
April 2016
April 2016
You might also like
- Canteen Check ListDocument6 pagesCanteen Check ListKunal Raheja75% (8)
- Capacity Planning at Shouldice HospitalDocument9 pagesCapacity Planning at Shouldice HospitalGilbert G. Asuncion Jr.No ratings yet
- Shouldice Case StudyDocument5 pagesShouldice Case StudyMirza Adikresna100% (1)
- Case Analysis Shouldice Hospital Limited 12Document11 pagesCase Analysis Shouldice Hospital Limited 12Grace Gao100% (1)
- #Design and Implementation of Computerized Medical Duties Scheduling System - Inimax HubDocument77 pages#Design and Implementation of Computerized Medical Duties Scheduling System - Inimax Hubclarus100% (1)
- Personal Hygiene PPTDocument16 pagesPersonal Hygiene PPTAnmol Sharma100% (2)
- Case Study SorianoDocument3 pagesCase Study SorianoErika SorianoNo ratings yet
- Discharges Final (Gap, Flowchart, Checklist)Document24 pagesDischarges Final (Gap, Flowchart, Checklist)akinravNo ratings yet
- StaffingDocument20 pagesStaffingmohsinayaz100% (3)
- PROJECT PROPOSAL Extension of ClinicDocument2 pagesPROJECT PROPOSAL Extension of ClinicFranc Anthony Galao100% (2)
- Shouldice Hospital SolutionDocument8 pagesShouldice Hospital SolutionSyed Ahmer RizviNo ratings yet
- Objectives of Staffing in NursingDocument10 pagesObjectives of Staffing in NursingEli Zza KoiralaNo ratings yet
- DeveshDocument14 pagesDeveshAr Aditya SagarNo ratings yet
- Hand Hygiene: Alcohol Based Hand RubDocument2 pagesHand Hygiene: Alcohol Based Hand RubKIERSTINE MARIE BARCELONo ratings yet
- ADA - Infection Control Guidelines 2012Document50 pagesADA - Infection Control Guidelines 2012Gujapaneni Ravi KumarNo ratings yet
- Picot PaperDocument11 pagesPicot Paperapi-24092736888% (8)
- Nursing StaffingDocument5 pagesNursing StaffingPeace Andong PerochoNo ratings yet
- Organisational Structure - Asian HeartDocument13 pagesOrganisational Structure - Asian HeartshwetadhotarNo ratings yet
- High Power CommitteeDocument39 pagesHigh Power CommitteeJaya PrabhaNo ratings yet
- Capacity Planning at Shouldice HospitalDocument9 pagesCapacity Planning at Shouldice HospitalMuayad Faraj0% (1)
- Staffing-Term PaperDocument9 pagesStaffing-Term PaperRodel CamposoNo ratings yet
- 4-Milk LabDocument10 pages4-Milk Labفرحة كمالNo ratings yet
- Norms of Staffing in NursingDocument34 pagesNorms of Staffing in NursingUdaya Sree87% (23)
- (Alia) CASE STUDY HSM541Document6 pages(Alia) CASE STUDY HSM541radia amalin99No ratings yet
- HRM CMPLTDocument9 pagesHRM CMPLTJithin PonathilNo ratings yet
- Reserch PaperDocument17 pagesReserch PaperVithanalage WathsalaNo ratings yet
- 2010 Seven Ways To No Delays FINAL (Low-Res)Document24 pages2010 Seven Ways To No Delays FINAL (Low-Res)Ruby SharmaNo ratings yet
- Burn Care CaseDocument8 pagesBurn Care CaseFahad AliNo ratings yet
- Microsoft Word Safe Staffing The Basics NHPPD Version 1 0Document15 pagesMicrosoft Word Safe Staffing The Basics NHPPD Version 1 0odin9360343No ratings yet
- Norms of Staffing in Nursing PDF FreeDocument34 pagesNorms of Staffing in Nursing PDF FreeChetanyadav PacheriyaNo ratings yet
- StaffingDocument31 pagesStaffingSwapnil MahapureNo ratings yet
- Annisha Rahmani Eksa Bintari Ike Imelda Sinaga Nurliza Permatasari Rika Pebriani Siti RobiahDocument53 pagesAnnisha Rahmani Eksa Bintari Ike Imelda Sinaga Nurliza Permatasari Rika Pebriani Siti Robiahrpebriani_1No ratings yet
