Download as pdf or txt
You might also like
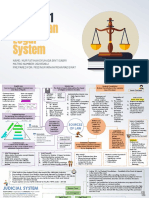
- Mind Mapping Chapter 1 Malaysian Legal SystemDocument3 pagesMind Mapping Chapter 1 Malaysian Legal Systemnur fatihah100% (1)
- Driver Record Screening Disclosure: Authorization For Release of Information For Employment ScreeningDocument1 pageDriver Record Screening Disclosure: Authorization For Release of Information For Employment ScreeningMucho FacerapeNo ratings yet
- Blue Shield CA Employee Enrollment Template v20160101Document8 pagesBlue Shield CA Employee Enrollment Template v20160101Anonymous RLktVcNo ratings yet
- Anthem Blue Cross Medical Enrollment Form 2014Document4 pagesAnthem Blue Cross Medical Enrollment Form 2014Tanveer ShaikhNo ratings yet
- Anthem Blue Cross California Individual Application 2011Document33 pagesAnthem Blue Cross California Individual Application 2011DennisNo ratings yet
- Servicemembers' Group Life Insurance Election and CertificateDocument4 pagesServicemembers' Group Life Insurance Election and CertificateChad ChriscoNo ratings yet
- COBRA General Notice Full VersionDocument14 pagesCOBRA General Notice Full VersionKristieNo ratings yet
- Policies Mutual AssistanceDocument4 pagesPolicies Mutual AssistanceDonna Fe Patiluna100% (1)
- Life Insurance-Shaiful ALICODocument6 pagesLife Insurance-Shaiful ALICOMahamudul Hassan RumiNo ratings yet
- JF Elite Plus Student Insurance Claim Form: ImportantDocument2 pagesJF Elite Plus Student Insurance Claim Form: ImportantJayesh GoplaniNo ratings yet
- Member Enrollment FormDocument3 pagesMember Enrollment FormVishnu Dev DeeviNo ratings yet
- Texas Employees Group Benefits Program (GBP) Supplemental Information Form For EmployeesDocument2 pagesTexas Employees Group Benefits Program (GBP) Supplemental Information Form For EmployeesBhargav Teja NukalaNo ratings yet
- Individual Change of Coverage Application CA 2011Document5 pagesIndividual Change of Coverage Application CA 2011Dennis AlexanderNo ratings yet
- Employee Enrollment Form: To Be Completed by EmployerDocument4 pagesEmployee Enrollment Form: To Be Completed by EmployerHarris HoneycuttNo ratings yet
- BrochuresDocument6 pagesBrochuresabdud.daiyaanNo ratings yet
- Employees Retirement System of Texas Texas Employees Group Benefits Program (GBP) Evidence of Insurability (EOI) Application Active/Retired EmployeesDocument5 pagesEmployees Retirement System of Texas Texas Employees Group Benefits Program (GBP) Evidence of Insurability (EOI) Application Active/Retired EmployeesCarroll MixsonNo ratings yet
- Correction Captains Association - Redacted HWMDocument17 pagesCorrection Captains Association - Redacted HWMAnonymous kprzCiZNo ratings yet
- BCBSIL Multistate Premier 2 SummaryDocument10 pagesBCBSIL Multistate Premier 2 SummaryMark MaNo ratings yet
- National Insurance Varistha Proposal FormDocument5 pagesNational Insurance Varistha Proposal FormAnirBanerjee0% (1)
- Secure Access 2015Document16 pagesSecure Access 2015api-288656991No ratings yet
- 2014 Bridging The Gap Colorado ApplicationDocument2 pages2014 Bridging The Gap Colorado ApplicationTodd GroveNo ratings yet
- W-1QMBR Medicare Savings Redetermination Form PDFDocument3 pagesW-1QMBR Medicare Savings Redetermination Form PDFehaegertNo ratings yet
- Family Club Membership Form, Benefits & TermsDocument4 pagesFamily Club Membership Form, Benefits & TermsPeterNo ratings yet
- ATD and LOA To Debit PremiumDocument2 pagesATD and LOA To Debit PremiumWalyn NagaNo ratings yet
- 55-0763 Fitness Reimbursement Form PDFDocument1 page55-0763 Fitness Reimbursement Form PDFChris HarbertNo ratings yet
- Hcps - Vet Insurance Form 16-17Document1 pageHcps - Vet Insurance Form 16-17api-325687960No ratings yet
- APRIL 1, 2011: Preferred Blue PPO Plan Blue Care Elect PPODocument19 pagesAPRIL 1, 2011: Preferred Blue PPO Plan Blue Care Elect PPOIan S. SandovalNo ratings yet
