Download as pdf or txt
You might also like
- ST Richards Floor PlanDocument2 pagesST Richards Floor PlanMarc33% (3)
- Ramsay Sedation Scale and How To Use ItDocument10 pagesRamsay Sedation Scale and How To Use ItAdinda Putra PradhanaNo ratings yet
- Nursing Care Plan For Alzheimer's DiseaseDocument4 pagesNursing Care Plan For Alzheimer's DiseaseRnspeakcom100% (1)
- ANC OB and GYN HISTORY Taking SampleDocument43 pagesANC OB and GYN HISTORY Taking SampleGebremichael Reta100% (3)
- Brain AbcesDocument6 pagesBrain AbcesGintar Isnu WardoyoNo ratings yet
- AbcesoDocument2 pagesAbcesoRocio LedesmaNo ratings yet
- Mold Infections of The Central Nervous SystemDocument15 pagesMold Infections of The Central Nervous SystemJohn TusselNo ratings yet
- Brain Abscess: State-Of-The-Art Clinical ArticleDocument17 pagesBrain Abscess: State-Of-The-Art Clinical ArticleAwais KhanNo ratings yet
- Brain Abscess: State-Of-The-Art Clinical ArticleDocument17 pagesBrain Abscess: State-Of-The-Art Clinical ArticleIqbal AbdillahNo ratings yet
- Cerebral Abscesses Imaging A Practical ApproachDocument14 pagesCerebral Abscesses Imaging A Practical Approachhasbi.alginaaNo ratings yet
- Invasive Cryptococcal Meningitis Presenting As A Skull Base Mass in An Immunocompetent Host: A Case ReportDocument5 pagesInvasive Cryptococcal Meningitis Presenting As A Skull Base Mass in An Immunocompetent Host: A Case ReportAsep RiswandiNo ratings yet
- Absceso CerebralDocument8 pagesAbsceso Cerebralgiseladelarosa2006No ratings yet
- Cerebral Toxoplasmosis: ClinicalpictureDocument2 pagesCerebral Toxoplasmosis: ClinicalpictureRahul RaiNo ratings yet
- Cerebral Toxoplasmosis - 1Document2 pagesCerebral Toxoplasmosis - 1hasbi.alginaaNo ratings yet
- 55 61 Brain AbscessDocument7 pages55 61 Brain AbscessNadia OktarinaNo ratings yet
- Community-Acquired Bacterial Meningitis in Adults: Review ArticleDocument10 pagesCommunity-Acquired Bacterial Meningitis in Adults: Review ArticleÁlvaro NBNo ratings yet
- Absceso Cerebral en RN Asociado A Infeccion UmbilicalDocument5 pagesAbsceso Cerebral en RN Asociado A Infeccion UmbilicalAbrahamKatimeNo ratings yet
- Abses Cerebri 1Document8 pagesAbses Cerebri 1astri sukma mNo ratings yet
- Bacterial Brain Abscess: Journal ReadingDocument22 pagesBacterial Brain Abscess: Journal ReadingdinarNo ratings yet
- Brain Abscess in Immunocompetent Adult PatientsDocument6 pagesBrain Abscess in Immunocompetent Adult PatientsshofwaNo ratings yet
- (10920684 - Neurosurgical Focus) Pyogenic Brain AbscessDocument10 pages(10920684 - Neurosurgical Focus) Pyogenic Brain AbscesschiquitaputriNo ratings yet
- Intracranial Infections Clinical and Imaging CharacteristicsDocument20 pagesIntracranial Infections Clinical and Imaging CharacteristicsRiyan NuelNo ratings yet
- (10920684 - Neurosurgical Focus) Intracranial Infections - Lessons Learned From 52 Surgically Treated CasesDocument8 pages(10920684 - Neurosurgical Focus) Intracranial Infections - Lessons Learned From 52 Surgically Treated CasesIsmail MuhammadNo ratings yet
- The Management of Intracranial AbscessesDocument3 pagesThe Management of Intracranial AbscessesDio AlexanderNo ratings yet