- 9 Staffing and RecruitmentDocument37 pages9 Staffing and Recruitmentxr4dmNo ratings yet
- SIP Poster - Hannah PR2Document1 pageSIP Poster - Hannah PR2NCPQSWNo ratings yet
- Shouldice Hospital LTD: Group Case presentation-NMP25Document9 pagesShouldice Hospital LTD: Group Case presentation-NMP25Krishna TiwariNo ratings yet
- Emergency Obstrics CareDocument13 pagesEmergency Obstrics CareParesh SinghalNo ratings yet
- ARCHANA MUKHERJEE Project On Woodlands HospitalDocument26 pagesARCHANA MUKHERJEE Project On Woodlands Hospitaldipannita adhikaryNo ratings yet
- Shija IntroDocument27 pagesShija IntroHomeshori SoraishamNo ratings yet
- Ed Model of Care 2012Document68 pagesEd Model of Care 2012Hans GrobakNo ratings yet
- CHDC Hospital Quanti AnalysisDocument12 pagesCHDC Hospital Quanti Analysislloyd814No ratings yet
- Bab II Bag 1 FixDocument10 pagesBab II Bag 1 FixJimJim JimJimNo ratings yet
- EDJobDescriptionDocument18 pagesEDJobDescriptionAnonymous YqCxXQ6wF5No ratings yet
- EDJobDescriptionDocument18 pagesEDJobDescriptionAnonymous YqCxXQ6wF5No ratings yet
- Human Resource MXDocument21 pagesHuman Resource MXSobha ajoNo ratings yet
- Questions and AnswersDocument16 pagesQuestions and AnswersKavi priyaNo ratings yet
- 006 or Staffing PlanDocument8 pages006 or Staffing PlanAeryll JasminNo ratings yet
- HRM Project KMCHDocument15 pagesHRM Project KMCHPoorna Chandra0% (1)
- Synopsis FormatDocument4 pagesSynopsis FormatUrlam Srinivas Kumar100% (1)
- Staffing Model DescriptionDocument14 pagesStaffing Model DescriptionImwaniki21No ratings yet
- MSCI 102 Coursework ReportDocument8 pagesMSCI 102 Coursework ReportMartin AndreevNo ratings yet
- Hospital Care AnsDocument7 pagesHospital Care AnselizabethNo ratings yet
- ReportDocument126 pagesReportNeha Roy100% (1)
- PP 2Document6 pagesPP 2akositabon100% (1)
- 4 - Staffing & ScheduleDocument12 pages4 - Staffing & Scheduleمحمد حسنNo ratings yet
- Bab I Pendahuluan A. Latar BelakangDocument27 pagesBab I Pendahuluan A. Latar BelakangyeniNo ratings yet
- Fortis AnalysisDocument27 pagesFortis Analysisrahul kNo ratings yet
- Job TitleDocument60 pagesJob TitleDaud HospitalNo ratings yet
- ASAYMENTDocument7 pagesASAYMENTJohn Ervin AgenaNo ratings yet
- Preparation of Job DescriptionDocument7 pagesPreparation of Job DescriptionPrity Devi100% (1)
- Size Mix PDFDocument20 pagesSize Mix PDFZia MalikNo ratings yet
- 04 Ijms 223 22Document16 pages04 Ijms 223 22BRNSS Publication Hub InfoNo ratings yet
- Lean Doctors: A Bold and Practical Guide to Using Lean Principles to Transform Healthcare Systems, One Doctor at a TimeFrom EverandLean Doctors: A Bold and Practical Guide to Using Lean Principles to Transform Healthcare Systems, One Doctor at a TimeNo ratings yet
- Comprehensive Healthcare Simulation: Mobile Medical SimulationFrom EverandComprehensive Healthcare Simulation: Mobile Medical SimulationPatricia K. CarstensNo ratings yet
- The Clinical Practice Program: A How-to-Guide for Physician Leaders On Starting Up a Successful ProgramFrom EverandThe Clinical Practice Program: A How-to-Guide for Physician Leaders On Starting Up a Successful ProgramNo ratings yet
- The Ultimate Medical Consultant Interview Guide: Fifth Edition. Over 180 Interview Questions and Answers by Senior NHS Consultants, Practice on Clinical Governance, Teaching, Management, and COVID-19From EverandThe Ultimate Medical Consultant Interview Guide: Fifth Edition. Over 180 Interview Questions and Answers by Senior NHS Consultants, Practice on Clinical Governance, Teaching, Management, and COVID-19No ratings yet
