Download as pdf or txt
You might also like
- Motion For Summary JudgementDocument16 pagesMotion For Summary Judgementapi-374578652100% (3)
- 11-How To Make Any Twit Fall in Love With YouDocument13 pages11-How To Make Any Twit Fall in Love With YouAlex Sherlock-Stephonopoliss Holmes100% (1)
- A NEW Lightweight Symmetric Searchable Encryption Scheme For String IdentificationDocument9 pagesA NEW Lightweight Symmetric Searchable Encryption Scheme For String IdentificationMurali KrihnaNo ratings yet
- Guitar Lesson PlansDocument13 pagesGuitar Lesson PlansjamieholroydNo ratings yet
- Odontoma Vaka RaporuDocument4 pagesOdontoma Vaka RaporutasbetulNo ratings yet
- Amhsr 3 285Document3 pagesAmhsr 3 285Dwi Dayanti AgustinaNo ratings yet
- 15l8m04Document4 pages15l8m04chd9r5hr5kNo ratings yet
- Compound Odontoma - A Case ReportDocument10 pagesCompound Odontoma - A Case ReportRyan BachoNo ratings yet
- Compound Odontome A Case ReportDocument4 pagesCompound Odontome A Case ReportMariane SantosNo ratings yet
- JDMT - Volume 8 - Issue 3 - Pages 149-152Document4 pagesJDMT - Volume 8 - Issue 3 - Pages 149-152Alan PermanaNo ratings yet
- Odontomas: Pediatric Case Report and Review of The LiteratureDocument7 pagesOdontomas: Pediatric Case Report and Review of The LiteratureAlan PermanaNo ratings yet
- Compound Odontoma Associated With Impacted Maxillary Anterior Teeth A Case ReportDocument4 pagesCompound Odontoma Associated With Impacted Maxillary Anterior Teeth A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jurnal Asli JR Radiologi - Unusual Giant Complex Odontoma A Case ReportDocument4 pagesJurnal Asli JR Radiologi - Unusual Giant Complex Odontoma A Case ReportAliaNo ratings yet
- Odontoma Compound 1Document4 pagesOdontoma Compound 1ashariNo ratings yet
- 30 Case ReportDocument12 pages30 Case ReportkikiagrivitaNo ratings yet
- Compoun MolarDocument4 pagesCompoun MolarGhea AlmadeaNo ratings yet
- Compound Odontoma in Anterior Mandible-A Case Report: Eswara UMADocument4 pagesCompound Odontoma in Anterior Mandible-A Case Report: Eswara UMAMariane SantosNo ratings yet
- Odontoma: Case Series & Report of Cases Complicated by Infection and Multiple DenticlesDocument6 pagesOdontoma: Case Series & Report of Cases Complicated by Infection and Multiple DenticlesRamdaniar N. DianaNo ratings yet
- tmpB15C TMPDocument5 pagestmpB15C TMPFrontiersNo ratings yet
- BCR 2013 200316Document4 pagesBCR 2013 200316ay lmaoNo ratings yet
- Benign and MalignantDocument16 pagesBenign and MalignantRSU DUTA MULYANo ratings yet
- Clinical Case Reports - 2022 - Khalifa - Compound Complex Odontoma A Rare Case ReportDocument4 pagesClinical Case Reports - 2022 - Khalifa - Compound Complex Odontoma A Rare Case ReportAlbert OliveraNo ratings yet
- Dentigerous Cyst Associated With Transmigrated Mandibular Canine - A Case ReportDocument5 pagesDentigerous Cyst Associated With Transmigrated Mandibular Canine - A Case ReportIJAR JOURNALNo ratings yet
- Compound Odontoma PDFDocument6 pagesCompound Odontoma PDFNarendra ChaudhariNo ratings yet
- Oral Path Case Study PaperDocument4 pagesOral Path Case Study PaperSukirti MisraNo ratings yet
- Odontogenic FibromaDocument5 pagesOdontogenic FibromaGowthamChandraSrungavarapuNo ratings yet
- Crid2022 5981020Document10 pagesCrid2022 5981020lily oktarizaNo ratings yet
- Complex Odontome A Case ReportDocument3 pagesComplex Odontome A Case ReportJustforkiddslaserdental ChNo ratings yet
- Quiste DentigeroDocument5 pagesQuiste DentigeroAlicia Ajahuana PariNo ratings yet
