
Humphry
Humphry
You might also like
- EPIC Access From HomeDocument4 pagesEPIC Access From Homescribd4kmh100% (1)
- Stahl RX Swtiching Guide PDFDocument148 pagesStahl RX Swtiching Guide PDFscribd4kmh100% (4)
- Bio LabsDocument40 pagesBio LabsP NielsenNo ratings yet
- Project Traveller Arrest DetailsDocument7 pagesProject Traveller Arrest DetailsCynthiaMcLeodSunNo ratings yet
- Toxic Secrets - Fluoride PDFDocument15 pagesToxic Secrets - Fluoride PDFRorajma1100% (1)
- EPIC Access From Home PDFDocument4 pagesEPIC Access From Home PDFscribd4kmhNo ratings yet
- Bobath ApproachDocument22 pagesBobath ApproachCedricFernandez50% (4)
- 1490823659-Ch. 4 GA Story BibleDocument19 pages1490823659-Ch. 4 GA Story BibleKorry ShepardNo ratings yet
- Paper 1 Oprah Winfreys School For GirlsDocument4 pagesPaper 1 Oprah Winfreys School For Girlsapi-535571700No ratings yet
- Health Hazards of Chemicals Commonly Used On Military BasesDocument35 pagesHealth Hazards of Chemicals Commonly Used On Military Basesmale nurseNo ratings yet
- L O D M. B: AW Ffices of Arius ArazandehDocument4 pagesL O D M. B: AW Ffices of Arius ArazandehmichaelNo ratings yet
- To United Nations AgainDocument19 pagesTo United Nations AgainFrank GallagherNo ratings yet
- European Adoption Consultants Sued For Money Damages by Ohio Attorney General June 1st, 2017 18-Pagesy Damages OnlyDocument19 pagesEuropean Adoption Consultants Sued For Money Damages by Ohio Attorney General June 1st, 2017 18-Pagesy Damages OnlyHarry the GreekNo ratings yet
- We're All Lab Rats in The Government's Secret ExperimentsDocument7 pagesWe're All Lab Rats in The Government's Secret Experimentsivan a gargurevichNo ratings yet
- CREW: Department of Defense: Central Intelligence Agency: Regarding NSA Reporting Requirements: Cover LetterDocument3 pagesCREW: Department of Defense: Central Intelligence Agency: Regarding NSA Reporting Requirements: Cover LetterCREWNo ratings yet
- To Kill A Tree: Part FourDocument10 pagesTo Kill A Tree: Part FourPhilip John Jones100% (2)
- Trump To Declassify Documents Relating To Russia Investigation, Carter Page FISA Warrant - CNNPoliticsDocument2 pagesTrump To Declassify Documents Relating To Russia Investigation, Carter Page FISA Warrant - CNNPoliticsMY PROFILENo ratings yet
- The Hill Ran A False "Confederate Statues" Headline On Her SpeechDocument4 pagesThe Hill Ran A False "Confederate Statues" Headline On Her SpeechAnonymous Qn8AvWvx0% (1)
- 391 - Guilty As Charged! - From ITCCS!Document2 pages391 - Guilty As Charged! - From ITCCS!gerald_382046427No ratings yet
- Hoffer 1962Document65 pagesHoffer 1962adamNo ratings yet
- Osmond 1957Document17 pagesOsmond 1957Gonzalo BimonteNo ratings yet
- D&A: 05012016 Declaration Natalia VeselnitskayaDocument4 pagesD&A: 05012016 Declaration Natalia VeselnitskayaD&A Investigations, Inc.No ratings yet
- The Needle and The Damage Done. Martin P. Keerns. (2013) PDFDocument1,111 pagesThe Needle and The Damage Done. Martin P. Keerns. (2013) PDFilyes zambakto100% (1)
- Bush Exec Order 13470 30jul08Document40 pagesBush Exec Order 13470 30jul08Guy RazerNo ratings yet
- Waterboarding ArticleDocument28 pagesWaterboarding ArticleGlennKesslerWPNo ratings yet
- Ferdinand Edralin Marcos Documents and Videos Compilation: December 18 at 11:27amDocument5 pagesFerdinand Edralin Marcos Documents and Videos Compilation: December 18 at 11:27amCONCORDIO E. JABAGAT SR.No ratings yet
