
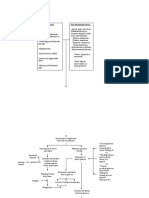
Pathophysiology Diabetes Mellitus: Otential That The Children of Diabetic Mothers Will Also
Pathophysiology Diabetes Mellitus: Otential That The Children of Diabetic Mothers Will Also
You might also like
- Instant Download Ebook PDF Fundamentals of Abnormal Psychology 9th Edition PDF ScribdDocument47 pagesInstant Download Ebook PDF Fundamentals of Abnormal Psychology 9th Edition PDF Scribdjohn.aki332100% (46)
- 981-0602 Onan MDKUB MDKWB Spec E-J Install Manual (2-2010)Document65 pages981-0602 Onan MDKUB MDKWB Spec E-J Install Manual (2-2010)pepa 007No ratings yet
- Carbohydrates (Page 7-9) GarbosaDocument7 pagesCarbohydrates (Page 7-9) GarbosaRej GarbosaNo ratings yet
- Gangstalking - IncompleteDocument37 pagesGangstalking - IncompleteBob WilliamsNo ratings yet
- Pathophysiology Diabetes MellitusDocument14 pagesPathophysiology Diabetes MellitusKevin Van Eric O. SaballoNo ratings yet
- Managing For Client With Diabetic MellitusDocument23 pagesManaging For Client With Diabetic MellitusNur HikmaNo ratings yet
- Law and Disorder - Type 1 Diabetes TemplateDocument3 pagesLaw and Disorder - Type 1 Diabetes Templateapi-371785797No ratings yet
- Jurnal 10Document8 pagesJurnal 10Muhammad RidhoNo ratings yet
- Diabetic Mellitus and Nursing ManagementDocument57 pagesDiabetic Mellitus and Nursing ManagementSukses TinggiNo ratings yet
- DM Type II ReportDocument7 pagesDM Type II Reportgigolo13No ratings yet
- Mechanism of Diabetes Mellitus: and How Does It Affect Health StatusDocument29 pagesMechanism of Diabetes Mellitus: and How Does It Affect Health StatusVARITPOL CHAROENYINGPAISALNo ratings yet
- Activity Part 1Document7 pagesActivity Part 1xiumethemoneyNo ratings yet
- Diabetes and Your Health: Monitoring Your Glucose LevelsDocument3 pagesDiabetes and Your Health: Monitoring Your Glucose Levelswiwin haryantoniNo ratings yet
- Pathogenesis of Obesity: Josanne VassalloDocument4 pagesPathogenesis of Obesity: Josanne VassalloAdkhiatul MuslihatinNo ratings yet
- CM Glucose and KetonesDocument3 pagesCM Glucose and Ketonesbaby ENo ratings yet
- Guia Del EspiritistaDocument8 pagesGuia Del Espiritistaxander trujilloNo ratings yet
- Intrauterine Programming of Physiological Systems: Causes and ConsequencesDocument9 pagesIntrauterine Programming of Physiological Systems: Causes and ConsequencesSandhy PrayudhanaNo ratings yet
- Gestational Diabetes Mellitus Third Trimester-There Is Rapid Decrease inDocument5 pagesGestational Diabetes Mellitus Third Trimester-There Is Rapid Decrease inOona Nicole DioricoNo ratings yet
- DM BrochureDocument3 pagesDM BrochureGrape JuiceNo ratings yet
- DM Type 2Document13 pagesDM Type 2Yssah Moira HamacNo ratings yet
- Ob PrelimsDocument13 pagesOb PrelimseliNo ratings yet
- Diabetes Mellitus Diabetes Mellitus DR Prakash H M DR Prakash H MDocument85 pagesDiabetes Mellitus Diabetes Mellitus DR Prakash H M DR Prakash H MrogeriotascaNo ratings yet
- Rumination Syndrome: A Difficult Diagnosis and TreatmentDocument6 pagesRumination Syndrome: A Difficult Diagnosis and TreatmentJaya TevesNo ratings yet
