Download as pdf or txt
You might also like
- 04.electrical Burn - Pre 3Document44 pages04.electrical Burn - Pre 3Jufrialdy Aldy88% (8)
- Electrical Safety HazardDocument73 pagesElectrical Safety Hazardanpuselvi125100% (2)
- Electrical Injury: By: Mohd Khairul Izzati OmarDocument28 pagesElectrical Injury: By: Mohd Khairul Izzati OmarInsyirah QalbiNo ratings yet
- Phemo Electrical InjuriesDocument54 pagesPhemo Electrical InjuriesFeny DamayantiNo ratings yet
- SCGH ED CME 23/7/15 Leesa EquidDocument43 pagesSCGH ED CME 23/7/15 Leesa EquidEvelyn RileyNo ratings yet
- ElectrocutionDocument4 pagesElectrocutionVijayakanth VijayakumarNo ratings yet
- Electrical BurnsDocument28 pagesElectrical BurnsFrancis OkwerekwuNo ratings yet
- Diathermy in SurgeryDocument31 pagesDiathermy in Surgeryrosybash100% (1)
- Electric InjuryDocument27 pagesElectric InjuryHusam ShawagfehNo ratings yet
- Electrical BurnsDocument27 pagesElectrical BurnsGautam KalraNo ratings yet
- Element 11 - ElectricityDocument22 pagesElement 11 - ElectricityJaveria FatimaNo ratings yet
- Electrical InjuriesDocument5 pagesElectrical InjuriesIrish Alyssa Kurishan UgayNo ratings yet
- Electrical InjuriesDocument12 pagesElectrical InjuriesIlyes FerenczNo ratings yet
- ANESKEY-Lightning and Electrical InjuriesDocument7 pagesANESKEY-Lightning and Electrical InjuriesJOSE LUIS FALCON CHAVEZNo ratings yet
- Types of EarthingDocument6 pagesTypes of Earthingvibhu_vermaNo ratings yet
- Electrical InjuryDocument33 pagesElectrical InjuryShazrul FaezNo ratings yet
- EsuDocument111 pagesEsuMuhammad Adryan LagitoNo ratings yet
- Electrical Injury and LightningDocument28 pagesElectrical Injury and LightningVasanth MeyNo ratings yet
- Luka Listrik: Electrical InjuryDocument37 pagesLuka Listrik: Electrical InjuryRendy SusantoNo ratings yet
- 01 B - CurrentsDocument29 pages01 B - CurrentsMeme MemeNo ratings yet
- SOPs HVDocument38 pagesSOPs HVshahidNo ratings yet
- CauterizationDocument34 pagesCauterizationBABANG GAGAHNo ratings yet
- Electrical Injuries (Electrocution)Document19 pagesElectrical Injuries (Electrocution)Habebt MusabNo ratings yet
- Electrical System of The BodyDocument11 pagesElectrical System of The BodyPyay Lin ThantNo ratings yet
- Spinal TraumaDocument47 pagesSpinal TraumadeepaNo ratings yet
- Medical Electrical SafetyDocument104 pagesMedical Electrical SafetyishoneyNo ratings yet
- Ch. 1Document18 pagesCh. 1Ahmed MohamedNo ratings yet
- 8 - Reconsructive Surgery Pt&Ot 2023-2024Document41 pages8 - Reconsructive Surgery Pt&Ot 2023-2024MUGISHA GratienNo ratings yet
- Hazards of Electricity: 1.1 Glossary Arc (Electric)Document21 pagesHazards of Electricity: 1.1 Glossary Arc (Electric)shani mughalNo ratings yet
- Electrical Safety of Medical Equipment: Bio-Medical Department Mahkota Medical Centre (Unedited..yet)Document52 pagesElectrical Safety of Medical Equipment: Bio-Medical Department Mahkota Medical Centre (Unedited..yet)Saleha AzizNo ratings yet
- Lec5 PDFDocument73 pagesLec5 PDFvenkatesh801No ratings yet
- Orthopedic EmergencyDocument94 pagesOrthopedic EmergencyZenith100% (1)
- Lecture - Electrocution and Lightning USJ FinalDocument58 pagesLecture - Electrocution and Lightning USJ FinalAde Darmawan100% (1)
