Download as pdf or txt
You might also like
- Photon Benefits 2022 (August)Document7 pagesPhoton Benefits 2022 (August)sojithesouljaNo ratings yet
- Malta Visa Application Centre, COCHIN Appointment LetterDocument4 pagesMalta Visa Application Centre, COCHIN Appointment LetterRamnas m.j0% (1)
- 2017 Anthem GHIP Benefits Booklet (Final)Document119 pages2017 Anthem GHIP Benefits Booklet (Final)Alexander NewberryNo ratings yet
- BCBS Enrollment GuideDocument6 pagesBCBS Enrollment GuideAnonymous Lri40PrlkNo ratings yet
- Us Apple Plus Ppo Feb2019 en 1Document3 pagesUs Apple Plus Ppo Feb2019 en 1Lucas Coleta AlmeidaNo ratings yet
- 2 VEBA Plan ComparisonDocument2 pages2 VEBA Plan ComparisonMitchell BigleyNo ratings yet
- USS Pre-Medicare PPO With RX PlanDocument3 pagesUSS Pre-Medicare PPO With RX PlanAnonymous w0egAgMouGNo ratings yet
- Act Ch09 l04 EnglishDocument3 pagesAct Ch09 l04 Englishaubrymichalllllllllll44No ratings yet
- Cigna OAP 0 Summary 1020Document12 pagesCigna OAP 0 Summary 1020santiagomNo ratings yet
- Benefits DocumentDocument11 pagesBenefits DocumentAndrew VlackNo ratings yet
- CAMAF Benefit Brochure 2014Document2 pagesCAMAF Benefit Brochure 20140796105632No ratings yet
- Care AdvantageDocument26 pagesCare AdvantageVipul KumarNo ratings yet
- Blueoptimum Plus Ppo Plan: Benefit SummaryDocument4 pagesBlueoptimum Plus Ppo Plan: Benefit Summarylooksmart111No ratings yet
- Vanderbilt phf-21-22Document2 pagesVanderbilt phf-21-22api-458468763No ratings yet
- Benefits Overview 2018Document5 pagesBenefits Overview 2018Joby JoNo ratings yet
- Standard Schedule of Benefits - Market Street LTD 2022Document2 pagesStandard Schedule of Benefits - Market Street LTD 2022mariojesus8807No ratings yet
- Shape B: Schedule of BenefitsDocument6 pagesShape B: Schedule of BenefitsRana GreeneNo ratings yet
- Patriot America Plus: Certificate of InsuranceDocument35 pagesPatriot America Plus: Certificate of InsuranceNavidadNo ratings yet
- 2023 FMCNA Medical Plan Cost ComparisonDocument2 pages2023 FMCNA Medical Plan Cost ComparisonCristal PeoplesNo ratings yet
- KP - Plan Summary Medical - PPODocument3 pagesKP - Plan Summary Medical - PPOshanegbaker51No ratings yet
- Select PlanDocument3 pagesSelect PlanLuis EscobarNo ratings yet
- 2022 Patriot America Plus PATAP PGTAPDocument37 pages2022 Patriot America Plus PATAP PGTAPmaNo ratings yet
- Summary of Benefits: Plan Highlights In-Network Out-of-NetworkDocument19 pagesSummary of Benefits: Plan Highlights In-Network Out-of-NetworkclassicalgasNo ratings yet
- DIANins Blue 100 Policy Terms Conditions V2 2023 2024Document47 pagesDIANins Blue 100 Policy Terms Conditions V2 2023 2024suritrue9644No ratings yet
- Lewermark Health Insurance Copay Plan For Delta State UniversityDocument3 pagesLewermark Health Insurance Copay Plan For Delta State Universityroby sorianoNo ratings yet
- BCBS Health Star Benefits SummaryDocument10 pagesBCBS Health Star Benefits SummaryCandice CobbNo ratings yet
- Snap Guardian Dental Plan Summary 2022Document4 pagesSnap Guardian Dental Plan Summary 2022Samson FungNo ratings yet
- Blue-Cross-Premier-Platinum-Extra-Dental-Vision CareerDocument8 pagesBlue-Cross-Premier-Platinum-Extra-Dental-Vision Careerapi-248930594No ratings yet
- Barbados NemCare Individuals Health InsuranceDocument3 pagesBarbados NemCare Individuals Health InsuranceKammieNo ratings yet
- Sbi General'S Retail Health Insurance Policy: Ensure Your Family's HappinessDocument12 pagesSbi General'S Retail Health Insurance Policy: Ensure Your Family's HappinessYOGESHNo ratings yet