- W-1QMBR BlankDocument3 pagesW-1QMBR BlankehaegertNo ratings yet
- Recommendation - Kok Wee (New)Document3 pagesRecommendation - Kok Wee (New)Yew Shan ZhiNo ratings yet
- SG Simplecare Individuals ApplicationDocument8 pagesSG Simplecare Individuals Applicationmanishkpandey07No ratings yet
- Medicare and BTGC 2014Document4 pagesMedicare and BTGC 2014Todd GroveNo ratings yet
- 2019 Chicago Marathon Waiver and Commitment Form - Guaranteed ExDocument3 pages2019 Chicago Marathon Waiver and Commitment Form - Guaranteed ExSeanSean ParkNo ratings yet
- Anthem Dental Enrollment Enrollment Form 2014Document2 pagesAnthem Dental Enrollment Enrollment Form 2014Tanveer ShaikhNo ratings yet
- Member Enrollment Form - SMQDocument2 pagesMember Enrollment Form - SMQHussain bashaNo ratings yet
- Benefits Analysis Application Process FAX COVER LETTERDocument10 pagesBenefits Analysis Application Process FAX COVER LETTERmdugan5026No ratings yet
- Elizabeth A Winkowski - Thewoodlandsinnandresort - Fall2011Document26 pagesElizabeth A Winkowski - Thewoodlandsinnandresort - Fall2011studentATtempleNo ratings yet
- Parivar Proposal FormDocument10 pagesParivar Proposal FormHANSDA DHIRENDRANATHANNo ratings yet
- Life Insurance Plans 2013 - 2014 FINALDocument3 pagesLife Insurance Plans 2013 - 2014 FINALMattress Firm BenefitsNo ratings yet
- 46-7136 CL - Info Folder - ENDocument252 pages46-7136 CL - Info Folder - ENmenash23No ratings yet
- MLAMU Account Opening Form 1Document4 pagesMLAMU Account Opening Form 1Tumwine Kahweza ProsperNo ratings yet
- Employee Waiver FormDocument1 pageEmployee Waiver FormL.A Review CenterNo ratings yet
- GHS Declaration-2Document2 pagesGHS Declaration-2estrade1112No ratings yet
- Prudential PruPersonal AccidentDocument13 pagesPrudential PruPersonal AccidentpriscillasooNo ratings yet
- 11036Document28 pages11036api-309082881No ratings yet
- 2024-2025 Resident and Fellow Salary Benefits Sheet FULL (1)Document37 pages2024-2025 Resident and Fellow Salary Benefits Sheet FULL (1)Brian HelbigNo ratings yet
- WMED Outbound ApplicationDocument1 pageWMED Outbound ApplicationMichael ZhangNo ratings yet
- Employee Enrollment Application: Group Size 51+ Eligible Employees - Medically UnderwrittenDocument6 pagesEmployee Enrollment Application: Group Size 51+ Eligible Employees - Medically Underwrittenmdugan5026No ratings yet
- MifDocument2 pagesMifpatilshashiNo ratings yet
- 2018 Membership FormpdfDocument1 page2018 Membership Formpdfapi-308949534No ratings yet
- Bupa Advantage Care Membership GuideDocument40 pagesBupa Advantage Care Membership GuidePatricia GuzmanNo ratings yet
- Diplomat America BrochureDocument8 pagesDiplomat America BrochurelytdakkaNo ratings yet
- IHP Proposal FormDocument9 pagesIHP Proposal FormDeepakNo ratings yet
- 10-17-23 Midtown Membership Agreement One PageDocument1 page10-17-23 Midtown Membership Agreement One PagebodybyonderNo ratings yet
- Eskwela Davao Application Form (Blank)Document2 pagesEskwela Davao Application Form (Blank)Aljeania Marie M. MolialNo ratings yet
- Eskwela Davao Application Form (Blank)Document2 pagesEskwela Davao Application Form (Blank)no one33% (3)
- TD Insurance Product GuideDocument39 pagesTD Insurance Product Guidetake.a.chance123456No ratings yet
- Mrs Client 100k SPWL WiDocument8 pagesMrs Client 100k SPWL WikubusipitNo ratings yet
- Your Summary Plan Description: Cognizant Technology Solutions US CorpDocument37 pagesYour Summary Plan Description: Cognizant Technology Solutions US CorpKishore ViswanathanNo ratings yet
- 2012 Middlebury College Vountary Insurance Application PDFDocument1 page2012 Middlebury College Vountary Insurance Application PDFJorge SayãoNo ratings yet
- Question For Term InsuranceDocument3 pagesQuestion For Term Insuranceradhika jagtapNo ratings yet
- How to Enroll in Medicare Health Insurance: Choose a Medicare Part D Drug Plan and a Medicare Supplement PlanFrom EverandHow to Enroll in Medicare Health Insurance: Choose a Medicare Part D Drug Plan and a Medicare Supplement PlanNo ratings yet