- Scope of Work: To, MR - Pradeep Tower 16 Flat No-1606 Jaypee Kosmos Sector 134 NoidaDocument1 pageScope of Work: To, MR - Pradeep Tower 16 Flat No-1606 Jaypee Kosmos Sector 134 NoidaAr Aditya SagarNo ratings yet
- Scope of Work Prime Club Area Rs./Sqft. Total Wood Work Closet (Laminate Finish)Document7 pagesScope of Work Prime Club Area Rs./Sqft. Total Wood Work Closet (Laminate Finish)Ar Aditya SagarNo ratings yet
- JM FLorence QuotationDocument1 pageJM FLorence QuotationAr Aditya SagarNo ratings yet
- Laminates-Inner Surface: Virgo, Outer Surface: Greenlam Note - Fittings - Hettich Boards / Ply - Greenply: Carcass, Action Tesa HDHMR: ShutterDocument1 pageLaminates-Inner Surface: Virgo, Outer Surface: Greenlam Note - Fittings - Hettich Boards / Ply - Greenply: Carcass, Action Tesa HDHMR: ShutterAr Aditya SagarNo ratings yet
- Scope of Work Prime Club Area Rs./Sqft. Total Wood Work Closet (Laminate Finish)Document6 pagesScope of Work Prime Club Area Rs./Sqft. Total Wood Work Closet (Laminate Finish)Ar Aditya SagarNo ratings yet
- Scope of Work Prime Club Area Rs./Sqft. Total Wood WorkDocument5 pagesScope of Work Prime Club Area Rs./Sqft. Total Wood WorkAr Aditya SagarNo ratings yet
- Washroom Washroom 1: GurugramDocument4 pagesWashroom Washroom 1: GurugramAr Aditya SagarNo ratings yet
- Payment Plan Stages Amount DateDocument1 pagePayment Plan Stages Amount DateAr Aditya SagarNo ratings yet
- Scope of Work Prime Club Area Rs./Sqft. Total Wood Work: Paint WallpaperDocument5 pagesScope of Work Prime Club Area Rs./Sqft. Total Wood Work: Paint WallpaperAr Aditya SagarNo ratings yet
- Paint Wallpaper: False Ceiling (Pop J.K/ Sakarni)Document2 pagesPaint Wallpaper: False Ceiling (Pop J.K/ Sakarni)Ar Aditya SagarNo ratings yet
- HubantDocument3 pagesHubantAr Aditya SagarNo ratings yet
- Sanfrancesco 150410041419 Conversion Gate01Document16 pagesSanfrancesco 150410041419 Conversion Gate01Ar Aditya SagarNo ratings yet
- Allotment Date: MS152 13/jul/2019 45040486Document1 pageAllotment Date: MS152 13/jul/2019 45040486Ar Aditya SagarNo ratings yet
- About The Project:: HABITAT CENTRE Is Now Home Not Only ToDocument34 pagesAbout The Project:: HABITAT CENTRE Is Now Home Not Only ToAr Aditya SagarNo ratings yet
- Site PlanDocument1 pageSite PlanAr Aditya SagarNo ratings yet
- AnjaliDocument1 pageAnjaliAr Aditya SagarNo ratings yet
- Ground Floor PlanDocument1 pageGround Floor PlanAr Aditya SagarNo ratings yet
- College Plan Single LineDocument1 pageCollege Plan Single LineAr Aditya SagarNo ratings yet
- Elevat inDocument1 pageElevat inAr Aditya SagarNo ratings yet
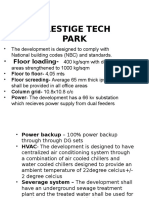
- Prestige Tech Park: - Floor LoadingDocument9 pagesPrestige Tech Park: - Floor LoadingAr Aditya SagarNo ratings yet
- Thesis Submission Check ListDocument2 pagesThesis Submission Check ListAr Aditya SagarNo ratings yet
- Baroque Architecture (Buildings and Architects) : Submitted ByDocument14 pagesBaroque Architecture (Buildings and Architects) : Submitted ByAr Aditya SagarNo ratings yet
- Ent of FeeDocument1 pageEnt of FeeAr Aditya SagarNo ratings yet
