements PDFDocument7 pagesPilot Transfer Arrangements PDFKunal SinghNo ratings yet
- Fire Test ProcedureDocument9 pagesFire Test ProcedureKunal SinghNo ratings yet
- Fair Treatment of SeafarersDocument3 pagesFair Treatment of SeafarersKunal SinghNo ratings yet
- A Complete Guide of Loading TDI Onboard A Chemical TankerDocument19 pagesA Complete Guide of Loading TDI Onboard A Chemical TankerKunal Singh100% (1)
- Annual Summary of Notices To Mariners What Is NP 247Document2 pagesAnnual Summary of Notices To Mariners What Is NP 247Kunal SinghNo ratings yet
- Annual Summary of Notices To Mariners What Is NP247Document2 pagesAnnual Summary of Notices To Mariners What Is NP247Kunal SinghNo ratings yet
- Why Captain's Cabin Is Always On Starboard SideDocument2 pagesWhy Captain's Cabin Is Always On Starboard SideKunal SinghNo ratings yet
- What Is Abort Point and How You Can Use It For Safe NavigationDocument16 pagesWhat Is Abort Point and How You Can Use It For Safe NavigationKunal Singh100% (1)
- Annual Summary of Notices To Mariners What Is NP247Document2 pagesAnnual Summary of Notices To Mariners What Is NP247Kunal SinghNo ratings yet
- Understanding IMO Conventions, Resolutions and CircularsDocument15 pagesUnderstanding IMO Conventions, Resolutions and CircularsKunal Singh100% (2)
- Where Does NBDP Fit in GMDSS and How To Use ItDocument14 pagesWhere Does NBDP Fit in GMDSS and How To Use ItKunal SinghNo ratings yet
- Ecdis Chart CorrDocument24 pagesEcdis Chart CorrKunal Singh100% (2)
- GMDSS Batteries Tests and Checks Mariners Must KnowDocument9 pagesGMDSS Batteries Tests and Checks Mariners Must KnowKunal Singh100% (2)
- Katalog Techniczny ENG PDFDocument136 pagesKatalog Techniczny ENG PDFJoseph Cloyd L. LamberteNo ratings yet
- Mtic NotesDocument50 pagesMtic NotesAnshita GargNo ratings yet
- Financial Planning and BudgetingDocument45 pagesFinancial Planning and BudgetingRafael BensigNo ratings yet
- Cisco 3Document396 pagesCisco 3Vihaga JayalathNo ratings yet
- Anno 2070Document16 pagesAnno 207012345zolyNo ratings yet
- Software Defined RadioDocument17 pagesSoftware Defined RadioJyoti BaliNo ratings yet
- NTA PM (Approved As Final 11-7-11)Document9 pagesNTA PM (Approved As Final 11-7-11)charlene cleo eibenNo ratings yet
- Business Studies HSC Exam 2010Document18 pagesBusiness Studies HSC Exam 2010MikeNo ratings yet
- PowerFlex Rack Administration - Instructor GuideDocument241 pagesPowerFlex Rack Administration - Instructor GuideGreivin ArguedasNo ratings yet
- Merivaara Futura Plus 8381 Junior Manual ServiceDocument40 pagesMerivaara Futura Plus 8381 Junior Manual ServiceDanniel SchaafNo ratings yet
- MKT 201 - Lecture 2 & 3Document73 pagesMKT 201 - Lecture 2 & 3Duval PearsonNo ratings yet
- Syllabus Fire FightingDocument112 pagesSyllabus Fire FightingMuhammad MukhtarNo ratings yet
- Verbal Section Reading CompDocument35 pagesVerbal Section Reading CompBasharat AliNo ratings yet
- SQL WindowsDocument424 pagesSQL WindowsjNo ratings yet
- Saiteja T.S ReportDocument4 pagesSaiteja T.S ReportSaiNo ratings yet
- 08 Chapter 2Document22 pages08 Chapter 2venuNo ratings yet
- Cambridge Food HygieneDocument22 pagesCambridge Food Hygieneapi-350003268No ratings yet
- Mechanical Engineering Technology 241A0 Info Sheet WebDocument2 pagesMechanical Engineering Technology 241A0 Info Sheet WebtomaNo ratings yet
- Contractor All Risk (CAR) PolicyDocument22 pagesContractor All Risk (CAR) PolicySew BigNo ratings yet