- 118A - Liver-Failure Handout #5 (Sir Marvin)Document5 pages118A - Liver-Failure Handout #5 (Sir Marvin)Joanna TaylanNo ratings yet
- Revision Pe 1 (Kalppena Naidu)Document11 pagesRevision Pe 1 (Kalppena Naidu)vinoedhnaidu_rajagopalNo ratings yet
- Environmental FactorsDocument7 pagesEnvironmental FactorsjayrchinNo ratings yet
- Etiology: Predisposing Factors Present JustificationDocument3 pagesEtiology: Predisposing Factors Present Justificationelvie21No ratings yet
- Diagnosis and Classi Fication of Diabetes Mellitus: Merican Iabetes SsociationDocument8 pagesDiagnosis and Classi Fication of Diabetes Mellitus: Merican Iabetes Ssociationzahriz zaitunNo ratings yet
- Pathophysiology CKD - DrawioDocument54 pagesPathophysiology CKD - DrawioGwyneth CiriloNo ratings yet
- Endocrine System Disorders Endocrine Disorders - Too Much GigantismDocument4 pagesEndocrine System Disorders Endocrine Disorders - Too Much GigantismDhea Angela A. CapuyanNo ratings yet
- The Gut: A Key To The Pathogenesis of Type 2 Diabetes?: ReviewDocument4 pagesThe Gut: A Key To The Pathogenesis of Type 2 Diabetes?: ReviewOlesiaNo ratings yet
- Essentials of Clinical Periodontology and Periodontics 5th Ed (1) - Pages-2Document3 pagesEssentials of Clinical Periodontology and Periodontics 5th Ed (1) - Pages-2Diana AjengNo ratings yet
- OB PathophysiologyDocument2 pagesOB PathophysiologyCathy SantosNo ratings yet
- Schem Di 4th FloorDocument19 pagesSchem Di 4th FloorMark Ianne AngNo ratings yet
- Physiological: Basis ofDocument28 pagesPhysiological: Basis ofArnab RayNo ratings yet
- Concept Map Diabetes Mellitus GROUP4Document2 pagesConcept Map Diabetes Mellitus GROUP4ALIZA BAKILNo ratings yet
- Physiology of Starvation and Refeeding SyndromeDocument11 pagesPhysiology of Starvation and Refeeding SyndromeUCI COVID Pediátrico HNGAINo ratings yet
- Week 7 Diabetes MellitusDocument8 pagesWeek 7 Diabetes MellitusJiro MarianoNo ratings yet
- Endocrinology: I. Basic PrinciplesDocument14 pagesEndocrinology: I. Basic PrinciplesBenjamin NgNo ratings yet
- CASE STUDY #5 Endocrine System (Diabetes)Document6 pagesCASE STUDY #5 Endocrine System (Diabetes)Lerma PagcaliwanganNo ratings yet
- Diabetes Mellitus 1Document5 pagesDiabetes Mellitus 1Xarius FidelNo ratings yet
- Prepregnancy and Preconception NutritionDocument4 pagesPrepregnancy and Preconception NutritionNobiliary ortizNo ratings yet
- A Pregnant Woman With Diabetes Mellitus Diabetes Mellitus Type 1 DiabetesDocument5 pagesA Pregnant Woman With Diabetes Mellitus Diabetes Mellitus Type 1 Diabeteskenken the ExplorerNo ratings yet
- Nutri Lab2 CARBOHYDRATES-1Document7 pagesNutri Lab2 CARBOHYDRATES-1Maria Elvira Abrogena DuadNo ratings yet
- DiabetesDocument170 pagesDiabetesKoRnflakesNo ratings yet
- Pregestational ConditionDocument7 pagesPregestational ConditionCamille UlepNo ratings yet
- BSN 2B B2 TERATOGENS Metabolic ConditionsDocument5 pagesBSN 2B B2 TERATOGENS Metabolic ConditionsDANIEL SAENSANOHNo ratings yet
- Diabetes 316 LecDocument6 pagesDiabetes 316 LecKatherine BautistaNo ratings yet
