Download as docx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Dodigen 2808 TDSDocument1 pageDodigen 2808 TDSRashid SaleemNo ratings yet
- 1.) Pumping ProblemsDocument3 pages1.) Pumping ProblemsKaren EstavilloNo ratings yet
- ESTAVILLO, Karen G. (FEVER UTI, CONSTI)Document4 pagesESTAVILLO, Karen G. (FEVER UTI, CONSTI)Karen EstavilloNo ratings yet
- Obesity: Far Eastern University - Nicanor Reyes Medical FoundationDocument5 pagesObesity: Far Eastern University - Nicanor Reyes Medical FoundationKaren EstavilloNo ratings yet
- (ObstetricsA) Prenatal Care - Dr. San Jose (Lea Pacis)Document12 pages(ObstetricsA) Prenatal Care - Dr. San Jose (Lea Pacis)Karen EstavilloNo ratings yet
- Case BDocument2 pagesCase BKaren EstavilloNo ratings yet
- Renal Cell Carcinoma-ReportDocument6 pagesRenal Cell Carcinoma-ReportKaren EstavilloNo ratings yet
- Teratology, Teratogens, and Fetotoxic AgentsDocument92 pagesTeratology, Teratogens, and Fetotoxic AgentsKaren EstavilloNo ratings yet
- Far Eastern University - Nicanor Reyes Medical Foundation: Clinical Diagnosis B Lab Activity - Stool Analysis OrientationDocument3 pagesFar Eastern University - Nicanor Reyes Medical Foundation: Clinical Diagnosis B Lab Activity - Stool Analysis OrientationKaren EstavilloNo ratings yet
- Far Eastern University - Nicanor Reyes Medical Foundation: Clinical Diagnosis B Lab Activity - Stool Analysis OrientationDocument3 pagesFar Eastern University - Nicanor Reyes Medical Foundation: Clinical Diagnosis B Lab Activity - Stool Analysis OrientationKaren EstavilloNo ratings yet
- Anterior Abdominal Wall - Dr. Bea (KK)Document3 pagesAnterior Abdominal Wall - Dr. Bea (KK)Karen EstavilloNo ratings yet
- Disclosure & Family CeaDocument3 pagesDisclosure & Family CeaKaren EstavilloNo ratings yet
- What Is Galactosemia?: GalactoseDocument8 pagesWhat Is Galactosemia?: GalactoseKaren EstavilloNo ratings yet
- Red and Blue! (Complete)Document18 pagesRed and Blue! (Complete)Karen EstavilloNo ratings yet
- Galactosemia 1B1G6Document13 pagesGalactosemia 1B1G6Karen Estavillo100% (1)
- Waiver Company Visit (OJT)Document1 pageWaiver Company Visit (OJT)Karen EstavilloNo ratings yet
- To Whom It May ConcernDocument8 pagesTo Whom It May ConcernKaren EstavilloNo ratings yet
- InfectionDocument2 pagesInfectionKaren EstavilloNo ratings yet
- Galactose MiaDocument12 pagesGalactose MiaKaren EstavilloNo ratings yet
- Darell Albay Domondon: I. Personal InformationDocument2 pagesDarell Albay Domondon: I. Personal InformationKaren EstavilloNo ratings yet
- The Nirma Story!: - Vikram U. MoreDocument15 pagesThe Nirma Story!: - Vikram U. Moreamit_12No ratings yet
- Celullar Respiration Notes Grade 12Document8 pagesCelullar Respiration Notes Grade 12Mafalda SeabraNo ratings yet
- 24-01-2023 - SR - Super60 - NUCLEUS & ALL - BT - Jee-Main-GTM-14 - Q.PAPERDocument20 pages24-01-2023 - SR - Super60 - NUCLEUS & ALL - BT - Jee-Main-GTM-14 - Q.PAPERkasalachinuNo ratings yet
- Ozonation of Dye in A Fixed Bed Batch Bubble Column Reactor-A Case Study For The Removal of Persistent Chemicals in Waste Water by Tertiary Treatment.Document13 pagesOzonation of Dye in A Fixed Bed Batch Bubble Column Reactor-A Case Study For The Removal of Persistent Chemicals in Waste Water by Tertiary Treatment.S Bharadwaj ReddyNo ratings yet