- Silver DXB 0% (120923)Document7 pagesSilver DXB 0% (120923)arasakumar_mNo ratings yet
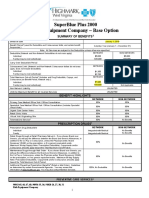
- Rish Equipment Base Plan Option Eff. 1.1.2019Document4 pagesRish Equipment Base Plan Option Eff. 1.1.2019michala anthonyNo ratings yet
- Jo Say 2020 QuotesDocument6 pagesJo Say 2020 QuotessebastianNo ratings yet
- Uhc Aawa24lp0123163 000 H1278028000 SB 21082023 030634 2024 SF20230921Document15 pagesUhc Aawa24lp0123163 000 H1278028000 SB 21082023 030634 2024 SF20230921kevin.mccreaNo ratings yet
- 2017 Anthem GHIP Benefits Booklet (Final)Document119 pages2017 Anthem GHIP Benefits Booklet (Final)Alexander NewberryNo ratings yet
- Thomas PPO Thomas HMO Claire EPO Claire HMO: in Network. in NetworkDocument1 pageThomas PPO Thomas HMO Claire EPO Claire HMO: in Network. in Networkanas fassiNo ratings yet
- InsuracneDocument4 pagesInsuracnesathishbabuNo ratings yet
- Ben Sum - LocalPlus IN Plan - 04.01.2023 - GreenWaste Recovery, LLC - 3341739 - 2023-03-06T19 - 39 - 33Document16 pagesBen Sum - LocalPlus IN Plan - 04.01.2023 - GreenWaste Recovery, LLC - 3341739 - 2023-03-06T19 - 39 - 33Romina AstridNo ratings yet
- Employee Benefits-Wellness Guide 2023-24Document30 pagesEmployee Benefits-Wellness Guide 2023-24shanzeh2609No ratings yet
- HP Benefits 1104 1Document6 pagesHP Benefits 1104 1Anu Raj Anu RajNo ratings yet
- Northeastern University Student Health Plan: Blue Care Elect Preferred (PPO)Document4 pagesNortheastern University Student Health Plan: Blue Care Elect Preferred (PPO)agdayemNo ratings yet
- NntfilesMyNASAdminSetupPolicySetupPayer567MContract410440Product866AttachmentsCAT B 9c360102 4d1f 4e73 Acb3 F03e5176e4a0Document8 pagesNntfilesMyNASAdminSetupPolicySetupPayer567MContract410440Product866AttachmentsCAT B 9c360102 4d1f 4e73 Acb3 F03e5176e4a0syedjabeenhussainNo ratings yet
- International Student Health Certificate Individual CoverageDocument40 pagesInternational Student Health Certificate Individual CoverageJialun ZhuNo ratings yet
- Participant DocumentsDocument8 pagesParticipant DocumentsSergiu EniNo ratings yet
- Benefits HighlightsDocument1 pageBenefits HighlightsRobert AvramescuNo ratings yet
- Van Wagner Medical Plans 2013Document1 pageVan Wagner Medical Plans 2013res6250No ratings yet
- Star Health Gain - 20Document2 pagesStar Health Gain - 20Rajiv GandhiNo ratings yet
- Gold Plus DXB 20% (120923)Document7 pagesGold Plus DXB 20% (120923)ccmms6yngfNo ratings yet
- United Healthcare CA Select Plus Silver 30 2000 30 Aksa W 405Document8 pagesUnited Healthcare CA Select Plus Silver 30 2000 30 Aksa W 405zxcvNo ratings yet
- Studentsecure: Pursuing Your Education Outside Your Home Country?Document6 pagesStudentsecure: Pursuing Your Education Outside Your Home Country?Importaciones Zhong WenNo ratings yet
- 2010 UnitedHealthcare Benefits SummaryDocument1 page2010 UnitedHealthcare Benefits Summaryapi-27017317No ratings yet
- L2-Care Smart SelectDocument12 pagesL2-Care Smart SelectDeepak BansodeNo ratings yet
- Management Science Associates SpdsDocument64 pagesManagement Science Associates SpdsAshwinNo ratings yet
- VEBA Plan PresentationDocument19 pagesVEBA Plan PresentationMitchell BigleyNo ratings yet
- Cotización de Póliza de Salud en PanamaDocument4 pagesCotización de Póliza de Salud en PanamacuentasygastosdecasaNo ratings yet
- Core BronzeDocument4 pagesCore BronzeMohit MarwahNo ratings yet