- Promis, Main Core DocumentationDocument11 pagesPromis, Main Core DocumentationDAVID M .DASTYCHNo ratings yet
- Dr. Peter BeterDocument3 pagesDr. Peter BeterŽubori PotokNo ratings yet
- NH Foia James OkeefeDocument6 pagesNH Foia James OkeefejchristianadamsNo ratings yet
- States V Us and States Compl 2021-11-23 WITH EXHIBITSDocument1,230 pagesStates V Us and States Compl 2021-11-23 WITH EXHIBITSPete SantilliNo ratings yet
- Adrenochrome - C9H9NO3 - PubChemDocument22 pagesAdrenochrome - C9H9NO3 - PubChemMatías PierottiNo ratings yet
- D&A: 23012017 The Barack Obama, Joe Biden Scheme To Entrap General FlynnDocument4 pagesD&A: 23012017 The Barack Obama, Joe Biden Scheme To Entrap General FlynnD&A Investigations, Inc.No ratings yet
- H1N1-Journalist Files Charges - 2Document4 pagesH1N1-Journalist Files Charges - 2RedzaNo ratings yet
- Declassified Horowitz FootnotesDocument5 pagesDeclassified Horowitz FootnotesAndy BeltNo ratings yet
- PodestaFiles PDFDocument8 pagesPodestaFiles PDFAndrow George Makram100% (1)
- WISCONSIN VOTERS ALLIANCE V PENCEDocument7 pagesWISCONSIN VOTERS ALLIANCE V PENCERawStoryNo ratings yet
- Establishment of One New World OrderDocument9 pagesEstablishment of One New World OrderGuy Razer100% (1)
- State Department Release of Emails Between Huma Abedine and Hillary Clinton Emails 2-2-2018Document137 pagesState Department Release of Emails Between Huma Abedine and Hillary Clinton Emails 2-2-2018Beverly TranNo ratings yet
- Joe Biden: Jump To Navigation Jump To SearchDocument77 pagesJoe Biden: Jump To Navigation Jump To Searchjason7sean-30030No ratings yet
- Report of Investigation: Recovery of Text Messages From Certain FBI Mobile DevicesDocument16 pagesReport of Investigation: Recovery of Text Messages From Certain FBI Mobile DevicesScott Johnson100% (1)
- Request For Declassification and Publication of Intelligence Community Assessment On COVID19 ORIGINSDocument2 pagesRequest For Declassification and Publication of Intelligence Community Assessment On COVID19 ORIGINSEmanuel McCrayNo ratings yet
- Fast Furious Report Part 1Document211 pagesFast Furious Report Part 1dcodreaNo ratings yet
- Eleven-Page Journal Entry in W. MI U. Vaccine Mandate Case Dated Oct. 7th, 2021Document11 pagesEleven-Page Journal Entry in W. MI U. Vaccine Mandate Case Dated Oct. 7th, 2021Harry the Greek100% (1)
- Bioweapon AttackDocument3 pagesBioweapon Attackta84288No ratings yet
- International: Documents Reveal Top NSA Hacking UnitDocument4 pagesInternational: Documents Reveal Top NSA Hacking UnitEb OlaNo ratings yet
- #Karenhudes Karen Hudes Jesuit Vatican Gold #Chemtrails #Geoengineering PDFDocument20 pages#Karenhudes Karen Hudes Jesuit Vatican Gold #Chemtrails #Geoengineering PDFsisterrosettaNo ratings yet
- "Obama Worse Than Bush", David R. HoffmanDocument5 pages"Obama Worse Than Bush", David R. HoffmanGiuliano ValverdeNo ratings yet
- ( ( (Media) ) ) Inflates Common Cold To Trash US ConstitutionDocument6 pages( ( (Media) ) ) Inflates Common Cold To Trash US ConstitutiongqqhqNo ratings yet
- Northwoods and Garden Plot PDFDocument58 pagesNorthwoods and Garden Plot PDFthierryNo ratings yet
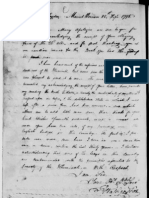
- George Washington Letter On Dangers of Illuminati 25 Sep 1798Document5 pagesGeorge Washington Letter On Dangers of Illuminati 25 Sep 1798Mick RynningNo ratings yet
- Executive Order 12148Document9 pagesExecutive Order 12148Jeremy Green100% (1)
- Pfizer Under 17 Years Adverse Events Reported To CDCDocument149 pagesPfizer Under 17 Years Adverse Events Reported To CDCWilliam BanksNo ratings yet