- Indian Standard Basic Requirements For Hospital Planning: 0. ForewordDocument2 pagesIndian Standard Basic Requirements For Hospital Planning: 0. ForewordAr Aditya SagarNo ratings yet
- Requirments Commercial ComplexDocument2 pagesRequirments Commercial ComplexAr Aditya SagarNo ratings yet
- Area Requirement1Document2 pagesArea Requirement1Ar Aditya SagarNo ratings yet
- Buddism Architecture: The Architecture of India Then Move TowardsDocument2 pagesBuddism Architecture: The Architecture of India Then Move TowardsAr Aditya SagarNo ratings yet
- Handwashing BoothDocument8 pagesHandwashing Boothapi-284180001No ratings yet
- Bag Tech Students-WordDocument5 pagesBag Tech Students-WordKing Nehpets AlczNo ratings yet
- WHO Research Agenda For Hand Hygiene in Health Care 2023-2030Document17 pagesWHO Research Agenda For Hand Hygiene in Health Care 2023-2030Catherine IskandarNo ratings yet
- A Lively & Healthy MeDocument18 pagesA Lively & Healthy MeARACELI RAITNo ratings yet
- PROCEDURE CHECKLIST FOR PRIMING IV TUBING AND ETC Revised 1Document3 pagesPROCEDURE CHECKLIST FOR PRIMING IV TUBING AND ETC Revised 1Nicole Sherry M. CHEENo ratings yet
- Rubric ClassroomDocument3 pagesRubric ClassroomErnest Gerard DuranoNo ratings yet
- Why Is Personal Hygiene ImportantDocument3 pagesWhy Is Personal Hygiene ImportantSirat KambojNo ratings yet
- CHG ChlorhexidineDocument73 pagesCHG Chlorhexidinetaher adelNo ratings yet
- Assessment Standard 7.2-4 Personal Environmental Safety TESTDocument4 pagesAssessment Standard 7.2-4 Personal Environmental Safety TESTnurse1990No ratings yet
- DM No. 524 S. 2022 2022 GLOBAL HANDWASHING DAY CELEBRATIONDocument7 pagesDM No. 524 S. 2022 2022 GLOBAL HANDWASHING DAY CELEBRATIONEhlee Eton TubalinalNo ratings yet
- Hand HygieneDocument11 pagesHand HygieneAllan M Murray-doNo ratings yet
- Bussiness Plan AAU (Dessalegn) - 1Document20 pagesBussiness Plan AAU (Dessalegn) - 1firehiwotmisganaw3No ratings yet
- HandHygiene PDFDocument5 pagesHandHygiene PDFDrBishnu Prasad MahalaNo ratings yet
- PDF (SG) - EAP 11 - 12 - UNIT 7 - LESSON 1 - Features and Structure of A Critique PaperDocument17 pagesPDF (SG) - EAP 11 - 12 - UNIT 7 - LESSON 1 - Features and Structure of A Critique PaperMayNo ratings yet
- IFS Food UFP Harmonized Checklist JUNE2014 2Document45 pagesIFS Food UFP Harmonized Checklist JUNE2014 2Gerardcp100% (1)
- Alberta Food Safety Basics For Meat Processors BookletDocument53 pagesAlberta Food Safety Basics For Meat Processors BookletThiago LucasNo ratings yet
- Q3 Health 8 Module 5 PDFDocument13 pagesQ3 Health 8 Module 5 PDFkateNo ratings yet
- Washing HandsDocument1 pageWashing HandsWin Maung TNo ratings yet
- Preparation of FoodDocument36 pagesPreparation of FoodJUSTIN RECELESTINONo ratings yet
- Conducting and Organizing Community Leaders MeetingDocument8 pagesConducting and Organizing Community Leaders MeetingDhasarathan100% (1)
- Bag TechniqueDocument5 pagesBag Techniqueamp_raphNo ratings yet
- Lynn13 4Document2 pagesLynn13 4Harley Justiniani Dela CruzNo ratings yet
- Eng IX PDFDocument228 pagesEng IX PDFMuhammad Ayaan AsrarNo ratings yet
- Complete Bed BathDocument4 pagesComplete Bed BathYeesha Palacio BalmesNo ratings yet
- (Azadirachta Indica), HOLY BASIL (Ocimum Sanctum), AND LEMON (Citrus Limon)Document23 pages(Azadirachta Indica), HOLY BASIL (Ocimum Sanctum), AND LEMON (Citrus Limon)Camille SalmasanNo ratings yet




















































































