- Physiology of DiabetesDocument52 pagesPhysiology of DiabetesPhysiology by Dr RaghuveerNo ratings yet
- Ally Omary Mwambela MD2Document10 pagesAlly Omary Mwambela MD2Ally OmaryNo ratings yet
- PATHODocument2 pagesPATHOjunrey1990No ratings yet
- DiabetesDocument170 pagesDiabetesMarvin Dela CruzNo ratings yet
- Diabetes Mellitus-Pathophysiology & Herbal Management: Pharmaceutical and Biosciences Journal September 2017Document10 pagesDiabetes Mellitus-Pathophysiology & Herbal Management: Pharmaceutical and Biosciences Journal September 2017Siti AnisaNo ratings yet
- Refeeding SyndromeDocument10 pagesRefeeding SyndromePhysiology by Dr RaghuveerNo ratings yet
- Diabetes and PeriodontitisDocument25 pagesDiabetes and PeriodontitisAmrutha KasinaNo ratings yet
- Diabetes MellitusDocument32 pagesDiabetes MellitusGloria KikiNo ratings yet
- Pa Tho ReviseDocument10 pagesPa Tho ReviseCharl SembranoNo ratings yet
- Carbohydrate DisorderDocument74 pagesCarbohydrate DisorderEric YewNo ratings yet
- Maps of KwashiorkorDocument9 pagesMaps of KwashiorkorScribdTranslationsNo ratings yet
- Shafiullah PDFDocument12 pagesShafiullah PDFMayra PereiraNo ratings yet
- Care of Clients With Glucose Metabolism ProblemsDocument5 pagesCare of Clients With Glucose Metabolism ProblemsRyel Lixel DivinagraciaNo ratings yet
- Diabetes CipDocument3 pagesDiabetes CipLlang LleavNo ratings yet
- HLTH 102 Photovoice ProjectDocument8 pagesHLTH 102 Photovoice Projectapi-500574206No ratings yet
- Francisco GS Conference March 2022Document69 pagesFrancisco GS Conference March 2022SamuelNo ratings yet
- PJI NEJMoa2020198Document11 pagesPJI NEJMoa2020198dwi.and1989No ratings yet
- Bacolod Assignment in P.EDocument6 pagesBacolod Assignment in P.EQueenie BacolodNo ratings yet
- Encapsulation of Curcumin in Self-Assembling Peptide Hydrogels As Injectable Drug Delivery Vehicles - Paper RevisionDocument2 pagesEncapsulation of Curcumin in Self-Assembling Peptide Hydrogels As Injectable Drug Delivery Vehicles - Paper RevisionAna Mary GCNo ratings yet
- ANCA Mosaic 3Document12 pagesANCA Mosaic 3vemalNo ratings yet
- Heroes Act SummaryDocument71 pagesHeroes Act SummaryFedSmith Inc.100% (2)
- Master Test in Mapeh 8Document4 pagesMaster Test in Mapeh 8Wendyl SullanoNo ratings yet
- OperculectomyDocument4 pagesOperculectomyshania arifinNo ratings yet
- Sy FC Sem 3 Full NotesDocument59 pagesSy FC Sem 3 Full Notes081 Om DhuriNo ratings yet
- Buttaravoli, Philip - Minor Emergencies - Blunt Scrotal Trauma (2007)Document3 pagesButtaravoli, Philip - Minor Emergencies - Blunt Scrotal Trauma (2007)Vivian ChanNo ratings yet
- Sarker Maruf - Final DraftDocument6 pagesSarker Maruf - Final DraftSarker MarufNo ratings yet
- Tofik M .Clinical Audit Project Proposal PDFDocument16 pagesTofik M .Clinical Audit Project Proposal PDFMerwan KemalNo ratings yet
- LincolnWeld 860 FluxDocument25 pagesLincolnWeld 860 FluxPubcrawlNo ratings yet
- The Breath Sounds: Intensity (Or Loudness)Document6 pagesThe Breath Sounds: Intensity (Or Loudness)Santhosh KumarNo ratings yet