- JOralMaxillofacRadiol3270-5211945 142839Document6 pagesJOralMaxillofacRadiol3270-5211945 142839Ankit SahaNo ratings yet
- Dentigerous Cyst With Recurrent Maxillary Sinusitis A Case Report With Literature ReviewDocument4 pagesDentigerous Cyst With Recurrent Maxillary Sinusitis A Case Report With Literature ReviewAnne LydellNo ratings yet
- Ameloblastic Fibro-Dentinoma of Mandible: A Case ReportDocument3 pagesAmeloblastic Fibro-Dentinoma of Mandible: A Case ReportBrutusRexNo ratings yet
- Dentigerous Cyst Associated With Multiple Complex Composite OdontomasDocument3 pagesDentigerous Cyst Associated With Multiple Complex Composite OdontomasayuandraniNo ratings yet
- Saudi Journal of Pathology and Microbiology (SJPM) : Case ReportDocument3 pagesSaudi Journal of Pathology and Microbiology (SJPM) : Case ReportSuman ChaturvediNo ratings yet
- Minnimally Invasive Surgical Management of Compound Odontoma at Floor Maxillary Sinus Associated With Impacted Caninus: A Case ReportDocument5 pagesMinnimally Invasive Surgical Management of Compound Odontoma at Floor Maxillary Sinus Associated With Impacted Caninus: A Case ReportRussi AshariNo ratings yet
- Periapical Cemento-Osseous Dysplasia Clinicopathological FeaturesDocument4 pagesPeriapical Cemento-Osseous Dysplasia Clinicopathological FeaturesCindyNo ratings yet
- Figure 1 - Clinical Photograph Showing Erupted Odontoma: StructuresDocument4 pagesFigure 1 - Clinical Photograph Showing Erupted Odontoma: Structuresmohamed ibrahimNo ratings yet
- Partial PulpotomyDocument5 pagesPartial PulpotomyLeena Losheene VijayakumarNo ratings yet
- Dafpus 1Document8 pagesDafpus 1Winda WidhyastutiNo ratings yet
- Adenomatoid Odontogenic Tumor, An Uncommon TumorDocument3 pagesAdenomatoid Odontogenic Tumor, An Uncommon TumorHarshavardhan ReddyNo ratings yet
- Compound Odontoma Associated With Impacted Teeth: A Case ReportDocument4 pagesCompound Odontoma Associated With Impacted Teeth: A Case ReportayuandraniNo ratings yet
- GulusinDocument5 pagesGulusinEkta KhobragadeNo ratings yet
- Differential Diagnosis of Periapical Radiolucencies and RadiopacitiesDocument27 pagesDifferential Diagnosis of Periapical Radiolucencies and RadiopacitiesDerya İçözNo ratings yet
- Osseous Choristoma of The Periodontium: Case ReportDocument3 pagesOsseous Choristoma of The Periodontium: Case ReportAndykaYayanSetiawanNo ratings yet
- Adenomatoid Odontogenic Tumour of Maxilla A Case ReportDocument6 pagesAdenomatoid Odontogenic Tumour of Maxilla A Case ReportAthenaeum Scientific PublishersNo ratings yet
- Tutorial 6 SK 4 Blok 13Document18 pagesTutorial 6 SK 4 Blok 13Mutiah Dwi ariniNo ratings yet
- Tutorial 6 SK 4 Blok 13Document19 pagesTutorial 6 SK 4 Blok 13Mutiah Dwi ariniNo ratings yet
- OmyxomaDocument6 pagesOmyxomaClaret TeneNo ratings yet
- Cystic Lesions of MandibleDocument18 pagesCystic Lesions of MandibleRahul ShindeNo ratings yet
- Bilateral Dentigerous CystDocument3 pagesBilateral Dentigerous CystjoseluisNo ratings yet
- A Radiolucency Is The Darker Area Within A Bone On A Conventional RadiographDocument83 pagesA Radiolucency Is The Darker Area Within A Bone On A Conventional Radiographkabir shaikhNo ratings yet
- Complex Odontoma: A Clinical Case ReportDocument5 pagesComplex Odontoma: A Clinical Case ReportkikiagrivitaNo ratings yet
- Endo-Perio Lesions Diagnosis and Clinical ConsiderationsDocument8 pagesEndo-Perio Lesions Diagnosis and Clinical ConsiderationsBejan OvidiuNo ratings yet
- Variasi Normal Torus Mandibula OvilDocument2 pagesVariasi Normal Torus Mandibula OvilAqilahaisarNo ratings yet
