Download as pdf or txt
You might also like
- Tavi 150923155743 Lva1 App6892Document157 pagesTavi 150923155743 Lva1 App6892Zhivka Kostadinova100% (1)
- Service-manual-SG Emachines E725 E525 031809Document236 pagesService-manual-SG Emachines E725 E525 031809andhrimnirNo ratings yet
- Norsok M 121 AluminiumDocument17 pagesNorsok M 121 Aluminiumale_f_79No ratings yet
- F5 Exam P2 QuestionsDocument5 pagesF5 Exam P2 QuestionsTrevor G. Samaroo100% (3)
- Ivc FilterDocument15 pagesIvc FilterashishNo ratings yet
- Cut Down Access To Avoid Vascular Complications During Transcatheter Aortic Valve ImplantationDocument9 pagesCut Down Access To Avoid Vascular Complications During Transcatheter Aortic Valve ImplantationAthenaeum Scientific PublishersNo ratings yet
- Inferior Vena Cava Filter GuidelineDocument5 pagesInferior Vena Cava Filter GuidelineAndika ResaNo ratings yet
- Vein - 2009 Sir - Ivcf ReviewDocument9 pagesVein - 2009 Sir - Ivcf Reviewjohn_smith_532No ratings yet
- Why When and HowDocument11 pagesWhy When and Howamrit koiralaNo ratings yet
- FundusDocument6 pagesFunduslong hoàngNo ratings yet
- CQE11 Patient Care Safety Access Maintaining 0Document42 pagesCQE11 Patient Care Safety Access Maintaining 0Srinivas KoudaganiNo ratings yet
- Focus: Real-Time Ultrasound-Guided External Ventricular Drain Placement: Technical NoteDocument5 pagesFocus: Real-Time Ultrasound-Guided External Ventricular Drain Placement: Technical NoteOdiet RevenderNo ratings yet
- Pda Ev Ejtcs 04Document7 pagesPda Ev Ejtcs 04emmanuel le bretNo ratings yet
- S0090429521002594Document7 pagesS0090429521002594Mounia MarsouNo ratings yet
- Post Aua ReconstructivaDocument14 pagesPost Aua ReconstructivaIndhira Sierra SanchezNo ratings yet
- 6 ST1312-011Document12 pages6 ST1312-011Blink TdmNo ratings yet
- 1 s2.0 S1879522615003929 MainDocument4 pages1 s2.0 S1879522615003929 MainsagaNo ratings yet
- Article AVI in UKDocument10 pagesArticle AVI in UKFaddy OrahaNo ratings yet
- The Surgical Bilio-Digestive Bypass Before Cephalic Pancreaticoduodenectomy, Report of Eight CasesDocument4 pagesThe Surgical Bilio-Digestive Bypass Before Cephalic Pancreaticoduodenectomy, Report of Eight CasesIJAR JOURNALNo ratings yet
- Central Venous Catheter Removal: Procedures and Rationale: LinicalDocument9 pagesCentral Venous Catheter Removal: Procedures and Rationale: LinicalVendiNo ratings yet
- Fraktur FrakDocument11 pagesFraktur FrakRirin SeptianiNo ratings yet
- Continuous Ambulatory Peritoneal Dialysis Catheter Placement Is Omentectomy Necessary 2016Document3 pagesContinuous Ambulatory Peritoneal Dialysis Catheter Placement Is Omentectomy Necessary 2016waldemar russellNo ratings yet
- J Vet Emergen Crit Care - 2022 - Jones - Comparison of Success Rate and Time To Obtain Venous Cannulation by CutdownDocument9 pagesJ Vet Emergen Crit Care - 2022 - Jones - Comparison of Success Rate and Time To Obtain Venous Cannulation by CutdownAdriana PalmaNo ratings yet
- 1 s2.0 S0929664615003514 MainDocument8 pages1 s2.0 S0929664615003514 MainMutiana SafitriNo ratings yet
- Ivc Filter RetrievalDocument8 pagesIvc Filter RetrievalMostafaNo ratings yet
- How To Do Aorta InterventionDocument80 pagesHow To Do Aorta InterventionMohamad ZulfikarNo ratings yet
- Is It Safe and Practical To Use A Foley Catheter As A Chest Tube For Lung Cancer Patients After Lobectomy? A Prospective Cohort Study With 441 CasesDocument6 pagesIs It Safe and Practical To Use A Foley Catheter As A Chest Tube For Lung Cancer Patients After Lobectomy? A Prospective Cohort Study With 441 CasesRayCassidyNo ratings yet
- 10 1093icvtsivy076Document9 pages10 1093icvtsivy076mukhlis akmalNo ratings yet
- HAI bUNDLESDocument54 pagesHAI bUNDLESNurhayati100% (1)
- Ventriculoperitoneal ShuntDocument5 pagesVentriculoperitoneal ShunttameemNo ratings yet
- Clinical Guideline: Umbilical Venous Catheter InsertionDocument14 pagesClinical Guideline: Umbilical Venous Catheter InsertionCrisu AlexandraNo ratings yet