- TLE Computer Systems Servicing 10 Installing and Configuring Computer Systems (ICCS) Quarter 2 - Week 1 ModuleDocument10 pagesTLE Computer Systems Servicing 10 Installing and Configuring Computer Systems (ICCS) Quarter 2 - Week 1 ModulePauljam OnamorNo ratings yet
- Science Has Made Life Better But Not Easier.' Discuss.Document2 pagesScience Has Made Life Better But Not Easier.' Discuss.Yvette LimNo ratings yet
- Self Learning PPT1 Application LayerDocument34 pagesSelf Learning PPT1 Application LayerHarsh SinghalNo ratings yet
- Jimenez Vizconde Lozcano V VeranoDocument2 pagesJimenez Vizconde Lozcano V VeranoEscanorNo ratings yet
- Banking Laws Cases Diligence Required From BanksDocument4 pagesBanking Laws Cases Diligence Required From Bankslalyn100% (1)
- Ojt Questions AnswersDocument1 pageOjt Questions Answersapi-127186411No ratings yet
- Equipo PanasonicDocument42 pagesEquipo PanasonicCarlos JaramilloNo ratings yet
- SSP 425 EcoFuel Natural Gas Drive With 1.4L 110 KW TSI EngineDocument28 pagesSSP 425 EcoFuel Natural Gas Drive With 1.4L 110 KW TSI EnginefferdinandNo ratings yet












































































































Download as doc, pdf, or txt
You might also like
- OBDII Codes PDFDocument238 pagesOBDII Codes PDFedhuam50% (6)
- MSC Application FormDocument4 pagesMSC Application FormSneha ChatterjeeNo ratings yet
- Case Analysis ON GlossierDocument8 pagesCase Analysis ON GlossierMadhusmita PattanayakNo ratings yet
- Stowage Plan of Chem TankersDocument21 pagesStowage Plan of Chem TankersKunal Singh100% (1)
- Daily, Monthly and Weekly Tests of GMDSS Equipment On Board ShipsDocument32 pagesDaily, Monthly and Weekly Tests of GMDSS Equipment On Board ShipsKunal Singh100% (1)
- The Pathophysiology of CancerDocument1 pageThe Pathophysiology of Cancermisskitcat100% (11)
- Ship Management Pvt. LTD.: Application Form / Personal Data Update FormDocument5 pagesShip Management Pvt. LTD.: Application Form / Personal Data Update FormViorel StanNo ratings yet
- (Tanker) CVDocument5 pages(Tanker) CVMMS SNo ratings yet
- Am S ApplicationformDocument5 pagesAm S ApplicationformDivay BakshiNo ratings yet
- YUAM Application FormDocument5 pagesYUAM Application FormPrabhu DevaNo ratings yet
- Off. 012 Crew Data Application FormDocument7 pagesOff. 012 Crew Data Application Formsuyashchanne2142No ratings yet
- Seastar Ship Management Private Limited: Application / Personal Data Form For Officer'S & RatingsDocument4 pagesSeastar Ship Management Private Limited: Application / Personal Data Form For Officer'S & RatingsrupalNo ratings yet
- P&W Application FormDocument6 pagesP&W Application FormDeeshalni SivabalanNo ratings yet
- Application For Employment: PhotoDocument6 pagesApplication For Employment: PhotoEzat RahmanNo ratings yet
- Skylark Dasos BrochureDocument12 pagesSkylark Dasos BrochureSuresh CANo ratings yet
- Application Form: RPSL-MUM-167Document3 pagesApplication Form: RPSL-MUM-167Meghanath AdkonkarNo ratings yet
- MBA ApplicationDocument2 pagesMBA ApplicationVarshaNo ratings yet
- C 05 - Seafarer Employment Application Form ABDUL RAHMANDocument4 pagesC 05 - Seafarer Employment Application Form ABDUL RAHMANSoekhaidir SuripnoNo ratings yet
- 02 - Application FormDocument3 pages02 - Application FormMohamed El SheikhNo ratings yet
- WSMKR Application Blank NewDocument4 pagesWSMKR Application Blank Newevander.lazarteNo ratings yet
- Msccs - Application FormDocument4 pagesMsccs - Application FormanitttaNo ratings yet