- CEMENTO2Document4 pagesCEMENTO2ton viet nguyenNo ratings yet
- Torus InglesDocument5 pagesTorus InglespaolaNo ratings yet
- An Unusual Case of 177 Pieces of Mandibular Compound Odontoma: 10-Year Follow-UpDocument4 pagesAn Unusual Case of 177 Pieces of Mandibular Compound Odontoma: 10-Year Follow-UpTrianita DivaNo ratings yet
- Benign Cementoblastoma - A Case ReportDocument3 pagesBenign Cementoblastoma - A Case ReportArafat Masud NiloyNo ratings yet
- Bilateral Maxillary Dentigerous Cysts - A Case ReportDocument3 pagesBilateral Maxillary Dentigerous Cysts - A Case ReportGregory NashNo ratings yet
- Cementoblastoma Journal PDFDocument3 pagesCementoblastoma Journal PDFBayu Indra LesmanaNo ratings yet
- Oral Maxillofacial RadiologiDocument5 pagesOral Maxillofacial RadiologiFlorasta CrewNo ratings yet
- EndoDocument3 pagesEndoJessicaLisaNugrohoNo ratings yet
- Imaging of Odontogenic InfectionsDocument14 pagesImaging of Odontogenic InfectionsMaria Corena100% (1)
- File MP926-1 3079-101-1 3173603Document19 pagesFile MP926-1 3079-101-1 3173603heruassociates2555No ratings yet
- Math 2Document5 pagesMath 2Alexandra BanaagNo ratings yet
- Company Law CREDocument16 pagesCompany Law CREayush gattaniNo ratings yet
- Umbilical Cord ProlapseDocument19 pagesUmbilical Cord ProlapsedenekeNo ratings yet
- IPS Emax For All-Ceramic Restorations Clinical SurDocument10 pagesIPS Emax For All-Ceramic Restorations Clinical Surjulist.tianNo ratings yet
- Outsystems Components and ToolsDocument18 pagesOutsystems Components and ToolsSaiKrishna MundretiNo ratings yet
- Cell Theory: Biology Scientific Theory CellsDocument5 pagesCell Theory: Biology Scientific Theory CellsNiel S. DefensorNo ratings yet
- Unit 8 Pag 79-82Document14 pagesUnit 8 Pag 79-82Kenny GamarraNo ratings yet
- GravitationDocument45 pagesGravitationthinkiit100% (1)
- ManuscriptDocument59 pagesManuscriptelijah maeNo ratings yet
- Welfare Policies of Dawar FootwearDocument110 pagesWelfare Policies of Dawar FootwearRohit Soni33% (3)
- Thesis It Na JudDocument38 pagesThesis It Na JudNepoy Beltran EntendezNo ratings yet
- ID Application FormDocument1 pageID Application FormMiguel MarinNo ratings yet
- Wills Under Indian Succession Act, 1925Document5 pagesWills Under Indian Succession Act, 1925Aeshita MarwahNo ratings yet
- Content Analysis-Cory AquinoDocument4 pagesContent Analysis-Cory AquinoDara Rose FilosofoNo ratings yet
- 20 de Thi HK 1 Tieng Anh 8 Co Dap AnDocument105 pages20 de Thi HK 1 Tieng Anh 8 Co Dap AnLinh Cao KhanhNo ratings yet
- Module 2 (JEEP 1)Document8 pagesModule 2 (JEEP 1)Angelito HalmainNo ratings yet
- Chapter - 2 - C - II Liver CirrhosisDocument39 pagesChapter - 2 - C - II Liver CirrhosisEmmaNo ratings yet
- The Prowess of AliguyonDocument4 pagesThe Prowess of AliguyonPauline Karen Macaisa-Concepcion100% (1)
- Scelsi: AionDocument3 pagesScelsi: AionSimon MathewsNo ratings yet
- Rapid Dutch Vol 1 PDFDocument20 pagesRapid Dutch Vol 1 PDFvhonNo ratings yet
- DanielledrippsresumegipDocument2 pagesDanielledrippsresumegipapi-400200010No ratings yet
- Q) 7) Describe Observation and Schedule MethodDocument6 pagesQ) 7) Describe Observation and Schedule Methodrashmi shreeNo ratings yet
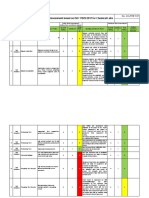
- Lab Risk Assessment Based On ISO 17025:2017 For Chemical LabsDocument5 pagesLab Risk Assessment Based On ISO 17025:2017 For Chemical Labsgristy100% (1)
- Hotel Reservation SystemaDocument11 pagesHotel Reservation SystemaVenus OlescoNo ratings yet
- BEED-525 FinalDocument17 pagesBEED-525 FinalMariecris Barayuga Duldulao-AbelaNo ratings yet