- Citrobacter Koseri Meningitis: A Neurosurgical Condition?Document4 pagesCitrobacter Koseri Meningitis: A Neurosurgical Condition?SukumarNo ratings yet
- Neurocysticercosis. A Frequent Cause of Seizures, Epilepsy, and OtherDocument12 pagesNeurocysticercosis. A Frequent Cause of Seizures, Epilepsy, and OtherMaria Lucero Jinés TapiaNo ratings yet
- Brain Abcess in ChildrenDocument5 pagesBrain Abcess in Childrencamelia musaadNo ratings yet
- Current Epidemiological Trends of Brain Abscess: A Clinicopathological StudyDocument9 pagesCurrent Epidemiological Trends of Brain Abscess: A Clinicopathological StudyNur Fadhilah KusnadiNo ratings yet
- Imaging of Intracranial InfectionsDocument12 pagesImaging of Intracranial Infectionsrafael rocha novaesNo ratings yet
- Tuberculomas of The Brain With and Without Associated Meningitis: A Cohort of 28 Cases Treated With Anti-Tuberculosis Drugs at A Tertiary Care CentreDocument4 pagesTuberculomas of The Brain With and Without Associated Meningitis: A Cohort of 28 Cases Treated With Anti-Tuberculosis Drugs at A Tertiary Care CentreDestyNo ratings yet
- Bodil Sen 2018Document15 pagesBodil Sen 2018Sannita Mayusda BadiriNo ratings yet
- Nihms 985420Document30 pagesNihms 985420Frank Harry LampardNo ratings yet
- Nej MR A 1216008Document11 pagesNej MR A 1216008guillosarahNo ratings yet
- Pubid-848078832 1010 PDFDocument10 pagesPubid-848078832 1010 PDFCocosul Cocosului CocosaruluiNo ratings yet
- Research ArticleDocument13 pagesResearch ArticlenetifarhatiiNo ratings yet
- Focus: Intracranial Infections: Lessons Learned From 52 Surgically Treated CasesDocument8 pagesFocus: Intracranial Infections: Lessons Learned From 52 Surgically Treated Casesjena maraNo ratings yet
- JurnalDocument4 pagesJurnalGaluh M ArtamtiNo ratings yet
- Prospective Study of Intracranial Space Occupying Lesions in Children in Correlation With C.T. ScanDocument8 pagesProspective Study of Intracranial Space Occupying Lesions in Children in Correlation With C.T. Scannurulanisa0703No ratings yet
- Actinomycotic Brain Abscess: Case ReportDocument3 pagesActinomycotic Brain Abscess: Case ReportIqbal AbdillahNo ratings yet
- Peripheral Primitive Neuro-Ectodermal Tumor of The Pleura About A Rare Caser, With Literature ReviewDocument4 pagesPeripheral Primitive Neuro-Ectodermal Tumor of The Pleura About A Rare Caser, With Literature ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Constellatus StrokeDocument4 pagesConstellatus StrokeW Antonio Rivera MartínezNo ratings yet
- Vol-1, Issue-1 Prospective Study of Peripheral Nerve Tumors Over A Period of 2 YearsDocument4 pagesVol-1, Issue-1 Prospective Study of Peripheral Nerve Tumors Over A Period of 2 YearsijhrmimsNo ratings yet
- 2 Brain AbscessDocument25 pages2 Brain AbscessKaif KhanNo ratings yet
- New 1Document12 pagesNew 1Muhammad SyaifullahNo ratings yet
- Cns ParasitesDocument74 pagesCns Parasitesahmed12mohamed12hNo ratings yet
- Clinical Symptoms, Diagnosis, and Treatment of NeurocysticercosisDocument15 pagesClinical Symptoms, Diagnosis, and Treatment of NeurocysticercosisIngVictorHuertaNo ratings yet
- Brain Abscess Following Meningitis in A Neonate: Report of Three CasesDocument6 pagesBrain Abscess Following Meningitis in A Neonate: Report of Three CasesprimayosiNo ratings yet