Download as pdf or txt
You might also like
- Canteen Check ListDocument6 pagesCanteen Check ListKunal Raheja75% (8)
- Capacity Planning at Shouldice HospitalDocument9 pagesCapacity Planning at Shouldice HospitalGilbert G. Asuncion Jr.No ratings yet
- Shouldice Case StudyDocument5 pagesShouldice Case StudyMirza Adikresna100% (1)
- Case Analysis Shouldice Hospital Limited 12Document11 pagesCase Analysis Shouldice Hospital Limited 12Grace Gao100% (1)
- #Design and Implementation of Computerized Medical Duties Scheduling System - Inimax HubDocument77 pages#Design and Implementation of Computerized Medical Duties Scheduling System - Inimax Hubclarus100% (1)
- Personal Hygiene PPTDocument16 pagesPersonal Hygiene PPTAnmol Sharma100% (2)
- Case Study SorianoDocument3 pagesCase Study SorianoErika SorianoNo ratings yet
- Discharges Final (Gap, Flowchart, Checklist)Document24 pagesDischarges Final (Gap, Flowchart, Checklist)akinravNo ratings yet
- StaffingDocument20 pagesStaffingmohsinayaz100% (3)
- PROJECT PROPOSAL Extension of ClinicDocument2 pagesPROJECT PROPOSAL Extension of ClinicFranc Anthony Galao100% (2)
- Shouldice Hospital SolutionDocument8 pagesShouldice Hospital SolutionSyed Ahmer RizviNo ratings yet
- Objectives of Staffing in NursingDocument10 pagesObjectives of Staffing in NursingEli Zza KoiralaNo ratings yet
- DeveshDocument14 pagesDeveshAr Aditya SagarNo ratings yet
- Hand Hygiene: Alcohol Based Hand RubDocument2 pagesHand Hygiene: Alcohol Based Hand RubKIERSTINE MARIE BARCELONo ratings yet
- ADA - Infection Control Guidelines 2012Document50 pagesADA - Infection Control Guidelines 2012Gujapaneni Ravi KumarNo ratings yet
- Picot PaperDocument11 pagesPicot Paperapi-24092736888% (8)
- Nursing StaffingDocument5 pagesNursing StaffingPeace Andong PerochoNo ratings yet
- Organisational Structure - Asian HeartDocument13 pagesOrganisational Structure - Asian HeartshwetadhotarNo ratings yet
- High Power CommitteeDocument39 pagesHigh Power CommitteeJaya PrabhaNo ratings yet
- Capacity Planning at Shouldice HospitalDocument9 pagesCapacity Planning at Shouldice HospitalMuayad Faraj0% (1)
- Staffing-Term PaperDocument9 pagesStaffing-Term PaperRodel CamposoNo ratings yet
- 4-Milk LabDocument10 pages4-Milk Labفرحة كمالNo ratings yet
- Norms of Staffing in NursingDocument34 pagesNorms of Staffing in NursingUdaya Sree87% (23)
- (Alia) CASE STUDY HSM541Document6 pages(Alia) CASE STUDY HSM541radia amalin99No ratings yet
- HRM CMPLTDocument9 pagesHRM CMPLTJithin PonathilNo ratings yet
- Reserch PaperDocument17 pagesReserch PaperVithanalage WathsalaNo ratings yet
- 2010 Seven Ways To No Delays FINAL (Low-Res)Document24 pages2010 Seven Ways To No Delays FINAL (Low-Res)Ruby SharmaNo ratings yet
- Burn Care CaseDocument8 pagesBurn Care CaseFahad AliNo ratings yet
- Microsoft Word Safe Staffing The Basics NHPPD Version 1 0Document15 pagesMicrosoft Word Safe Staffing The Basics NHPPD Version 1 0odin9360343No ratings yet
- Norms of Staffing in Nursing PDF FreeDocument34 pagesNorms of Staffing in Nursing PDF FreeChetanyadav PacheriyaNo ratings yet
- StaffingDocument31 pagesStaffingSwapnil MahapureNo ratings yet
- Annisha Rahmani Eksa Bintari Ike Imelda Sinaga Nurliza Permatasari Rika Pebriani Siti RobiahDocument53 pagesAnnisha Rahmani Eksa Bintari Ike Imelda Sinaga Nurliza Permatasari Rika Pebriani Siti Robiahrpebriani_1No ratings yet