- Anti-Thyroid DrugsDocument60 pagesAnti-Thyroid DrugsApurba Sarker Apu100% (1)
- Gastrointestinal Pathology Case Studies ParDocument2 pagesGastrointestinal Pathology Case Studies Pardr nirupamaNo ratings yet
- Effect of Denture Cleansers On Color Stability, Surface Roughness, and Hardness of Different Denture Base ResinsDocument7 pagesEffect of Denture Cleansers On Color Stability, Surface Roughness, and Hardness of Different Denture Base ResinsZainb SabahNo ratings yet
- HyperlipidemiaDocument17 pagesHyperlipidemiabent alfay7a2No ratings yet
- AppreciationDocument10 pagesAppreciationProjek JK3No ratings yet
- Nurses' Attitude On The Use of Personal Protective Equipment (Ppe) in Emergency Room of Dr. Slamet Hospital GarutDocument9 pagesNurses' Attitude On The Use of Personal Protective Equipment (Ppe) in Emergency Room of Dr. Slamet Hospital GarutDede NunuNo ratings yet
- Prioritization and Ranking CHN RLEDocument5 pagesPrioritization and Ranking CHN RLESherry Ann FayeNo ratings yet
- Pe Grade9 QTR1 Module1Document37 pagesPe Grade9 QTR1 Module1Jp DiolaNo ratings yet
- Tooth Regeneration: A Revolution in Stomatology and Evolution in Regenerative MedicineDocument10 pagesTooth Regeneration: A Revolution in Stomatology and Evolution in Regenerative MedicineElize B.No ratings yet
- DRUG STUDY Furosemide LasixDocument1 pageDRUG STUDY Furosemide LasixG4 AMOYO ANGELICA NICOLENo ratings yet
- Saliers V Walmart:Hy-VeeDocument43 pagesSaliers V Walmart:Hy-VeeUncoverDCNo ratings yet
- Pathophysiology of CVD InfarctDocument2 pagesPathophysiology of CVD InfarctIris Caberte86% (7)

























































































Download as docx, pdf, or txt
You might also like
- Instant Download Ebook PDF Fundamentals of Abnormal Psychology 9th Edition PDF ScribdDocument47 pagesInstant Download Ebook PDF Fundamentals of Abnormal Psychology 9th Edition PDF Scribdjohn.aki332100% (46)
- 981-0602 Onan MDKUB MDKWB Spec E-J Install Manual (2-2010)Document65 pages981-0602 Onan MDKUB MDKWB Spec E-J Install Manual (2-2010)pepa 007No ratings yet
- Carbohydrates (Page 7-9) GarbosaDocument7 pagesCarbohydrates (Page 7-9) GarbosaRej GarbosaNo ratings yet
- Gangstalking - IncompleteDocument37 pagesGangstalking - IncompleteBob WilliamsNo ratings yet
- Pathophysiology Diabetes MellitusDocument14 pagesPathophysiology Diabetes MellitusKevin Van Eric O. SaballoNo ratings yet
- Managing For Client With Diabetic MellitusDocument23 pagesManaging For Client With Diabetic MellitusNur HikmaNo ratings yet
- Law and Disorder - Type 1 Diabetes TemplateDocument3 pagesLaw and Disorder - Type 1 Diabetes Templateapi-371785797No ratings yet
- Jurnal 10Document8 pagesJurnal 10Muhammad RidhoNo ratings yet
- Diabetic Mellitus and Nursing ManagementDocument57 pagesDiabetic Mellitus and Nursing ManagementSukses TinggiNo ratings yet
- DM Type II ReportDocument7 pagesDM Type II Reportgigolo13No ratings yet
- Mechanism of Diabetes Mellitus: and How Does It Affect Health StatusDocument29 pagesMechanism of Diabetes Mellitus: and How Does It Affect Health StatusVARITPOL CHAROENYINGPAISALNo ratings yet