- Brain Abcess Journal 2Document4 pagesBrain Abcess Journal 2ansyemomoleNo ratings yet
- Brain Abscesses: An Overview in Children: Andrzej Krzyszto Fiak Paola Zangari Maia de Luca Alberto VillaniDocument4 pagesBrain Abscesses: An Overview in Children: Andrzej Krzyszto Fiak Paola Zangari Maia de Luca Alberto VillaniSannita Mayusda BadiriNo ratings yet
- Brain Abscess Management: Presenter: Pankaj Ailawadhi Moderators: PROF. BS SHARMA Dr. Sumit SinhaDocument86 pagesBrain Abscess Management: Presenter: Pankaj Ailawadhi Moderators: PROF. BS SHARMA Dr. Sumit SinhaDex RayNo ratings yet
- Brain AbscessDocument61 pagesBrain Abscessderarataye6No ratings yet
- READING Brain Abscess ContusionDocument2 pagesREADING Brain Abscess ContusionMaryzelle TayNo ratings yet
- Objetivo 3 Móvil PDFDocument26 pagesObjetivo 3 Móvil PDFnawal akarmaniNo ratings yet
- Neurotoxoplasmose e Neurocisticercose em Paciente Com AIDS - Relato de CasoDocument8 pagesNeurotoxoplasmose e Neurocisticercose em Paciente Com AIDS - Relato de CasoMarcinha BauerNo ratings yet
- 3.01 2023 Student PackDocument12 pages3.01 2023 Student Packrohanjeet59No ratings yet
- Mehu131 U1 T6 NeurocysticercosisDocument16 pagesMehu131 U1 T6 NeurocysticercosisGabriel OlivaresNo ratings yet
- Infections Diseases of The Central Nervous System: Chapter VI - J. RuscalledaDocument11 pagesInfections Diseases of The Central Nervous System: Chapter VI - J. RuscalledaArif BudimanNo ratings yet
- Fusobacterial - Brain - Abscess - Caused - by - ParadoxicalDocument3 pagesFusobacterial - Brain - Abscess - Caused - by - Paradoxicaldrsiddharthchoudhary15No ratings yet
- Clinicalsigns, Imagingfeatures, Neuropathology, Andoutcome Incatsanddogswithcentralnervoussystemcryptococcosis FromcaliforniaDocument12 pagesClinicalsigns, Imagingfeatures, Neuropathology, Andoutcome Incatsanddogswithcentralnervoussystemcryptococcosis FromcaliforniaMicheleBerselliNo ratings yet
- Neuroimaging Patterns of Intracranial Infections Meningitis, Cerebritis, and Their ComplicationsDocument31 pagesNeuroimaging Patterns of Intracranial Infections Meningitis, Cerebritis, and Their ComplicationsMauro Oscar Soares De Souza LimaNo ratings yet
- Case Bezold AbscessDocument3 pagesCase Bezold AbscessCarimaGhalieNo ratings yet
- Chronic MeningitisDocument7 pagesChronic Meningitisneurojuancarfab100% (1)
- Echography and Doppler of the BrainFrom EverandEchography and Doppler of the BrainChiara RobbaNo ratings yet
- Neurorheumatology: A Comprehenisve Guide to Immune Mediated Disorders of the Nervous SystemFrom EverandNeurorheumatology: A Comprehenisve Guide to Immune Mediated Disorders of the Nervous SystemNo ratings yet
- Jurnal MH PDFDocument12 pagesJurnal MH PDFcamelia musaadNo ratings yet
- Jurnal SistitisDocument5 pagesJurnal Sistitiscamelia musaadNo ratings yet
- Brain Abcess in ChildrenDocument5 pagesBrain Abcess in Childrencamelia musaadNo ratings yet
- Ebm JurnalDocument198 pagesEbm Jurnalcamelia musaadNo ratings yet
- Brain Abscess: H. R W, M.DDocument1 pageBrain Abscess: H. R W, M.Dcamelia musaadNo ratings yet