- Evidence Swine FluDocument10 pagesEvidence Swine FluThorsteinn Thorsteinsson100% (1)
- Pentagon Papers Part IV B 3Document177 pagesPentagon Papers Part IV B 3KidNo ratings yet
- U S D C D C: Ontgomery Lair IbleyDocument27 pagesU S D C D C: Ontgomery Lair IbleyLartoonNo ratings yet
- CIA's Support To The Nazi War Criminal InvestigationsDocument8 pagesCIA's Support To The Nazi War Criminal InvestigationsThe Baked CatNo ratings yet
- A Journey In Other Worlds: A Romance of the FutureFrom EverandA Journey In Other Worlds: A Romance of the FutureRating: 2.5 out of 5 stars2.5/5 (12)
- Summary of Judy Mikovits & Kent Heckenlively's Plague of CorruptionFrom EverandSummary of Judy Mikovits & Kent Heckenlively's Plague of CorruptionNo ratings yet
- The TI Program: A Multi-Trillion Dollar Plot for Global Domination?: 1A, #1From EverandThe TI Program: A Multi-Trillion Dollar Plot for Global Domination?: 1A, #1No ratings yet
- Public Response Dispatcher DetailsDocument11 pagesPublic Response Dispatcher Detailsscribd4kmhNo ratings yet
- 2022 COVID 19 SPSL PosterDocument1 page2022 COVID 19 SPSL Posterscribd4kmhNo ratings yet
- (Cliff Notes) 1984Document47 pages(Cliff Notes) 1984scribd4kmhNo ratings yet
- Data Overview - CITY CARRIER ASSISTANT - NORTH HOLLYWOOD CA NC10784723Document4 pagesData Overview - CITY CARRIER ASSISTANT - NORTH HOLLYWOOD CA NC10784723scribd4kmhNo ratings yet
- Change Lives by Building: Better Systems of CareDocument6 pagesChange Lives by Building: Better Systems of Carescribd4kmhNo ratings yet
- Examinee Guide: POST Entry-Level Dispatcher Selection Test BatteryDocument9 pagesExaminee Guide: POST Entry-Level Dispatcher Selection Test Batteryscribd4kmhNo ratings yet
- 10yr F-U Psychosis - 2017-World - PsychiatryDocument3 pages10yr F-U Psychosis - 2017-World - Psychiatryscribd4kmhNo ratings yet
- Application For Temporary Smog Exemption For A Vehicle Located Out-Of-StateDocument1 pageApplication For Temporary Smog Exemption For A Vehicle Located Out-Of-Statescribd4kmhNo ratings yet
- Position StatementDocument6 pagesPosition Statementscribd4kmhNo ratings yet
- 4 False PremisesDocument30 pages4 False Premisesscribd4kmhNo ratings yet
- Abbass Royal College 2005 PDFDocument3 pagesAbbass Royal College 2005 PDFscribd4kmhNo ratings yet
- Jse 16 2Document166 pagesJse 16 2scribd4kmhNo ratings yet
- Short-Term Psychodynamic Psychotherapy For Somatic DisordersDocument10 pagesShort-Term Psychodynamic Psychotherapy For Somatic Disordersscribd4kmhNo ratings yet
- 05 Szasz and TorreyDocument14 pages05 Szasz and Torreyscribd4kmhNo ratings yet
- Express Checkout: Check Out Time Is 11:00 AmDocument1 pageExpress Checkout: Check Out Time Is 11:00 Amscribd4kmhNo ratings yet
- Amer Peds Recomm Re Psy Drugs and PregnancyDocument10 pagesAmer Peds Recomm Re Psy Drugs and Pregnancyscribd4kmhNo ratings yet
- Rschgate Psychoisi TX W TherDocument11 pagesRschgate Psychoisi TX W Therscribd4kmhNo ratings yet
- Somatization: Diagnosing It Sooner Through Emotion-Focused InterviewingDocument10 pagesSomatization: Diagnosing It Sooner Through Emotion-Focused Interviewingscribd4kmhNo ratings yet
- Instructions For Completing Inf 70 Request For Record InformationDocument5 pagesInstructions For Completing Inf 70 Request For Record Informationscribd4kmhNo ratings yet
- DR Childress Communicating With ChildrenDocument1 pageDR Childress Communicating With Childrenscribd4kmhNo ratings yet