- 9 Staffing and RecruitmentDocument37 pages9 Staffing and Recruitmentxr4dmNo ratings yet
- SIP Poster - Hannah PR2Document1 pageSIP Poster - Hannah PR2NCPQSWNo ratings yet
- Shouldice Hospital LTD: Group Case presentation-NMP25Document9 pagesShouldice Hospital LTD: Group Case presentation-NMP25Krishna TiwariNo ratings yet
- Emergency Obstrics CareDocument13 pagesEmergency Obstrics CareParesh SinghalNo ratings yet
- ARCHANA MUKHERJEE Project On Woodlands HospitalDocument26 pagesARCHANA MUKHERJEE Project On Woodlands Hospitaldipannita adhikaryNo ratings yet
- Shija IntroDocument27 pagesShija IntroHomeshori SoraishamNo ratings yet
- Ed Model of Care 2012Document68 pagesEd Model of Care 2012Hans GrobakNo ratings yet
- CHDC Hospital Quanti AnalysisDocument12 pagesCHDC Hospital Quanti Analysislloyd814No ratings yet
- Bab II Bag 1 FixDocument10 pagesBab II Bag 1 FixJimJim JimJimNo ratings yet
- EDJobDescriptionDocument18 pagesEDJobDescriptionAnonymous YqCxXQ6wF5No ratings yet
- EDJobDescriptionDocument18 pagesEDJobDescriptionAnonymous YqCxXQ6wF5No ratings yet
- Human Resource MXDocument21 pagesHuman Resource MXSobha ajoNo ratings yet
- Questions and AnswersDocument16 pagesQuestions and AnswersKavi priyaNo ratings yet
- 006 or Staffing PlanDocument8 pages006 or Staffing PlanAeryll JasminNo ratings yet
- HRM Project KMCHDocument15 pagesHRM Project KMCHPoorna Chandra0% (1)
- Synopsis FormatDocument4 pagesSynopsis FormatUrlam Srinivas Kumar100% (1)
- Staffing Model DescriptionDocument14 pagesStaffing Model DescriptionImwaniki21No ratings yet
- MSCI 102 Coursework ReportDocument8 pagesMSCI 102 Coursework ReportMartin AndreevNo ratings yet
- Hospital Care AnsDocument7 pagesHospital Care AnselizabethNo ratings yet
- ReportDocument126 pagesReportNeha Roy100% (1)
- PP 2Document6 pagesPP 2akositabon100% (1)
- 4 - Staffing & ScheduleDocument12 pages4 - Staffing & Scheduleمحمد حسنNo ratings yet
- Bab I Pendahuluan A. Latar BelakangDocument27 pagesBab I Pendahuluan A. Latar BelakangyeniNo ratings yet
- Fortis AnalysisDocument27 pagesFortis Analysisrahul kNo ratings yet
- Job TitleDocument60 pagesJob TitleDaud HospitalNo ratings yet
- ASAYMENTDocument7 pagesASAYMENTJohn Ervin AgenaNo ratings yet
- Preparation of Job DescriptionDocument7 pagesPreparation of Job DescriptionPrity Devi100% (1)
- Size Mix PDFDocument20 pagesSize Mix PDFZia MalikNo ratings yet
- 04 Ijms 223 22Document16 pages04 Ijms 223 22BRNSS Publication Hub InfoNo ratings yet
- Lean Doctors: A Bold and Practical Guide to Using Lean Principles to Transform Healthcare Systems, One Doctor at a TimeFrom EverandLean Doctors: A Bold and Practical Guide to Using Lean Principles to Transform Healthcare Systems, One Doctor at a TimeNo ratings yet
- Comprehensive Healthcare Simulation: Mobile Medical SimulationFrom EverandComprehensive Healthcare Simulation: Mobile Medical SimulationPatricia K. CarstensNo ratings yet
- The Clinical Practice Program: A How-to-Guide for Physician Leaders On Starting Up a Successful ProgramFrom EverandThe Clinical Practice Program: A How-to-Guide for Physician Leaders On Starting Up a Successful ProgramNo ratings yet