- 1.1 A CNCO SPSM Application Form - Crew OCT 2020 VersionDocument11 pages1.1 A CNCO SPSM Application Form - Crew OCT 2020 VersionCharlemaigne Josef DolorielNo ratings yet
- 1216 - CareerPDF2 - Appendix-I - Medical OfficerDocument3 pages1216 - CareerPDF2 - Appendix-I - Medical OfficermvprakashNo ratings yet
- Application Form Rev 4Document4 pagesApplication Form Rev 4MARK ANTHONY TIONGSONNo ratings yet
- OIS Application FormDocument6 pagesOIS Application FormShanidu MalshanNo ratings yet
- SPSM ASSM Application FormDocument10 pagesSPSM ASSM Application FormCharlemaigne Josef Cuartero DolorielNo ratings yet
- 1.officers Application Form RiomarrDocument5 pages1.officers Application Form RiomarrÁřvíňď PřášáďNo ratings yet
- Notification DMHO West Godavari Staff Nurse Lab Technician Other PostsDocument3 pagesNotification DMHO West Godavari Staff Nurse Lab Technician Other PostsrajaNo ratings yet
- UPDATED CRW13 - Application Form 6.1Document2 pagesUPDATED CRW13 - Application Form 6.1jeffNo ratings yet
- Draftsperson Registration Application Form PDFDocument13 pagesDraftsperson Registration Application Form PDFKaterina KaradikNo ratings yet
- NHSRCL-APPLICATION-FORM-1539150837-Application FormDocument5 pagesNHSRCL-APPLICATION-FORM-1539150837-Application FormGaurav SinghNo ratings yet
- Appln Format Cso 01102010Document3 pagesAppln Format Cso 01102010asherraniNo ratings yet
- Application Form MSDocument3 pagesApplication Form MSravi12b2006No ratings yet
- PF012.3 Application and Induction PackDocument14 pagesPF012.3 Application and Induction PackJide SeyiNo ratings yet
- Ussl001en - PM0302 - CV Ussl - EngDocument4 pagesUssl001en - PM0302 - CV Ussl - Engsifat.8712.khanNo ratings yet
- 2021 SSPL Application Form - Crew OCT 2021 VersionDocument4 pages2021 SSPL Application Form - Crew OCT 2021 VersionjeffNo ratings yet
- Application Civil 01092010Document3 pagesApplication Civil 01092010dhanishNo ratings yet
- DTD.X: Sri Venkateswara Institute of Medical Sciences, Tirupati Notification Roc - No.C1/21/Cfar/Svims/18, Dtd.09.02.19Document2 pagesDTD.X: Sri Venkateswara Institute of Medical Sciences, Tirupati Notification Roc - No.C1/21/Cfar/Svims/18, Dtd.09.02.19Ramanje SirNo ratings yet
- CMA Ships Application Form Crewform 01aDocument9 pagesCMA Ships Application Form Crewform 01aNicu ScutaruNo ratings yet
- CMA Ships Application Form Crewform 01aDocument9 pagesCMA Ships Application Form Crewform 01aCfyt50% (2)
- Personal Particulars FormatDocument2 pagesPersonal Particulars Formatchandan kumar giriNo ratings yet
- Suntech Ship MGMT Employment FormDocument6 pagesSuntech Ship MGMT Employment FormAvinash Singh100% (1)
- CCF 015 Sea Staff Application FormDocument1 pageCCF 015 Sea Staff Application Formtharindu hasarangaNo ratings yet
- Aei-Fpd 01-New - Application FormDocument1 pageAei-Fpd 01-New - Application FormTarique MarchentNo ratings yet
- APPL030709Document1 pageAPPL030709svjnair100% (2)
- Application/Personal Data Form - No - : - Last Salary (USD) Propose VesselDocument1 pageApplication/Personal Data Form - No - : - Last Salary (USD) Propose VesselКирилл БуровNo ratings yet
- MSC ApplicationDocument4 pagesMSC ApplicationRathinavel001No ratings yet
- Brukaan Officers Application FormDocument5 pagesBrukaan Officers Application Formbaba maachoNo ratings yet
- Application Form: Chinar Shipping & Trading Co. Pvt. LTDDocument3 pagesApplication Form: Chinar Shipping & Trading Co. Pvt. LTDcaptdadwalNo ratings yet
- Rigel Marine Services Biodata / Pre Joining Form - Officers: Personal DataDocument4 pagesRigel Marine Services Biodata / Pre Joining Form - Officers: Personal DataSatyabrat GaanNo ratings yet