- Chemistry ProjectDocument14 pagesChemistry ProjectnrdwallahNo ratings yet
- Arctic and Subarctic Construction Calculation Methods For Determination of Depths of Freeze and Thaw in SoilsDocument62 pagesArctic and Subarctic Construction Calculation Methods For Determination of Depths of Freeze and Thaw in SoilsGAEL MICHEL-GROSJEANNo ratings yet
- MHPS Jac GTDocument7 pagesMHPS Jac GTkp pkNo ratings yet
- United States Environmental Protection Agency Washington, DC 20460Document30 pagesUnited States Environmental Protection Agency Washington, DC 20460Kelvin Troubadour MchelseaNo ratings yet
- FMEA BoilerDocument2 pagesFMEA BoilerKevin FloresNo ratings yet
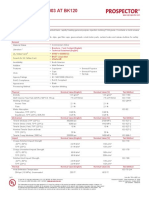
- Ultraform® N 2320 003 AT BK120Document3 pagesUltraform® N 2320 003 AT BK120Vu TranNo ratings yet
- Marine PDFDocument578 pagesMarine PDFNizar BouchaalaNo ratings yet
- Candle N MatchDocument12 pagesCandle N MatchAzee Berihun AbNo ratings yet
- Kinetics Study On The Reaction Between Potassium Iodate and Sodium Sulphite (Theory) - Class 12 - Chemistry - Amrita Online LabDocument3 pagesKinetics Study On The Reaction Between Potassium Iodate and Sodium Sulphite (Theory) - Class 12 - Chemistry - Amrita Online Labganesh kumarNo ratings yet
- Turboflow XL 32Document10 pagesTurboflow XL 32Chris StroudNo ratings yet
- N0 Tahun Chemical Engineering Plant Cost IndexDocument8 pagesN0 Tahun Chemical Engineering Plant Cost IndexIlham Kiki ShahilaNo ratings yet
- Glass Fiber Post Ifu Msds L 198 0611 v4 NPDocument2 pagesGlass Fiber Post Ifu Msds L 198 0611 v4 NPMelih AltıntaşNo ratings yet
- Calcium Silicate Data SheetDocument2 pagesCalcium Silicate Data Sheetkresimir.mikoc9765No ratings yet
- 02-General Principals of Metallurgical operations-Ques.-Final-EDocument11 pages02-General Principals of Metallurgical operations-Ques.-Final-EAbhishek RavirajNo ratings yet
- Is 3076Document18 pagesIs 3076Sathish KumarNo ratings yet
- FM 38-700 Packaging of Materiel - PreservationDocument267 pagesFM 38-700 Packaging of Materiel - PreservationJared A. Lang100% (1)
- C10 Chemical Bonding IIDocument64 pagesC10 Chemical Bonding IIJay-pee BarronNo ratings yet
- CFP 00105 CHEMISTRY 1 - Laboratory Manual UNIKLDocument21 pagesCFP 00105 CHEMISTRY 1 - Laboratory Manual UNIKLIrham SyahmiNo ratings yet
- Material Property ReportDocument25 pagesMaterial Property Reporta4idNo ratings yet
- Comparative Analysis of Some Toxic Metals in Some Brands of Yogurt Drinks Sold in MalumfashiDocument45 pagesComparative Analysis of Some Toxic Metals in Some Brands of Yogurt Drinks Sold in MalumfashiHamza ummusalma Ali100% (1)
- Astm B 265 - 03Document8 pagesAstm B 265 - 03kaminaljuyuNo ratings yet
- PNS RocuroniumDocument2 pagesPNS RocuroniumKim RuizNo ratings yet
- Trends in Period 3Document34 pagesTrends in Period 3Fildzah AdanyNo ratings yet
- Chapter 2 - FIRE SAFETY PREVENTION SYSTEMDocument66 pagesChapter 2 - FIRE SAFETY PREVENTION SYSTEMHUHU yeszNo ratings yet
- General Office Cleaning: Example Risk Assessment ForDocument3 pagesGeneral Office Cleaning: Example Risk Assessment Forisak23No ratings yet