- Activity Part 1Document7 pagesActivity Part 1xiumethemoneyNo ratings yet
- Diabetes and Your Health: Monitoring Your Glucose LevelsDocument3 pagesDiabetes and Your Health: Monitoring Your Glucose Levelswiwin haryantoniNo ratings yet
- Pathogenesis of Obesity: Josanne VassalloDocument4 pagesPathogenesis of Obesity: Josanne VassalloAdkhiatul MuslihatinNo ratings yet
- CM Glucose and KetonesDocument3 pagesCM Glucose and Ketonesbaby ENo ratings yet
- Guia Del EspiritistaDocument8 pagesGuia Del Espiritistaxander trujilloNo ratings yet
- Intrauterine Programming of Physiological Systems: Causes and ConsequencesDocument9 pagesIntrauterine Programming of Physiological Systems: Causes and ConsequencesSandhy PrayudhanaNo ratings yet
- Gestational Diabetes Mellitus Third Trimester-There Is Rapid Decrease inDocument5 pagesGestational Diabetes Mellitus Third Trimester-There Is Rapid Decrease inOona Nicole DioricoNo ratings yet
- DM BrochureDocument3 pagesDM BrochureGrape JuiceNo ratings yet
- DM Type 2Document13 pagesDM Type 2Yssah Moira HamacNo ratings yet
- Ob PrelimsDocument13 pagesOb PrelimseliNo ratings yet
- Diabetes Mellitus Diabetes Mellitus DR Prakash H M DR Prakash H MDocument85 pagesDiabetes Mellitus Diabetes Mellitus DR Prakash H M DR Prakash H MrogeriotascaNo ratings yet
- Rumination Syndrome: A Difficult Diagnosis and TreatmentDocument6 pagesRumination Syndrome: A Difficult Diagnosis and TreatmentJaya TevesNo ratings yet
- 118A - Liver-Failure Handout #5 (Sir Marvin)Document5 pages118A - Liver-Failure Handout #5 (Sir Marvin)Joanna TaylanNo ratings yet
- Revision Pe 1 (Kalppena Naidu)Document11 pagesRevision Pe 1 (Kalppena Naidu)vinoedhnaidu_rajagopalNo ratings yet
- Environmental FactorsDocument7 pagesEnvironmental FactorsjayrchinNo ratings yet
- Etiology: Predisposing Factors Present JustificationDocument3 pagesEtiology: Predisposing Factors Present Justificationelvie21No ratings yet
- Diagnosis and Classi Fication of Diabetes Mellitus: Merican Iabetes SsociationDocument8 pagesDiagnosis and Classi Fication of Diabetes Mellitus: Merican Iabetes Ssociationzahriz zaitunNo ratings yet
- Pathophysiology CKD - DrawioDocument54 pagesPathophysiology CKD - DrawioGwyneth CiriloNo ratings yet
- Endocrine System Disorders Endocrine Disorders - Too Much GigantismDocument4 pagesEndocrine System Disorders Endocrine Disorders - Too Much GigantismDhea Angela A. CapuyanNo ratings yet
- The Gut: A Key To The Pathogenesis of Type 2 Diabetes?: ReviewDocument4 pagesThe Gut: A Key To The Pathogenesis of Type 2 Diabetes?: ReviewOlesiaNo ratings yet
- Essentials of Clinical Periodontology and Periodontics 5th Ed (1) - Pages-2Document3 pagesEssentials of Clinical Periodontology and Periodontics 5th Ed (1) - Pages-2Diana AjengNo ratings yet
- OB PathophysiologyDocument2 pagesOB PathophysiologyCathy SantosNo ratings yet
- Schem Di 4th FloorDocument19 pagesSchem Di 4th FloorMark Ianne AngNo ratings yet
- Physiological: Basis ofDocument28 pagesPhysiological: Basis ofArnab RayNo ratings yet