- ITF - SIWES Report Sheet - 1584379696Document2 pagesITF - SIWES Report Sheet - 1584379696Animonga HajimeNo ratings yet
- Application Form Rev 0320Document9 pagesApplication Form Rev 0320Deepak PandeyNo ratings yet
- Application For Rectt AMD1 2011Document4 pagesApplication For Rectt AMD1 2011Amod KumarNo ratings yet
- Application Form Winter 2012Document2 pagesApplication Form Winter 2012shehzaib tariqNo ratings yet
- Offline Applicatiion Format-PuducherryDocument5 pagesOffline Applicatiion Format-Puducherrykumaresanr812No ratings yet
- Polembros Shipping Limited Sea Staff Application and Interview FormDocument2 pagesPolembros Shipping Limited Sea Staff Application and Interview FormBilly NasaiosNo ratings yet
- Hiring Application FormDocument6 pagesHiring Application FormAnonymous QHfIVes9r100% (1)
- Revised JSC Employment Form 2021 UPDATED 29.03.2022Document5 pagesRevised JSC Employment Form 2021 UPDATED 29.03.2022tonysisseyNo ratings yet
- Part A. Application Form: Seaman S Application Prior Joining THE Vessel A ND Assessment ProfileDocument4 pagesPart A. Application Form: Seaman S Application Prior Joining THE Vessel A ND Assessment ProfileCap Karim ElSherbiniNo ratings yet
- Seafarer ApplicationDocument5 pagesSeafarer ApplicationAvais ManiyarNo ratings yet
- RP03 Seafarers Recruitment Proposal FormDocument4 pagesRP03 Seafarers Recruitment Proposal FormPETER BROWMNo ratings yet
- Job Application FormDocument4 pagesJob Application FormDinu EdirisingheNo ratings yet
- CEPTAM-03 Application FormDocument2 pagesCEPTAM-03 Application Formshenoy_ramakrishnaNo ratings yet
- Standard Application Form 6 Pager FATCA Change 31052016Document6 pagesStandard Application Form 6 Pager FATCA Change 31052016आज़ाद पटेलNo ratings yet
- Framo Hydraulic Cargo Pumping System On ShipsDocument3 pagesFramo Hydraulic Cargo Pumping System On ShipsKunal SinghNo ratings yet
- Submerged Pump SysDocument2 pagesSubmerged Pump SysKunal SinghNo ratings yet
- ACRYLONITRILE Characteristics & Handling MethodsDocument3 pagesACRYLONITRILE Characteristics & Handling MethodsKunal SinghNo ratings yet
- Survival Craft VHF 2Document7 pagesSurvival Craft VHF 2Kunal SinghNo ratings yet
- Types of PumpsDocument3 pagesTypes of PumpsKunal SinghNo ratings yet
- Safety Questions & AnswersDocument18 pagesSafety Questions & AnswersKunal Singh100% (2)
- ECDISDocument28 pagesECDISKunal SinghNo ratings yet
- Pilot Transfer Arrangements PDFDocument7 pagesPilot Transfer Arrangements PDFKunal SinghNo ratings yet
- Fire Test ProcedureDocument9 pagesFire Test ProcedureKunal SinghNo ratings yet
- Fair Treatment of SeafarersDocument3 pagesFair Treatment of SeafarersKunal SinghNo ratings yet
- A Complete Guide of Loading TDI Onboard A Chemical TankerDocument19 pagesA Complete Guide of Loading TDI Onboard A Chemical TankerKunal Singh100% (1)
- Annual Summary of Notices To Mariners What Is NP 247Document2 pagesAnnual Summary of Notices To Mariners What Is NP 247Kunal SinghNo ratings yet
- Annual Summary of Notices To Mariners What Is NP247Document2 pagesAnnual Summary of Notices To Mariners What Is NP247Kunal SinghNo ratings yet
- Why Captain's Cabin Is Always On Starboard SideDocument2 pagesWhy Captain's Cabin Is Always On Starboard SideKunal SinghNo ratings yet
- What Is Abort Point and How You Can Use It For Safe NavigationDocument16 pagesWhat Is Abort Point and How You Can Use It For Safe NavigationKunal Singh100% (1)