- DR Childress Family TherapyDocument2 pagesDR Childress Family Therapyscribd4kmhNo ratings yet
- Form WHO Dewasa PDFDocument2 pagesForm WHO Dewasa PDFAbizar Agung WibawaNo ratings yet
- VastarelDocument20 pagesVastarelKristen FieldsNo ratings yet
- The Seasonal Health Questionnaire Is More EffectiveDocument2 pagesThe Seasonal Health Questionnaire Is More EffectiveMaíra DiasNo ratings yet
- Nursing Care PlansDocument31 pagesNursing Care PlansCyril Jane Caanyagan AcutNo ratings yet
- Trigeminal NeuralgiaDocument72 pagesTrigeminal NeuralgiaCocoMathewNo ratings yet
- Hints For Remembering Medication ClassificationsDocument2 pagesHints For Remembering Medication ClassificationsSarah SNo ratings yet
- نسخة 264889196 Tramadol Drug StudyDocument1 pageنسخة 264889196 Tramadol Drug StudyMeteab AlzhiryNo ratings yet
- Presented By: Lady Diane Cabriga Bsn-IiiDocument11 pagesPresented By: Lady Diane Cabriga Bsn-IiiDayan CabrigaNo ratings yet
- SickLeaveCertificate With and Without Diagnosis 20230717 154636Document2 pagesSickLeaveCertificate With and Without Diagnosis 20230717 154636rishibarathiNo ratings yet
- Reflective Functioning ManualDocument47 pagesReflective Functioning ManualAntonio Tejero PocielloNo ratings yet
- Cause and Effect ParagraphsDocument14 pagesCause and Effect ParagraphsJosue Nádasdy Borthwick50% (2)
- UrticariaDocument52 pagesUrticariappica8111No ratings yet
- The Good Indicators Guide:: Understanding How To Use and Choose IndicatorsDocument40 pagesThe Good Indicators Guide:: Understanding How To Use and Choose IndicatorssuperpaqsNo ratings yet
- Presented By: Ashlee Barbeau Student Occupational Therapist, Queen's UniversityDocument22 pagesPresented By: Ashlee Barbeau Student Occupational Therapist, Queen's UniversityDanielle Stella N'LucaNo ratings yet
- Lingualised Occ RevisitedDocument5 pagesLingualised Occ RevisitedDrPrachi AgrawalNo ratings yet
- Liver Cirrhosis PDFDocument9 pagesLiver Cirrhosis PDFDennis CobbNo ratings yet
- 6Cs in Social Care GuideDocument4 pages6Cs in Social Care GuideLoo DrBradNo ratings yet
- Dizziness - PPPD Information SheetDocument8 pagesDizziness - PPPD Information Sheettan_siqi100% (1)
- Assessment of Pain in ChildrenDocument30 pagesAssessment of Pain in ChildrenVlad AlexandraNo ratings yet
- Role of Double J Stenting After Uncomplicated Ureterorenoscopy For 1 Centimeter Ureteral Stones: A Randomised Control TrialDocument3 pagesRole of Double J Stenting After Uncomplicated Ureterorenoscopy For 1 Centimeter Ureteral Stones: A Randomised Control TrialAnonymous izrFWiQNo ratings yet
- Palatal InjectionDocument10 pagesPalatal InjectionJose Salas AdragnaNo ratings yet
- Cambridge English For Nursing Grammar Practice Pre Intermediate Unit6Document3 pagesCambridge English For Nursing Grammar Practice Pre Intermediate Unit6Jorge CampiNo ratings yet
- Laboratory Services in HospitalDocument58 pagesLaboratory Services in HospitalDr. Rakshit SolankiNo ratings yet
- ARB and CCB CombinationDocument11 pagesARB and CCB CombinationLucky PratamaNo ratings yet
- CEBM Levels of EvidenceDocument2 pagesCEBM Levels of Evidence2012100% (2)
- Advanced Practice Nursing in The Philippines: Are We There Yet?Document5 pagesAdvanced Practice Nursing in The Philippines: Are We There Yet?Alex LavadiaNo ratings yet
- DMPC CoeDocument1 pageDMPC CoeJulius Magaru RaquelNo ratings yet
- Leg UlcersDocument22 pagesLeg UlcersMarera DomnicNo ratings yet













































































