- The Ultimate Medical Consultant Interview Guide: Fifth Edition. Over 180 Interview Questions and Answers by Senior NHS Consultants, Practice on Clinical Governance, Teaching, Management, and COVID-19From EverandThe Ultimate Medical Consultant Interview Guide: Fifth Edition. Over 180 Interview Questions and Answers by Senior NHS Consultants, Practice on Clinical Governance, Teaching, Management, and COVID-19No ratings yet
- Scope of Work: To, MR - Pradeep Tower 16 Flat No-1606 Jaypee Kosmos Sector 134 NoidaDocument1 pageScope of Work: To, MR - Pradeep Tower 16 Flat No-1606 Jaypee Kosmos Sector 134 NoidaAr Aditya SagarNo ratings yet
- Scope of Work Prime Club Area Rs./Sqft. Total Wood Work Closet (Laminate Finish)Document7 pagesScope of Work Prime Club Area Rs./Sqft. Total Wood Work Closet (Laminate Finish)Ar Aditya SagarNo ratings yet
- JM FLorence QuotationDocument1 pageJM FLorence QuotationAr Aditya SagarNo ratings yet
- Laminates-Inner Surface: Virgo, Outer Surface: Greenlam Note - Fittings - Hettich Boards / Ply - Greenply: Carcass, Action Tesa HDHMR: ShutterDocument1 pageLaminates-Inner Surface: Virgo, Outer Surface: Greenlam Note - Fittings - Hettich Boards / Ply - Greenply: Carcass, Action Tesa HDHMR: ShutterAr Aditya SagarNo ratings yet
- Scope of Work Prime Club Area Rs./Sqft. Total Wood Work Closet (Laminate Finish)Document6 pagesScope of Work Prime Club Area Rs./Sqft. Total Wood Work Closet (Laminate Finish)Ar Aditya SagarNo ratings yet
- Scope of Work Prime Club Area Rs./Sqft. Total Wood WorkDocument5 pagesScope of Work Prime Club Area Rs./Sqft. Total Wood WorkAr Aditya SagarNo ratings yet
- Washroom Washroom 1: GurugramDocument4 pagesWashroom Washroom 1: GurugramAr Aditya SagarNo ratings yet
- Payment Plan Stages Amount DateDocument1 pagePayment Plan Stages Amount DateAr Aditya SagarNo ratings yet
- Scope of Work Prime Club Area Rs./Sqft. Total Wood Work: Paint WallpaperDocument5 pagesScope of Work Prime Club Area Rs./Sqft. Total Wood Work: Paint WallpaperAr Aditya SagarNo ratings yet
- Paint Wallpaper: False Ceiling (Pop J.K/ Sakarni)Document2 pagesPaint Wallpaper: False Ceiling (Pop J.K/ Sakarni)Ar Aditya SagarNo ratings yet
- HubantDocument3 pagesHubantAr Aditya SagarNo ratings yet
- Sanfrancesco 150410041419 Conversion Gate01Document16 pagesSanfrancesco 150410041419 Conversion Gate01Ar Aditya SagarNo ratings yet
- Allotment Date: MS152 13/jul/2019 45040486Document1 pageAllotment Date: MS152 13/jul/2019 45040486Ar Aditya SagarNo ratings yet
- About The Project:: HABITAT CENTRE Is Now Home Not Only ToDocument34 pagesAbout The Project:: HABITAT CENTRE Is Now Home Not Only ToAr Aditya SagarNo ratings yet
- Site PlanDocument1 pageSite PlanAr Aditya SagarNo ratings yet
- AnjaliDocument1 pageAnjaliAr Aditya SagarNo ratings yet
- Ground Floor PlanDocument1 pageGround Floor PlanAr Aditya SagarNo ratings yet
- College Plan Single LineDocument1 pageCollege Plan Single LineAr Aditya SagarNo ratings yet
- Elevat inDocument1 pageElevat inAr Aditya SagarNo ratings yet
- Prestige Tech Park: - Floor LoadingDocument9 pagesPrestige Tech Park: - Floor LoadingAr Aditya SagarNo ratings yet
- Thesis Submission Check ListDocument2 pagesThesis Submission Check ListAr Aditya SagarNo ratings yet
- Baroque Architecture (Buildings and Architects) : Submitted ByDocument14 pagesBaroque Architecture (Buildings and Architects) : Submitted ByAr Aditya SagarNo ratings yet
- Ent of FeeDocument1 pageEnt of FeeAr Aditya SagarNo ratings yet