- Elect EvaluationDocument11 pagesElect Evaluationapi-287081563No ratings yet
- Electric Burn Case PresentationDocument58 pagesElectric Burn Case PresentationAhmed AttiaNo ratings yet
- Electrical Hazards DMLatonioDocument71 pagesElectrical Hazards DMLatonioFarooqNo ratings yet
- Electrical InjuryDocument5 pagesElectrical InjuryCandilicious10No ratings yet
- Elecrtic Shock PresentationDocument58 pagesElecrtic Shock PresentationEuclid SantiagoNo ratings yet
- ElectrotherapyDocument78 pagesElectrotherapyManibhadra PandaNo ratings yet
- Lecture Notes 17 - Electrical Safety of Medical EquipmentDocument4 pagesLecture Notes 17 - Electrical Safety of Medical Equipmentnramanathan1No ratings yet
- Beee PPT 1Document19 pagesBeee PPT 1PreethikaaNo ratings yet
- Orthopedic Emergency EnglishDocument64 pagesOrthopedic Emergency EnglishmegaNo ratings yet
- 20.classification of CurrentsDocument21 pages20.classification of CurrentsKainat MasoodNo ratings yet
- Introduction To Electro TherapyDocument55 pagesIntroduction To Electro TherapyHema Malani Murthi82% (11)
- Sss Orthopedicemergencies 2012 Final Samuel-WongDocument38 pagesSss Orthopedicemergencies 2012 Final Samuel-WongMuhammad Irham FananiNo ratings yet
- Evoked PotentialsDocument49 pagesEvoked PotentialsparuNo ratings yet
- Electrical SafetyDocument21 pagesElectrical SafetyNobody NobodyNo ratings yet
- Appendix E - Electrical Shock and Injuries: A. "Simply Shocking" July 2001 Chevron Shipping Safety BulletinDocument2 pagesAppendix E - Electrical Shock and Injuries: A. "Simply Shocking" July 2001 Chevron Shipping Safety BulletinRol2No ratings yet
- Refresher Course Oisd-154 Electrical SafetyDocument12 pagesRefresher Course Oisd-154 Electrical Safetysonn1729No ratings yet
- Physical Injuries or Death by LIGHTNING AND ELECTRICITY PDFDocument2 pagesPhysical Injuries or Death by LIGHTNING AND ELECTRICITY PDFVincent De Vera100% (1)
- 18 - First Aid in Electrical InjuriesDocument39 pages18 - First Aid in Electrical InjuriesIsael sierraNo ratings yet
- Electric Shock: Presented By: Jignasha PatelDocument22 pagesElectric Shock: Presented By: Jignasha PatelBhargavNo ratings yet
- Electrical FatalitiesDocument12 pagesElectrical FatalitiesSárközi TiborNo ratings yet
- ElectrosurgeryDocument30 pagesElectrosurgeryKevoh MweuNo ratings yet
- PATHO-202: Submitted To:-Dr. Imtiaz Ahmed KhanDocument4 pagesPATHO-202: Submitted To:-Dr. Imtiaz Ahmed KhanAltaf HusainNo ratings yet
- Guidance For Emergency Medical Management of Electrical InjuriesDocument7 pagesGuidance For Emergency Medical Management of Electrical InjuriesNurul HudaNo ratings yet
- 1 - Electrical Safety ManagementDocument90 pages1 - Electrical Safety ManagementMohammad Hassan JawedNo ratings yet
- EKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXFrom EverandEKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXRating: 5 out of 5 stars5/5 (2)
- Electronics Troubleshooting Ilt Switches/Sensors/Solenoids: Global Manpower DevelopmentDocument28 pagesElectronics Troubleshooting Ilt Switches/Sensors/Solenoids: Global Manpower DevelopmentaimerNo ratings yet