Download as pdf or txt
You might also like
- EPIC Access From HomeDocument4 pagesEPIC Access From Homescribd4kmh100% (1)
- Stahl RX Swtiching Guide PDFDocument148 pagesStahl RX Swtiching Guide PDFscribd4kmh100% (4)
- Bio LabsDocument40 pagesBio LabsP NielsenNo ratings yet
- Project Traveller Arrest DetailsDocument7 pagesProject Traveller Arrest DetailsCynthiaMcLeodSunNo ratings yet
- Toxic Secrets - Fluoride PDFDocument15 pagesToxic Secrets - Fluoride PDFRorajma1100% (1)
- EPIC Access From Home PDFDocument4 pagesEPIC Access From Home PDFscribd4kmhNo ratings yet
- Bobath ApproachDocument22 pagesBobath ApproachCedricFernandez50% (4)
- 1490823659-Ch. 4 GA Story BibleDocument19 pages1490823659-Ch. 4 GA Story BibleKorry ShepardNo ratings yet
- Paper 1 Oprah Winfreys School For GirlsDocument4 pagesPaper 1 Oprah Winfreys School For Girlsapi-535571700No ratings yet
- Health Hazards of Chemicals Commonly Used On Military BasesDocument35 pagesHealth Hazards of Chemicals Commonly Used On Military Basesmale nurseNo ratings yet
- L O D M. B: AW Ffices of Arius ArazandehDocument4 pagesL O D M. B: AW Ffices of Arius ArazandehmichaelNo ratings yet
- To United Nations AgainDocument19 pagesTo United Nations AgainFrank GallagherNo ratings yet
- European Adoption Consultants Sued For Money Damages by Ohio Attorney General June 1st, 2017 18-Pagesy Damages OnlyDocument19 pagesEuropean Adoption Consultants Sued For Money Damages by Ohio Attorney General June 1st, 2017 18-Pagesy Damages OnlyHarry the GreekNo ratings yet
- We're All Lab Rats in The Government's Secret ExperimentsDocument7 pagesWe're All Lab Rats in The Government's Secret Experimentsivan a gargurevichNo ratings yet
- CREW: Department of Defense: Central Intelligence Agency: Regarding NSA Reporting Requirements: Cover LetterDocument3 pagesCREW: Department of Defense: Central Intelligence Agency: Regarding NSA Reporting Requirements: Cover LetterCREWNo ratings yet
- To Kill A Tree: Part FourDocument10 pagesTo Kill A Tree: Part FourPhilip John Jones100% (2)
- Trump To Declassify Documents Relating To Russia Investigation, Carter Page FISA Warrant - CNNPoliticsDocument2 pagesTrump To Declassify Documents Relating To Russia Investigation, Carter Page FISA Warrant - CNNPoliticsMY PROFILENo ratings yet
- The Hill Ran A False "Confederate Statues" Headline On Her SpeechDocument4 pagesThe Hill Ran A False "Confederate Statues" Headline On Her SpeechAnonymous Qn8AvWvx0% (1)
- 391 - Guilty As Charged! - From ITCCS!Document2 pages391 - Guilty As Charged! - From ITCCS!gerald_382046427No ratings yet
- Hoffer 1962Document65 pagesHoffer 1962adamNo ratings yet
- Osmond 1957Document17 pagesOsmond 1957Gonzalo BimonteNo ratings yet
- D&A: 05012016 Declaration Natalia VeselnitskayaDocument4 pagesD&A: 05012016 Declaration Natalia VeselnitskayaD&A Investigations, Inc.No ratings yet
- The Needle and The Damage Done. Martin P. Keerns. (2013) PDFDocument1,111 pagesThe Needle and The Damage Done. Martin P. Keerns. (2013) PDFilyes zambakto100% (1)
- Bush Exec Order 13470 30jul08Document40 pagesBush Exec Order 13470 30jul08Guy RazerNo ratings yet
- Waterboarding ArticleDocument28 pagesWaterboarding ArticleGlennKesslerWPNo ratings yet
- Ferdinand Edralin Marcos Documents and Videos Compilation: December 18 at 11:27amDocument5 pagesFerdinand Edralin Marcos Documents and Videos Compilation: December 18 at 11:27amCONCORDIO E. JABAGAT SR.No ratings yet