- Concept Map Diabetes Mellitus GROUP4Document2 pagesConcept Map Diabetes Mellitus GROUP4ALIZA BAKILNo ratings yet
- Physiology of Starvation and Refeeding SyndromeDocument11 pagesPhysiology of Starvation and Refeeding SyndromeUCI COVID Pediátrico HNGAINo ratings yet
- Week 7 Diabetes MellitusDocument8 pagesWeek 7 Diabetes MellitusJiro MarianoNo ratings yet
- Endocrinology: I. Basic PrinciplesDocument14 pagesEndocrinology: I. Basic PrinciplesBenjamin NgNo ratings yet
- CASE STUDY #5 Endocrine System (Diabetes)Document6 pagesCASE STUDY #5 Endocrine System (Diabetes)Lerma PagcaliwanganNo ratings yet
- Diabetes Mellitus 1Document5 pagesDiabetes Mellitus 1Xarius FidelNo ratings yet
- Prepregnancy and Preconception NutritionDocument4 pagesPrepregnancy and Preconception NutritionNobiliary ortizNo ratings yet
- A Pregnant Woman With Diabetes Mellitus Diabetes Mellitus Type 1 DiabetesDocument5 pagesA Pregnant Woman With Diabetes Mellitus Diabetes Mellitus Type 1 Diabeteskenken the ExplorerNo ratings yet
- Nutri Lab2 CARBOHYDRATES-1Document7 pagesNutri Lab2 CARBOHYDRATES-1Maria Elvira Abrogena DuadNo ratings yet
- DiabetesDocument170 pagesDiabetesKoRnflakesNo ratings yet
- Pregestational ConditionDocument7 pagesPregestational ConditionCamille UlepNo ratings yet
- BSN 2B B2 TERATOGENS Metabolic ConditionsDocument5 pagesBSN 2B B2 TERATOGENS Metabolic ConditionsDANIEL SAENSANOHNo ratings yet
- Diabetes 316 LecDocument6 pagesDiabetes 316 LecKatherine BautistaNo ratings yet
- Physiology of DiabetesDocument52 pagesPhysiology of DiabetesPhysiology by Dr RaghuveerNo ratings yet
- Ally Omary Mwambela MD2Document10 pagesAlly Omary Mwambela MD2Ally OmaryNo ratings yet
- PATHODocument2 pagesPATHOjunrey1990No ratings yet
- DiabetesDocument170 pagesDiabetesMarvin Dela CruzNo ratings yet
- Diabetes Mellitus-Pathophysiology & Herbal Management: Pharmaceutical and Biosciences Journal September 2017Document10 pagesDiabetes Mellitus-Pathophysiology & Herbal Management: Pharmaceutical and Biosciences Journal September 2017Siti AnisaNo ratings yet
- Refeeding SyndromeDocument10 pagesRefeeding SyndromePhysiology by Dr RaghuveerNo ratings yet
- Diabetes and PeriodontitisDocument25 pagesDiabetes and PeriodontitisAmrutha KasinaNo ratings yet
- Diabetes MellitusDocument32 pagesDiabetes MellitusGloria KikiNo ratings yet
- Pa Tho ReviseDocument10 pagesPa Tho ReviseCharl SembranoNo ratings yet
- Carbohydrate DisorderDocument74 pagesCarbohydrate DisorderEric YewNo ratings yet
- Maps of KwashiorkorDocument9 pagesMaps of KwashiorkorScribdTranslationsNo ratings yet
- Shafiullah PDFDocument12 pagesShafiullah PDFMayra PereiraNo ratings yet
- Care of Clients With Glucose Metabolism ProblemsDocument5 pagesCare of Clients With Glucose Metabolism ProblemsRyel Lixel DivinagraciaNo ratings yet
- Diabetes CipDocument3 pagesDiabetes CipLlang LleavNo ratings yet
- HLTH 102 Photovoice ProjectDocument8 pagesHLTH 102 Photovoice Projectapi-500574206No ratings yet
- Francisco GS Conference March 2022Document69 pagesFrancisco GS Conference March 2022SamuelNo ratings yet