- Annual Summary of Notices To Mariners What Is NP247Document2 pagesAnnual Summary of Notices To Mariners What Is NP247Kunal SinghNo ratings yet
- Understanding IMO Conventions, Resolutions and CircularsDocument15 pagesUnderstanding IMO Conventions, Resolutions and CircularsKunal Singh100% (2)
- Where Does NBDP Fit in GMDSS and How To Use ItDocument14 pagesWhere Does NBDP Fit in GMDSS and How To Use ItKunal SinghNo ratings yet
- Ecdis Chart CorrDocument24 pagesEcdis Chart CorrKunal Singh100% (2)
- GMDSS Batteries Tests and Checks Mariners Must KnowDocument9 pagesGMDSS Batteries Tests and Checks Mariners Must KnowKunal Singh100% (2)
- Katalog Techniczny ENG PDFDocument136 pagesKatalog Techniczny ENG PDFJoseph Cloyd L. LamberteNo ratings yet
- Mtic NotesDocument50 pagesMtic NotesAnshita GargNo ratings yet
- Financial Planning and BudgetingDocument45 pagesFinancial Planning and BudgetingRafael BensigNo ratings yet
- Cisco 3Document396 pagesCisco 3Vihaga JayalathNo ratings yet
- Anno 2070Document16 pagesAnno 207012345zolyNo ratings yet
- Software Defined RadioDocument17 pagesSoftware Defined RadioJyoti BaliNo ratings yet
- NTA PM (Approved As Final 11-7-11)Document9 pagesNTA PM (Approved As Final 11-7-11)charlene cleo eibenNo ratings yet
- Business Studies HSC Exam 2010Document18 pagesBusiness Studies HSC Exam 2010MikeNo ratings yet
- PowerFlex Rack Administration - Instructor GuideDocument241 pagesPowerFlex Rack Administration - Instructor GuideGreivin ArguedasNo ratings yet
- Merivaara Futura Plus 8381 Junior Manual ServiceDocument40 pagesMerivaara Futura Plus 8381 Junior Manual ServiceDanniel SchaafNo ratings yet
- MKT 201 - Lecture 2 & 3Document73 pagesMKT 201 - Lecture 2 & 3Duval PearsonNo ratings yet
- Syllabus Fire FightingDocument112 pagesSyllabus Fire FightingMuhammad MukhtarNo ratings yet
- Verbal Section Reading CompDocument35 pagesVerbal Section Reading CompBasharat AliNo ratings yet
- SQL WindowsDocument424 pagesSQL WindowsjNo ratings yet
- Saiteja T.S ReportDocument4 pagesSaiteja T.S ReportSaiNo ratings yet
- 08 Chapter 2Document22 pages08 Chapter 2venuNo ratings yet
- Cambridge Food HygieneDocument22 pagesCambridge Food Hygieneapi-350003268No ratings yet
- Mechanical Engineering Technology 241A0 Info Sheet WebDocument2 pagesMechanical Engineering Technology 241A0 Info Sheet WebtomaNo ratings yet
- Contractor All Risk (CAR) PolicyDocument22 pagesContractor All Risk (CAR) PolicySew BigNo ratings yet
- TLE Computer Systems Servicing 10 Installing and Configuring Computer Systems (ICCS) Quarter 2 - Week 1 ModuleDocument10 pagesTLE Computer Systems Servicing 10 Installing and Configuring Computer Systems (ICCS) Quarter 2 - Week 1 ModulePauljam OnamorNo ratings yet
- Science Has Made Life Better But Not Easier.' Discuss.Document2 pagesScience Has Made Life Better But Not Easier.' Discuss.Yvette LimNo ratings yet
- Self Learning PPT1 Application LayerDocument34 pagesSelf Learning PPT1 Application LayerHarsh SinghalNo ratings yet
- Jimenez Vizconde Lozcano V VeranoDocument2 pagesJimenez Vizconde Lozcano V VeranoEscanorNo ratings yet
- Banking Laws Cases Diligence Required From BanksDocument4 pagesBanking Laws Cases Diligence Required From Bankslalyn100% (1)
- Ojt Questions AnswersDocument1 pageOjt Questions Answersapi-127186411No ratings yet
- Equipo PanasonicDocument42 pagesEquipo PanasonicCarlos JaramilloNo ratings yet
- SSP 425 EcoFuel Natural Gas Drive With 1.4L 110 KW TSI EngineDocument28 pagesSSP 425 EcoFuel Natural Gas Drive With 1.4L 110 KW TSI EnginefferdinandNo ratings yet