- Ezae 127Document9 pagesEzae 127aimanshahnaz285No ratings yet
- Millington 2018Document18 pagesMillington 2018RositaMagda MataNo ratings yet
- J Euros 2021 06 010Document6 pagesJ Euros 2021 06 010Maita LojoNo ratings yet
- Casali 2009Document6 pagesCasali 2009Giancarlo Maruri MunarettoNo ratings yet
- Embedded Inferior Vena Cava Filter RemovalDocument20 pagesEmbedded Inferior Vena Cava Filter RemovalsirrfsNo ratings yet
- Pdi 34 2 010Document8 pagesPdi 34 2 010Ricardo IbarraNo ratings yet
- Guidelines For Peritoneal Dialysis Access: Perotial CathetersDocument7 pagesGuidelines For Peritoneal Dialysis Access: Perotial CathetersSahily MoralesNo ratings yet
- Eortc 22911Document7 pagesEortc 22911yingming zhuNo ratings yet
- VSD Ventricular Septal Defect RepairDocument31 pagesVSD Ventricular Septal Defect RepairRedmond P. Burke MD100% (8)
- The Clinical Outcomes of Endovenous Microwave and Laser Ablation For Varicose VeinsDocument6 pagesThe Clinical Outcomes of Endovenous Microwave and Laser Ablation For Varicose VeinsMalekseuofi مالك السيوفيNo ratings yet
- 1 s2.0 S0039606020306759 MainDocument9 pages1 s2.0 S0039606020306759 MainKar RodriguezNo ratings yet
- Reoperative Mitral Valve Replacement: Importance of Preservation of The Subvalvular ApparatusDocument6 pagesReoperative Mitral Valve Replacement: Importance of Preservation of The Subvalvular ApparatusThanh BinhNo ratings yet
- A Comparative Study of Complic PDFDocument6 pagesA Comparative Study of Complic PDFBeatrice TanudjajaNo ratings yet
- Journal Pre-Proof: Journal of The American College of SurgeonsDocument28 pagesJournal Pre-Proof: Journal of The American College of SurgeonsIvory June CadeteNo ratings yet
- Anterior Resection With Low AnastomosisDocument10 pagesAnterior Resection With Low AnastomosisOhana S.No ratings yet
- VSRR Ezaa083Document8 pagesVSRR Ezaa083NikhilNo ratings yet
- Cauti Prevention Qi SlidesDocument8 pagesCauti Prevention Qi Slidesapi-596656815No ratings yet
- Bjs 109 Suppl 5 IssueDocument151 pagesBjs 109 Suppl 5 IssueJENIFER KARINA PUTZ LORENZINo ratings yet
- VaricocelectomyDocument10 pagesVaricocelectomyugd armyNo ratings yet
- FCVM 09 750896Document10 pagesFCVM 09 750896S Ram KishoreNo ratings yet
- Partial Breast Irradiation: Dawn Radsek, RN Froedtert Hospital 9200 W Wisconsin Ave Milwaukee, WI 414/805-4440Document72 pagesPartial Breast Irradiation: Dawn Radsek, RN Froedtert Hospital 9200 W Wisconsin Ave Milwaukee, WI 414/805-4440Arun KUMAR.NNo ratings yet
- Bladder InjuryDocument7 pagesBladder InjurycorsaruNo ratings yet
- Ultrasound Guided Percutaneous DrainageDocument3 pagesUltrasound Guided Percutaneous DrainageLaraib Fatima0% (1)
- Quality Guidelines IVC FilterDocument9 pagesQuality Guidelines IVC Filteramrit koiralaNo ratings yet
- Percutaneous Nephrostomy: Last Updated: January 3, 2003Document5 pagesPercutaneous Nephrostomy: Last Updated: January 3, 2003Alicia EncinasNo ratings yet
- Modified 2 CM Super Single Port vs. The Traditional 3 CM Single Port For Video Assisted Thoracoscopic Surgery LobectomyDocument8 pagesModified 2 CM Super Single Port vs. The Traditional 3 CM Single Port For Video Assisted Thoracoscopic Surgery LobectomyAlin Ionut BurlacuNo ratings yet
- World Journal of Clinical Surgery: Open AccessDocument6 pagesWorld Journal of Clinical Surgery: Open AccessWorld Journal of Clinical SurgeryNo ratings yet
- Adrenalectomy LapDocument7 pagesAdrenalectomy LapTJ LapuzNo ratings yet
- Repair CDLDocument6 pagesRepair CDLYuliastuti Mamah ChelseaNo ratings yet
- A Novel Technique For Treatment of Distal Ureteral Calculi: Early ResultsDocument4 pagesA Novel Technique For Treatment of Distal Ureteral Calculi: Early ResultsTheQueensafa90No ratings yet
- Jkms 25 1748Document6 pagesJkms 25 1748NELLY VAZQUEZ FLORESNo ratings yet