- PJI NEJMoa2020198Document11 pagesPJI NEJMoa2020198dwi.and1989No ratings yet
- Bacolod Assignment in P.EDocument6 pagesBacolod Assignment in P.EQueenie BacolodNo ratings yet
- Encapsulation of Curcumin in Self-Assembling Peptide Hydrogels As Injectable Drug Delivery Vehicles - Paper RevisionDocument2 pagesEncapsulation of Curcumin in Self-Assembling Peptide Hydrogels As Injectable Drug Delivery Vehicles - Paper RevisionAna Mary GCNo ratings yet
- ANCA Mosaic 3Document12 pagesANCA Mosaic 3vemalNo ratings yet
- Heroes Act SummaryDocument71 pagesHeroes Act SummaryFedSmith Inc.100% (2)
- Master Test in Mapeh 8Document4 pagesMaster Test in Mapeh 8Wendyl SullanoNo ratings yet
- OperculectomyDocument4 pagesOperculectomyshania arifinNo ratings yet
- Sy FC Sem 3 Full NotesDocument59 pagesSy FC Sem 3 Full Notes081 Om DhuriNo ratings yet
- Buttaravoli, Philip - Minor Emergencies - Blunt Scrotal Trauma (2007)Document3 pagesButtaravoli, Philip - Minor Emergencies - Blunt Scrotal Trauma (2007)Vivian ChanNo ratings yet
- Sarker Maruf - Final DraftDocument6 pagesSarker Maruf - Final DraftSarker MarufNo ratings yet
- Tofik M .Clinical Audit Project Proposal PDFDocument16 pagesTofik M .Clinical Audit Project Proposal PDFMerwan KemalNo ratings yet
- LincolnWeld 860 FluxDocument25 pagesLincolnWeld 860 FluxPubcrawlNo ratings yet
- The Breath Sounds: Intensity (Or Loudness)Document6 pagesThe Breath Sounds: Intensity (Or Loudness)Santhosh KumarNo ratings yet
- Anti-Thyroid DrugsDocument60 pagesAnti-Thyroid DrugsApurba Sarker Apu100% (1)
- Gastrointestinal Pathology Case Studies ParDocument2 pagesGastrointestinal Pathology Case Studies Pardr nirupamaNo ratings yet
- Effect of Denture Cleansers On Color Stability, Surface Roughness, and Hardness of Different Denture Base ResinsDocument7 pagesEffect of Denture Cleansers On Color Stability, Surface Roughness, and Hardness of Different Denture Base ResinsZainb SabahNo ratings yet
- HyperlipidemiaDocument17 pagesHyperlipidemiabent alfay7a2No ratings yet
- AppreciationDocument10 pagesAppreciationProjek JK3No ratings yet
- Nurses' Attitude On The Use of Personal Protective Equipment (Ppe) in Emergency Room of Dr. Slamet Hospital GarutDocument9 pagesNurses' Attitude On The Use of Personal Protective Equipment (Ppe) in Emergency Room of Dr. Slamet Hospital GarutDede NunuNo ratings yet
- Prioritization and Ranking CHN RLEDocument5 pagesPrioritization and Ranking CHN RLESherry Ann FayeNo ratings yet
- Pe Grade9 QTR1 Module1Document37 pagesPe Grade9 QTR1 Module1Jp DiolaNo ratings yet
- Tooth Regeneration: A Revolution in Stomatology and Evolution in Regenerative MedicineDocument10 pagesTooth Regeneration: A Revolution in Stomatology and Evolution in Regenerative MedicineElize B.No ratings yet
- DRUG STUDY Furosemide LasixDocument1 pageDRUG STUDY Furosemide LasixG4 AMOYO ANGELICA NICOLENo ratings yet
- Saliers V Walmart:Hy-VeeDocument43 pagesSaliers V Walmart:Hy-VeeUncoverDCNo ratings yet
- Pathophysiology of CVD InfarctDocument2 pagesPathophysiology of CVD InfarctIris Caberte86% (7)