- Simple Interest FinalDocument15 pagesSimple Interest FinalJennifer AcedoNo ratings yet
- Farinas vs. Executive Secretary 463 Phil. 179 Dec 10, 2003 Callejo SR, J., FactsDocument4 pagesFarinas vs. Executive Secretary 463 Phil. 179 Dec 10, 2003 Callejo SR, J., FactsSbl IrvNo ratings yet
- Rethinking Domestic Violence 9780774813044 0774813040 9780774810159 9780774855112 9780774859875 - CompressDocument430 pagesRethinking Domestic Violence 9780774813044 0774813040 9780774810159 9780774855112 9780774859875 - CompressJerome Love100% (1)
- Administrative Order No. 99 - 57 December 27, 1999: Subject: Amendments ToDocument34 pagesAdministrative Order No. 99 - 57 December 27, 1999: Subject: Amendments ToMai UgayNo ratings yet
- Monitoring and Evaluation Team Organizational Set-Up: Jolan B. TorresDocument1 pageMonitoring and Evaluation Team Organizational Set-Up: Jolan B. TorresWinston CelestialNo ratings yet
- Report (2023!12!08 Sagadahoc County Sheriff's Office) ADocument97 pagesReport (2023!12!08 Sagadahoc County Sheriff's Office) ANEWS CENTER Maine100% (1)
- Case 1Document8 pagesCase 1michaelalterfabrikNo ratings yet
- Plane & Spherical Trigonometry: Engr. Marvin Y. Villorente, ECE, ECTDocument59 pagesPlane & Spherical Trigonometry: Engr. Marvin Y. Villorente, ECE, ECTMira Alvarez100% (2)
- ONG CHENG WAH & ANOR v. SUPRAMANIAM ARJUNANDocument20 pagesONG CHENG WAH & ANOR v. SUPRAMANIAM ARJUNANNur Syahindah Shamsul AzmanNo ratings yet
- Iaomr State Chapter Application FormDocument3 pagesIaomr State Chapter Application Formsgoeldoc_550661200No ratings yet
- HSE Alert 61-20 Heavy Equipment Operator-Rigger ValidationDocument1 pageHSE Alert 61-20 Heavy Equipment Operator-Rigger ValidationaswinNo ratings yet
- Rules Group 'B'Document25 pagesRules Group 'B'DivyaNo ratings yet
- Law Firms List 2Document13 pagesLaw Firms List 2Reena ShauNo ratings yet
- Cipl PancatirtaDocument2 pagesCipl Pancatirtak dodi priantoNo ratings yet
- Amity University Jharkhand Ranchi Project On INDIAN PARTNERSHIP ACT Act 1932 by Kirti Sabran A35101919003Document7 pagesAmity University Jharkhand Ranchi Project On INDIAN PARTNERSHIP ACT Act 1932 by Kirti Sabran A35101919003RaviNo ratings yet
- In The High Court of Judicature of . AT ..: ..Petitioners/Appellants andDocument4 pagesIn The High Court of Judicature of . AT ..: ..Petitioners/Appellants andSathish KumarNo ratings yet
- DAVIES - HOPT. Control Transactions - The Anatomy of Corporate Law PDFDocument26 pagesDAVIES - HOPT. Control Transactions - The Anatomy of Corporate Law PDFSushil JindalNo ratings yet
- Segment 002 of DIRM Search - 158745 - PDF-RDocument251 pagesSegment 002 of DIRM Search - 158745 - PDF-R420leaksNo ratings yet
- Labor Law Review Implementing Rules and RegulationsDocument2 pagesLabor Law Review Implementing Rules and RegulationsRaffy LopezNo ratings yet
- Government of Andhra Pradesh: (By Order and in The Name of The Governor of Andhra Pradesh)Document2 pagesGovernment of Andhra Pradesh: (By Order and in The Name of The Governor of Andhra Pradesh)syed haneefNo ratings yet
- DANIEL A. VILLAREAL, JR. (On Behalf of Orlando A. Villareal) vs. METROPOLITAN WATERWORKS AND SEWERAGE SYSTEM (MWSS)Document2 pagesDANIEL A. VILLAREAL, JR. (On Behalf of Orlando A. Villareal) vs. METROPOLITAN WATERWORKS AND SEWERAGE SYSTEM (MWSS)quejarra de asis100% (1)
- People vs. CagalinganDocument9 pagesPeople vs. Cagalinganprecy926No ratings yet
- An Overview of Major Laws Affecting BusinessDocument5 pagesAn Overview of Major Laws Affecting BusinessSharwan SinghNo ratings yet
- What Is A Process ServerDocument3 pagesWhat Is A Process ServergeorgebarleyNo ratings yet
- Barangay ClearanceDocument1 pageBarangay ClearanceBarangay SamputNo ratings yet
- Amazing LoveDocument5 pagesAmazing LoveReynald Ian CruzNo ratings yet