- Keys to Successful Orthotopic Bladder SubstitutionFrom EverandKeys to Successful Orthotopic Bladder SubstitutionUrs E. StuderNo ratings yet
- OMB BALL ValveDocument44 pagesOMB BALL Valveale_f_79No ratings yet
- Natural Gas Product SpecificationsDocument4 pagesNatural Gas Product Specificationsale_f_79No ratings yet
- Pip Mec FunDocument24 pagesPip Mec Funale_f_79No ratings yet
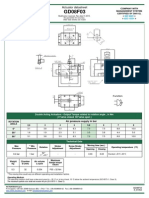
- GD0008F03Document1 pageGD0008F03ale_f_79No ratings yet
- Installation Guide Ansys 14.5Document71 pagesInstallation Guide Ansys 14.5ale_f_79No ratings yet
- Ansys 14.5 For Win Installation GuideDocument71 pagesAnsys 14.5 For Win Installation Guideale_f_79No ratings yet
- 0810 Operation Manual250708Document117 pages0810 Operation Manual250708isaacaiyacNo ratings yet
- Geothermal Well Operation and Maintenance: Sverrir ThorhallssonDocument23 pagesGeothermal Well Operation and Maintenance: Sverrir ThorhallssonLaras PutiNo ratings yet
- Electronic Reservation Slip IRCTC E-Ticketing Service (Agent)Document2 pagesElectronic Reservation Slip IRCTC E-Ticketing Service (Agent)Prashant PatilNo ratings yet
- Contribution of Medieval MuslimDocument16 pagesContribution of Medieval Muslimannur osmanNo ratings yet
- DLL For GenMath - Q1, W3EDocument3 pagesDLL For GenMath - Q1, W3EJigz Vasquez100% (4)
- Pinoy Development of Groups and TeamsDocument19 pagesPinoy Development of Groups and TeamsSarah Jane SeñaNo ratings yet
- EF4e Intplus Filetest 3bDocument7 pagesEF4e Intplus Filetest 3bjeanneramazanovaNo ratings yet
- WH2009 WaterHorseCatalogDocument132 pagesWH2009 WaterHorseCatalogAiko FeroNo ratings yet
- DBA ResumeDocument5 pagesDBA ResumeBheema ReddyNo ratings yet
- Applied Economics Module 3 Q1Document21 pagesApplied Economics Module 3 Q1Jefferson Del Rosario100% (1)
- From Rice To Apple-Pear Style - An Ecocritical Approach To China's Korean Ethnic MinorityDocument14 pagesFrom Rice To Apple-Pear Style - An Ecocritical Approach To China's Korean Ethnic MinorityLing LIUNo ratings yet
- Comparative Study of Soil Structure Interaction Analysis of Building On Clayey and Sandy Soil-IJRASETDocument11 pagesComparative Study of Soil Structure Interaction Analysis of Building On Clayey and Sandy Soil-IJRASETIJRASETPublicationsNo ratings yet
- Database Systems, Eleventh Edition by Coronel Morris, Course Technology 2014Document5 pagesDatabase Systems, Eleventh Edition by Coronel Morris, Course Technology 2014LaluMohan KcNo ratings yet
- Astaro Security Gateway enDocument4 pagesAstaro Security Gateway enmaxbyzNo ratings yet
- Tc3yf en Manual 170905 He PDFDocument1 pageTc3yf en Manual 170905 He PDFJuan Manuel EscorihuelaNo ratings yet
- NikeDocument3 pagesNikeAadnya UjagareNo ratings yet
- Nunez v. Sec - y of HHS - 2019 U.S. Claims LEXIS 644Document40 pagesNunez v. Sec - y of HHS - 2019 U.S. Claims LEXIS 644Kirk HartleyNo ratings yet
- LG W1943C Chass LM92C PDFDocument23 pagesLG W1943C Chass LM92C PDFDaniel Paguay100% (1)
- Deed in LieuDocument33 pagesDeed in LieuSteven WhitfordNo ratings yet
- Haunted: MuseumDocument36 pagesHaunted: MuseumNgoc PhanNo ratings yet
- Karens A-MDocument21 pagesKarens A-Mapi-291270075No ratings yet
- Exp 7 Colloids ChemistryDocument8 pagesExp 7 Colloids ChemistryNur Fadhilah100% (1)
- Lexico and GrammarDocument7 pagesLexico and Grammarphammaiphuong2k9No ratings yet
- Fast Food Waiting TimeDocument32 pagesFast Food Waiting TimebossdudeNo ratings yet
- Canadian Soil Quality Guidelines For The Protection of Environmental and Human Health Uranium 2007Document14 pagesCanadian Soil Quality Guidelines For The Protection of Environmental and Human Health Uranium 2007njcojann_co901745No ratings yet
- Magic SquaresDocument1 pageMagic SquaresplmokmNo ratings yet
- Impromptu SpeechDocument25 pagesImpromptu SpeechJerome Bulaun100% (1)
- Join The Club: C207 - Database Systems 2012Document237 pagesJoin The Club: C207 - Database Systems 2012hamzahNo ratings yet