- Promis, Main Core DocumentationDocument11 pagesPromis, Main Core DocumentationDAVID M .DASTYCHNo ratings yet
- Dr. Peter BeterDocument3 pagesDr. Peter BeterŽubori PotokNo ratings yet
- NH Foia James OkeefeDocument6 pagesNH Foia James OkeefejchristianadamsNo ratings yet
- States V Us and States Compl 2021-11-23 WITH EXHIBITSDocument1,230 pagesStates V Us and States Compl 2021-11-23 WITH EXHIBITSPete SantilliNo ratings yet
- Adrenochrome - C9H9NO3 - PubChemDocument22 pagesAdrenochrome - C9H9NO3 - PubChemMatías PierottiNo ratings yet
- D&A: 23012017 The Barack Obama, Joe Biden Scheme To Entrap General FlynnDocument4 pagesD&A: 23012017 The Barack Obama, Joe Biden Scheme To Entrap General FlynnD&A Investigations, Inc.No ratings yet
- H1N1-Journalist Files Charges - 2Document4 pagesH1N1-Journalist Files Charges - 2RedzaNo ratings yet
- Declassified Horowitz FootnotesDocument5 pagesDeclassified Horowitz FootnotesAndy BeltNo ratings yet
- PodestaFiles PDFDocument8 pagesPodestaFiles PDFAndrow George Makram100% (1)
- WISCONSIN VOTERS ALLIANCE V PENCEDocument7 pagesWISCONSIN VOTERS ALLIANCE V PENCERawStoryNo ratings yet
- Establishment of One New World OrderDocument9 pagesEstablishment of One New World OrderGuy Razer100% (1)
- State Department Release of Emails Between Huma Abedine and Hillary Clinton Emails 2-2-2018Document137 pagesState Department Release of Emails Between Huma Abedine and Hillary Clinton Emails 2-2-2018Beverly TranNo ratings yet
- Joe Biden: Jump To Navigation Jump To SearchDocument77 pagesJoe Biden: Jump To Navigation Jump To Searchjason7sean-30030No ratings yet
- Report of Investigation: Recovery of Text Messages From Certain FBI Mobile DevicesDocument16 pagesReport of Investigation: Recovery of Text Messages From Certain FBI Mobile DevicesScott Johnson100% (1)
- Request For Declassification and Publication of Intelligence Community Assessment On COVID19 ORIGINSDocument2 pagesRequest For Declassification and Publication of Intelligence Community Assessment On COVID19 ORIGINSEmanuel McCrayNo ratings yet
- Fast Furious Report Part 1Document211 pagesFast Furious Report Part 1dcodreaNo ratings yet
- Eleven-Page Journal Entry in W. MI U. Vaccine Mandate Case Dated Oct. 7th, 2021Document11 pagesEleven-Page Journal Entry in W. MI U. Vaccine Mandate Case Dated Oct. 7th, 2021Harry the Greek100% (1)
- Bioweapon AttackDocument3 pagesBioweapon Attackta84288No ratings yet
- International: Documents Reveal Top NSA Hacking UnitDocument4 pagesInternational: Documents Reveal Top NSA Hacking UnitEb OlaNo ratings yet
- #Karenhudes Karen Hudes Jesuit Vatican Gold #Chemtrails #Geoengineering PDFDocument20 pages#Karenhudes Karen Hudes Jesuit Vatican Gold #Chemtrails #Geoengineering PDFsisterrosettaNo ratings yet
- "Obama Worse Than Bush", David R. HoffmanDocument5 pages"Obama Worse Than Bush", David R. HoffmanGiuliano ValverdeNo ratings yet
- ( ( (Media) ) ) Inflates Common Cold To Trash US ConstitutionDocument6 pages( ( (Media) ) ) Inflates Common Cold To Trash US ConstitutiongqqhqNo ratings yet
- Northwoods and Garden Plot PDFDocument58 pagesNorthwoods and Garden Plot PDFthierryNo ratings yet
- George Washington Letter On Dangers of Illuminati 25 Sep 1798Document5 pagesGeorge Washington Letter On Dangers of Illuminati 25 Sep 1798Mick RynningNo ratings yet
- Executive Order 12148Document9 pagesExecutive Order 12148Jeremy Green100% (1)