- ebook download (eBook PDF) Medical Assisting: Administrative Procedures 7th Edition all chapterDocument43 pagesebook download (eBook PDF) Medical Assisting: Administrative Procedures 7th Edition all chaptermaalidmayram100% (2)
- Healthctr Risk ManagementDocument32 pagesHealthctr Risk Managementapi-257281959No ratings yet
- Rsudza: Dr. Bobby H.E Fermi SDocument3 pagesRsudza: Dr. Bobby H.E Fermi Sdarr artNo ratings yet
- Action Plan UPDATEDDocument2 pagesAction Plan UPDATEDStephanie Villanueva AdvinculaNo ratings yet
- AphasiaDocument28 pagesAphasiaEmilio Emmanué Escobar CruzNo ratings yet
- DoctorsDocument7 pagesDoctorsbey luNo ratings yet
- Management of Gallbladder Polyps - An Optimal Strategy ProposedDocument4 pagesManagement of Gallbladder Polyps - An Optimal Strategy ProposedTANH NGUYENNo ratings yet
- Tinel's Sign and Phalen's Maneuver: Physical Signs of Carpal Tunnel SyndromeDocument4 pagesTinel's Sign and Phalen's Maneuver: Physical Signs of Carpal Tunnel SyndromeNursyifa NovyantiNo ratings yet
- Positioning 2Document4 pagesPositioning 2le chixNo ratings yet
- (Current Clinica (Current - Clinical - Strategies) - Gynecology - and - Obstetrics - 2004l Strategies) - Gynecology and Obstetrics 2004Document125 pages(Current Clinica (Current - Clinical - Strategies) - Gynecology - and - Obstetrics - 2004l Strategies) - Gynecology and Obstetrics 2004Eliza Stochita100% (1)
- Basic LessonDocument26 pagesBasic LessonTriciaNo ratings yet
- Juvenile Rheumatoid ArthritisDocument12 pagesJuvenile Rheumatoid ArthritisCatherine PoNo ratings yet
- Gynecologic Cytology Laboratory Practice and MethodologyDocument37 pagesGynecologic Cytology Laboratory Practice and MethodologySeby SebastianNo ratings yet
- The RADICAL Framework For Implementing and Monitoring Healthcare Risk ManagementDocument11 pagesThe RADICAL Framework For Implementing and Monitoring Healthcare Risk ManagementRangga PradanaNo ratings yet
- Suicidal Thoughts How To Support Someone Factsheet 1Document11 pagesSuicidal Thoughts How To Support Someone Factsheet 1Nikka Shaira OñezNo ratings yet
- The Body ElectricDocument335 pagesThe Body Electricsuper0sonicNo ratings yet
- MED 2.7 Gait and StationDocument3 pagesMED 2.7 Gait and StationelleinasNo ratings yet
- Eportfolio Resume CVDocument4 pagesEportfolio Resume CVapi-577441503No ratings yet
- 15 - Major and Minor ConnectorDocument94 pages15 - Major and Minor Connectorمعاذ العسافNo ratings yet
- Asthma & COPDDocument26 pagesAsthma & COPDraheenbushNo ratings yet
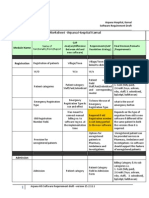
- Finalized Requirements-Worksheet - Arpana Hospital KarnalDocument11 pagesFinalized Requirements-Worksheet - Arpana Hospital KarnalMahesh PatilNo ratings yet
- Nursing Care Management of Client With Hypokalemia ACTUAL 1Document4 pagesNursing Care Management of Client With Hypokalemia ACTUAL 1Angel Nieto PengsonNo ratings yet
- Nursing Care PlanDocument1 pageNursing Care Planlaehaaa67% (3)
- Investigatory Project On AnalgesicsDocument30 pagesInvestigatory Project On AnalgesicsAnurag Singh100% (1)
- Core Procedures - Guidance For Assessors and Foundation DoctorsDocument10 pagesCore Procedures - Guidance For Assessors and Foundation DoctorsadybutucNo ratings yet
- DehydrationDocument10 pagesDehydrationAbdelrahman M. AlnweiriNo ratings yet