Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5833)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Crash Cart Lecture-WhiteDocument103 pagesCrash Cart Lecture-WhiteMarianne Laylo75% (4)
- The Hormone HandbookDocument74 pagesThe Hormone Handbookvictoria100% (2)
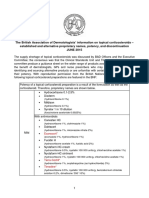
- Topical Corticosteroid Supply Shortage GuidanceDocument3 pagesTopical Corticosteroid Supply Shortage GuidancesyahrulroziNo ratings yet
- TrendCare User GuidelinesDocument11 pagesTrendCare User GuidelinesRidha SyahputraNo ratings yet
- Narayana Hurdyalaya Business Model CanvasDocument7 pagesNarayana Hurdyalaya Business Model CanvasShubham SinhaNo ratings yet
- Date/ Time Cues Needs Nursing Diagnosis Scientific Basis Goals Objectives Criteria Nursing Interventions Rationale EvaluationDocument2 pagesDate/ Time Cues Needs Nursing Diagnosis Scientific Basis Goals Objectives Criteria Nursing Interventions Rationale EvaluationJhensczy Hazel Maye AlbaNo ratings yet
- TireotoxicozaDocument3 pagesTireotoxicozaDragos PopoviciNo ratings yet
- Concept of Pharmacodynamics and Pharmacokinetics in AyurvedaDocument8 pagesConcept of Pharmacodynamics and Pharmacokinetics in AyurvedaBalaji Kumar PanigrahiNo ratings yet
- Manchester Triage System A Global SolutionDocument41 pagesManchester Triage System A Global Solutioneman sulaiman100% (1)
- Growth ChartDocument13 pagesGrowth Chartp1843dNo ratings yet
- Disease Summary of Common SymptomsDocument1 pageDisease Summary of Common SymptomsJeffrey CohenNo ratings yet
- Hanashima Et Al. - 2009 - A Study Regarding Occlusal Plane and Posterior Disocclusion-AnnotatedDocument8 pagesHanashima Et Al. - 2009 - A Study Regarding Occlusal Plane and Posterior Disocclusion-AnnotatedJonathan GIraldo Martinez100% (1)
- Stok Per TGL 11 Januari 2022Document77 pagesStok Per TGL 11 Januari 2022Bambang hendrawanNo ratings yet
- Cholesteatoma SurgeryDocument4 pagesCholesteatoma SurgeryJad KafrouniNo ratings yet
- 4357 - 22.Dr - Ravindra B. Gunale1 DR - Prajakta S. JagtapDocument2 pages4357 - 22.Dr - Ravindra B. Gunale1 DR - Prajakta S. Jagtap21 RakshitNo ratings yet
- Estudio SEDCOMDocument11 pagesEstudio SEDCOMElias Vera RojasNo ratings yet
- Trial CardDocument4 pagesTrial CardMM&MNo ratings yet
- Spritual Health Life: 1. Gyan Mudra (Mudra of Knowledge)Document10 pagesSpritual Health Life: 1. Gyan Mudra (Mudra of Knowledge)chachu123100% (2)
- Jurnal Non Sirotic VEDocument21 pagesJurnal Non Sirotic VEDheajeng Intan MutiarasariNo ratings yet
- AgendaDocument33 pagesAgendaPrateek Taneja0% (1)
- Concept Map MgenoviaDocument5 pagesConcept Map Mgenoviaapi-302138606No ratings yet
- I PSF Abstract Book 15Document107 pagesI PSF Abstract Book 15Trần HiềnNo ratings yet
- UW-5 Omeng0000Document58 pagesUW-5 Omeng0000Guillermo Jesus Avila ArrietaNo ratings yet
- Curios BehaviorDocument282 pagesCurios BehaviorroxyoanceaNo ratings yet
- Turmeric Cream Mask B16 Edison G1Document25 pagesTurmeric Cream Mask B16 Edison G1Lance HeindrickNo ratings yet
- Reconnective Healing: Beyond IntentionDocument2 pagesReconnective Healing: Beyond IntentionBentiv50% (2)
- Squirting What You Need To Know... and MoreDocument9 pagesSquirting What You Need To Know... and MoreFarid Hamidou0% (1)
- 2570-6541-1-SM (Tugas Mbak Bekti)Document12 pages2570-6541-1-SM (Tugas Mbak Bekti)Fadillah NurNo ratings yet
- 2.physiology of Salivary Secretion 3Document27 pages2.physiology of Salivary Secretion 3AFNAD 123No ratings yet
- 2020-10-16 Memorandum in Support of CVS Motion To DismissDocument28 pages2020-10-16 Memorandum in Support of CVS Motion To DismissNewsChannel 9 StaffNo ratings yet