- Pfizer Under 17 Years Adverse Events Reported To CDCDocument149 pagesPfizer Under 17 Years Adverse Events Reported To CDCWilliam BanksNo ratings yet
- Evidence Swine FluDocument10 pagesEvidence Swine FluThorsteinn Thorsteinsson100% (1)
- Pentagon Papers Part IV B 3Document177 pagesPentagon Papers Part IV B 3KidNo ratings yet
- U S D C D C: Ontgomery Lair IbleyDocument27 pagesU S D C D C: Ontgomery Lair IbleyLartoonNo ratings yet
- CIA's Support To The Nazi War Criminal InvestigationsDocument8 pagesCIA's Support To The Nazi War Criminal InvestigationsThe Baked CatNo ratings yet
- A Journey In Other Worlds: A Romance of the FutureFrom EverandA Journey In Other Worlds: A Romance of the FutureRating: 2.5 out of 5 stars2.5/5 (12)
- Summary of Judy Mikovits & Kent Heckenlively's Plague of CorruptionFrom EverandSummary of Judy Mikovits & Kent Heckenlively's Plague of CorruptionNo ratings yet
- The TI Program: A Multi-Trillion Dollar Plot for Global Domination?: 1A, #1From EverandThe TI Program: A Multi-Trillion Dollar Plot for Global Domination?: 1A, #1No ratings yet
- Public Response Dispatcher DetailsDocument11 pagesPublic Response Dispatcher Detailsscribd4kmhNo ratings yet
- 2022 COVID 19 SPSL PosterDocument1 page2022 COVID 19 SPSL Posterscribd4kmhNo ratings yet
- (Cliff Notes) 1984Document47 pages(Cliff Notes) 1984scribd4kmhNo ratings yet
- Data Overview - CITY CARRIER ASSISTANT - NORTH HOLLYWOOD CA NC10784723Document4 pagesData Overview - CITY CARRIER ASSISTANT - NORTH HOLLYWOOD CA NC10784723scribd4kmhNo ratings yet
- Change Lives by Building: Better Systems of CareDocument6 pagesChange Lives by Building: Better Systems of Carescribd4kmhNo ratings yet
- Examinee Guide: POST Entry-Level Dispatcher Selection Test BatteryDocument9 pagesExaminee Guide: POST Entry-Level Dispatcher Selection Test Batteryscribd4kmhNo ratings yet
- 10yr F-U Psychosis - 2017-World - PsychiatryDocument3 pages10yr F-U Psychosis - 2017-World - Psychiatryscribd4kmhNo ratings yet
- Application For Temporary Smog Exemption For A Vehicle Located Out-Of-StateDocument1 pageApplication For Temporary Smog Exemption For A Vehicle Located Out-Of-Statescribd4kmhNo ratings yet
- Position StatementDocument6 pagesPosition Statementscribd4kmhNo ratings yet
- 4 False PremisesDocument30 pages4 False Premisesscribd4kmhNo ratings yet
- Abbass Royal College 2005 PDFDocument3 pagesAbbass Royal College 2005 PDFscribd4kmhNo ratings yet
- Jse 16 2Document166 pagesJse 16 2scribd4kmhNo ratings yet
- Short-Term Psychodynamic Psychotherapy For Somatic DisordersDocument10 pagesShort-Term Psychodynamic Psychotherapy For Somatic Disordersscribd4kmhNo ratings yet
- 05 Szasz and TorreyDocument14 pages05 Szasz and Torreyscribd4kmhNo ratings yet
- Express Checkout: Check Out Time Is 11:00 AmDocument1 pageExpress Checkout: Check Out Time Is 11:00 Amscribd4kmhNo ratings yet
- Amer Peds Recomm Re Psy Drugs and PregnancyDocument10 pagesAmer Peds Recomm Re Psy Drugs and Pregnancyscribd4kmhNo ratings yet
- Rschgate Psychoisi TX W TherDocument11 pagesRschgate Psychoisi TX W Therscribd4kmhNo ratings yet
- Somatization: Diagnosing It Sooner Through Emotion-Focused InterviewingDocument10 pagesSomatization: Diagnosing It Sooner Through Emotion-Focused Interviewingscribd4kmhNo ratings yet
- Instructions For Completing Inf 70 Request For Record InformationDocument5 pagesInstructions For Completing Inf 70 Request For Record Informationscribd4kmhNo ratings yet
- DR Childress Communicating With ChildrenDocument1 pageDR Childress Communicating With Childrenscribd4kmhNo ratings yet