- Indian Standard Basic Requirements For Hospital Planning: 0. ForewordDocument2 pagesIndian Standard Basic Requirements For Hospital Planning: 0. ForewordAr Aditya SagarNo ratings yet
- Requirments Commercial ComplexDocument2 pagesRequirments Commercial ComplexAr Aditya SagarNo ratings yet
- Area Requirement1Document2 pagesArea Requirement1Ar Aditya SagarNo ratings yet
- Buddism Architecture: The Architecture of India Then Move TowardsDocument2 pagesBuddism Architecture: The Architecture of India Then Move TowardsAr Aditya SagarNo ratings yet
- Handwashing BoothDocument8 pagesHandwashing Boothapi-284180001No ratings yet
- Bag Tech Students-WordDocument5 pagesBag Tech Students-WordKing Nehpets AlczNo ratings yet
- WHO Research Agenda For Hand Hygiene in Health Care 2023-2030Document17 pagesWHO Research Agenda For Hand Hygiene in Health Care 2023-2030Catherine IskandarNo ratings yet
- A Lively & Healthy MeDocument18 pagesA Lively & Healthy MeARACELI RAITNo ratings yet
- PROCEDURE CHECKLIST FOR PRIMING IV TUBING AND ETC Revised 1Document3 pagesPROCEDURE CHECKLIST FOR PRIMING IV TUBING AND ETC Revised 1Nicole Sherry M. CHEENo ratings yet
- Rubric ClassroomDocument3 pagesRubric ClassroomErnest Gerard DuranoNo ratings yet
- Why Is Personal Hygiene ImportantDocument3 pagesWhy Is Personal Hygiene ImportantSirat KambojNo ratings yet
- CHG ChlorhexidineDocument73 pagesCHG Chlorhexidinetaher adelNo ratings yet
- Assessment Standard 7.2-4 Personal Environmental Safety TESTDocument4 pagesAssessment Standard 7.2-4 Personal Environmental Safety TESTnurse1990No ratings yet
- DM No. 524 S. 2022 2022 GLOBAL HANDWASHING DAY CELEBRATIONDocument7 pagesDM No. 524 S. 2022 2022 GLOBAL HANDWASHING DAY CELEBRATIONEhlee Eton TubalinalNo ratings yet
- Hand HygieneDocument11 pagesHand HygieneAllan M Murray-doNo ratings yet
- Bussiness Plan AAU (Dessalegn) - 1Document20 pagesBussiness Plan AAU (Dessalegn) - 1firehiwotmisganaw3No ratings yet
- HandHygiene PDFDocument5 pagesHandHygiene PDFDrBishnu Prasad MahalaNo ratings yet
- PDF (SG) - EAP 11 - 12 - UNIT 7 - LESSON 1 - Features and Structure of A Critique PaperDocument17 pagesPDF (SG) - EAP 11 - 12 - UNIT 7 - LESSON 1 - Features and Structure of A Critique PaperMayNo ratings yet
- IFS Food UFP Harmonized Checklist JUNE2014 2Document45 pagesIFS Food UFP Harmonized Checklist JUNE2014 2Gerardcp100% (1)
- Alberta Food Safety Basics For Meat Processors BookletDocument53 pagesAlberta Food Safety Basics For Meat Processors BookletThiago LucasNo ratings yet
- Q3 Health 8 Module 5 PDFDocument13 pagesQ3 Health 8 Module 5 PDFkateNo ratings yet
- Washing HandsDocument1 pageWashing HandsWin Maung TNo ratings yet
- Preparation of FoodDocument36 pagesPreparation of FoodJUSTIN RECELESTINONo ratings yet
- Conducting and Organizing Community Leaders MeetingDocument8 pagesConducting and Organizing Community Leaders MeetingDhasarathan100% (1)
- Bag TechniqueDocument5 pagesBag Techniqueamp_raphNo ratings yet
- Lynn13 4Document2 pagesLynn13 4Harley Justiniani Dela CruzNo ratings yet
- Eng IX PDFDocument228 pagesEng IX PDFMuhammad Ayaan AsrarNo ratings yet
- Complete Bed BathDocument4 pagesComplete Bed BathYeesha Palacio BalmesNo ratings yet
- (Azadirachta Indica), HOLY BASIL (Ocimum Sanctum), AND LEMON (Citrus Limon)Document23 pages(Azadirachta Indica), HOLY BASIL (Ocimum Sanctum), AND LEMON (Citrus Limon)Camille SalmasanNo ratings yet