- Find The Thévenin Equivalent With Respect To The 7k Ohm ResistorDocument27 pagesFind The Thévenin Equivalent With Respect To The 7k Ohm ResistorVipan SharmaNo ratings yet
- Practical - 2 - Resistance - Metre BridgeDocument3 pagesPractical - 2 - Resistance - Metre BridgeNitin SinghNo ratings yet
- Manual Hioki 3287 3288 3288-20Document2 pagesManual Hioki 3287 3288 3288-20Ing Kemberly OrdosgoittyNo ratings yet
- Nepal Electricity AthorityDocument22 pagesNepal Electricity AthorityShubham BaderiyaNo ratings yet
- Exercise (S) : R L, R C L, RDocument19 pagesExercise (S) : R L, R C L, RTausif RazaNo ratings yet
- D2656-13 Standard Specification For Crosslinked Polyethylene Insulation For Wire and Cable Rated 2001 To 35 000 VDocument3 pagesD2656-13 Standard Specification For Crosslinked Polyethylene Insulation For Wire and Cable Rated 2001 To 35 000 Vastewayb_964354182No ratings yet
- Current ElectricityDocument3 pagesCurrent ElectricityWild RaptorNo ratings yet
- Insulation ResistanceDocument22 pagesInsulation Resistancewikyarif100% (6)
- CIGRE 2018: 21, Rue D'artois, F-75008 PARISDocument14 pagesCIGRE 2018: 21, Rue D'artois, F-75008 PARISemilio26aNo ratings yet
- TP PDFDocument68 pagesTP PDFSanjana S NairNo ratings yet
- Earth Pit BasicsDocument16 pagesEarth Pit Basicscapluk100% (3)
- Electrical Power Cables - Part 1: ELEC9712 High Voltage SystemsDocument44 pagesElectrical Power Cables - Part 1: ELEC9712 High Voltage SystemscuntNo ratings yet
- Measurement & ControlDocument5 pagesMeasurement & ControlAsif PatelNo ratings yet
- Safecable LHD: Cut SheetDocument2 pagesSafecable LHD: Cut SheetMayraNo ratings yet
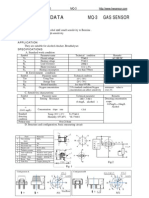
- MQ 3Document2 pagesMQ 3Farshad yazdiNo ratings yet
- APP 751A: SEL-751A Feeder Protection RelayDocument5 pagesAPP 751A: SEL-751A Feeder Protection RelayBouazzaNo ratings yet
- Topic 3 Alternating Current Circuits I PDFDocument20 pagesTopic 3 Alternating Current Circuits I PDFFeddy Blaiz100% (1)
- EEE-121 Electric Circuit Analysis I: Experimental Verification of Ohm's Law, Simulation Software (LTSPICE/circuit Maker)Document16 pagesEEE-121 Electric Circuit Analysis I: Experimental Verification of Ohm's Law, Simulation Software (LTSPICE/circuit Maker)iamneonkingNo ratings yet
- Codigos de ErroresDocument31 pagesCodigos de ErroresItseed CorcaNo ratings yet
- Chapter 1 and 2 Kamel PDFDocument93 pagesChapter 1 and 2 Kamel PDFAdel AtawiNo ratings yet
- Transformer Oil&DgaDocument70 pagesTransformer Oil&DgaBasudev Patra100% (1)
- PhysicsDocument6 pagesPhysicsFarhan KhalidNo ratings yet
- Future MOSFET Devices Using High-K (TiO2) DielectricDocument6 pagesFuture MOSFET Devices Using High-K (TiO2) DielectricIJRASETPublicationsNo ratings yet
- 3 Phase Ac Problems With SolutionDocument12 pages3 Phase Ac Problems With SolutionKim FetalverNo ratings yet
- THERMISTORDocument17 pagesTHERMISTORJaymar Abapo LumasagNo ratings yet
- Problem StatementDocument11 pagesProblem StatementprathameshNo ratings yet
- Grade 8 Q1 Week 5-7 LAW ValidatedDocument8 pagesGrade 8 Q1 Week 5-7 LAW ValidatedGINALYNROSE ROSIQUENo ratings yet
- Led Taxi Light TestingDocument2 pagesLed Taxi Light Testingajaydce05No ratings yet
- Generator TestDocument20 pagesGenerator TestElias GabrielNo ratings yet