- DR Childress Family TherapyDocument2 pagesDR Childress Family Therapyscribd4kmhNo ratings yet
- Form WHO Dewasa PDFDocument2 pagesForm WHO Dewasa PDFAbizar Agung WibawaNo ratings yet
- VastarelDocument20 pagesVastarelKristen FieldsNo ratings yet
- The Seasonal Health Questionnaire Is More EffectiveDocument2 pagesThe Seasonal Health Questionnaire Is More EffectiveMaíra DiasNo ratings yet
- Nursing Care PlansDocument31 pagesNursing Care PlansCyril Jane Caanyagan AcutNo ratings yet
- Trigeminal NeuralgiaDocument72 pagesTrigeminal NeuralgiaCocoMathewNo ratings yet
- Hints For Remembering Medication ClassificationsDocument2 pagesHints For Remembering Medication ClassificationsSarah SNo ratings yet
- نسخة 264889196 Tramadol Drug StudyDocument1 pageنسخة 264889196 Tramadol Drug StudyMeteab AlzhiryNo ratings yet
- Presented By: Lady Diane Cabriga Bsn-IiiDocument11 pagesPresented By: Lady Diane Cabriga Bsn-IiiDayan CabrigaNo ratings yet
- SickLeaveCertificate With and Without Diagnosis 20230717 154636Document2 pagesSickLeaveCertificate With and Without Diagnosis 20230717 154636rishibarathiNo ratings yet
- Reflective Functioning ManualDocument47 pagesReflective Functioning ManualAntonio Tejero PocielloNo ratings yet
- Cause and Effect ParagraphsDocument14 pagesCause and Effect ParagraphsJosue Nádasdy Borthwick50% (2)
- UrticariaDocument52 pagesUrticariappica8111No ratings yet
- The Good Indicators Guide:: Understanding How To Use and Choose IndicatorsDocument40 pagesThe Good Indicators Guide:: Understanding How To Use and Choose IndicatorssuperpaqsNo ratings yet
- Presented By: Ashlee Barbeau Student Occupational Therapist, Queen's UniversityDocument22 pagesPresented By: Ashlee Barbeau Student Occupational Therapist, Queen's UniversityDanielle Stella N'LucaNo ratings yet
- Lingualised Occ RevisitedDocument5 pagesLingualised Occ RevisitedDrPrachi AgrawalNo ratings yet
- Liver Cirrhosis PDFDocument9 pagesLiver Cirrhosis PDFDennis CobbNo ratings yet
- 6Cs in Social Care GuideDocument4 pages6Cs in Social Care GuideLoo DrBradNo ratings yet
- Dizziness - PPPD Information SheetDocument8 pagesDizziness - PPPD Information Sheettan_siqi100% (1)
- Assessment of Pain in ChildrenDocument30 pagesAssessment of Pain in ChildrenVlad AlexandraNo ratings yet
- Role of Double J Stenting After Uncomplicated Ureterorenoscopy For 1 Centimeter Ureteral Stones: A Randomised Control TrialDocument3 pagesRole of Double J Stenting After Uncomplicated Ureterorenoscopy For 1 Centimeter Ureteral Stones: A Randomised Control TrialAnonymous izrFWiQNo ratings yet
- Palatal InjectionDocument10 pagesPalatal InjectionJose Salas AdragnaNo ratings yet
- Cambridge English For Nursing Grammar Practice Pre Intermediate Unit6Document3 pagesCambridge English For Nursing Grammar Practice Pre Intermediate Unit6Jorge CampiNo ratings yet
- Laboratory Services in HospitalDocument58 pagesLaboratory Services in HospitalDr. Rakshit SolankiNo ratings yet
- ARB and CCB CombinationDocument11 pagesARB and CCB CombinationLucky PratamaNo ratings yet
- CEBM Levels of EvidenceDocument2 pagesCEBM Levels of Evidence2012100% (2)
- Advanced Practice Nursing in The Philippines: Are We There Yet?Document5 pagesAdvanced Practice Nursing in The Philippines: Are We There Yet?Alex LavadiaNo ratings yet
- DMPC CoeDocument1 pageDMPC CoeJulius Magaru RaquelNo ratings yet
- Leg UlcersDocument22 pagesLeg UlcersMarera DomnicNo ratings yet