- Photon Benefits Summary - Jan 2024Document12 pagesPhoton Benefits Summary - Jan 2024Saravanan MuniandiNo ratings yet
- Medical Insurance Eligibility Verification - The Comprehensive GuideFrom EverandMedical Insurance Eligibility Verification - The Comprehensive GuideNo ratings yet
- Sulfonamides, Trimethoprim, & Quinolones: Camille E. Beauduy, Pharmd, & Lisa G. Winston, MDDocument15 pagesSulfonamides, Trimethoprim, & Quinolones: Camille E. Beauduy, Pharmd, & Lisa G. Winston, MDRegine Coeli Menta LansanganNo ratings yet
- Molar Pregnancy: Presented byDocument87 pagesMolar Pregnancy: Presented bysanjay kashyapNo ratings yet
- Acute Mesenteric IschemiaDocument46 pagesAcute Mesenteric Ischemiashita febrianaNo ratings yet
- Theory Critique NursingDocument4 pagesTheory Critique NursingLowellaJulioNo ratings yet
- GEMD Safety Health PolicyDocument2 pagesGEMD Safety Health PolicyetaNo ratings yet
- Cutaneous Disorders of PregnancyDocument134 pagesCutaneous Disorders of Pregnancyabdul qayyumNo ratings yet
- Epilepsy MCQDocument7 pagesEpilepsy MCQko naythweNo ratings yet
- Working As A Doctor in Australia 4Document8 pagesWorking As A Doctor in Australia 4Samir RashadNo ratings yet
- How Social Media Impacts The Mental Health of Grade 10 Junior High School StudentsDocument2 pagesHow Social Media Impacts The Mental Health of Grade 10 Junior High School StudentsRegor Salvador ArboNo ratings yet
- Megan Frano Current ResumeDocument1 pageMegan Frano Current Resumeapi-544878035No ratings yet
- Assignment 1Document3 pagesAssignment 1SaulNo ratings yet
- Chess and NutritionDocument6 pagesChess and NutritionAnonymous pTZCrF7No ratings yet
- InsulinaDocument1 pageInsulinaRICARDO DEL ANGEL HERNANDEZNo ratings yet
- Comorbidity Between ADHD and Anxiety Disorders Across The LifespanDocument8 pagesComorbidity Between ADHD and Anxiety Disorders Across The LifespanRubíPeñaNo ratings yet
- Curriculum Vitae For Kimberly P. Lindsey, PHDDocument14 pagesCurriculum Vitae For Kimberly P. Lindsey, PHDKimLindseyNo ratings yet
- Þ" Hospital: Clinical and Scientific Rationale For The "MATH Treatment Protocol For COVID-19Document22 pagesÞ" Hospital: Clinical and Scientific Rationale For The "MATH Treatment Protocol For COVID-19Doménica SánchezNo ratings yet
- Depression Theory, AssessmentDocument11 pagesDepression Theory, Assessmentdiana nistoranNo ratings yet
- Week 1 - Principles of Pre Operative CareDocument25 pagesWeek 1 - Principles of Pre Operative Carechantlex3No ratings yet
- People Risk Infographics MercerDocument1 pagePeople Risk Infographics MercerChanakya NitiNo ratings yet
- Handbook of Musculoskeletal Pain in The WorkplaceDocument511 pagesHandbook of Musculoskeletal Pain in The WorkplaceJorge MartinsNo ratings yet
- Article 1646033027Document4 pagesArticle 1646033027DrHarikrishnan MeenakshisundaramNo ratings yet
- Abstract Presentations - Australian Physiotherapy Association (PDFDrive)Document160 pagesAbstract Presentations - Australian Physiotherapy Association (PDFDrive)thilsen_abi8303No ratings yet
- Community Invitation LetterDocument2 pagesCommunity Invitation Letterandersmag100% (1)
- Project 1 Personal Prescription Paper Final Submission 1Document5 pagesProject 1 Personal Prescription Paper Final Submission 1api-734716578No ratings yet
- Occupational Health ObjectivesDocument1 pageOccupational Health Objectivesbook1manNo ratings yet
- Anemia in Adolescent College Girls: Effect of Age, Nutritional Status and Nutrient IntakeDocument4 pagesAnemia in Adolescent College Girls: Effect of Age, Nutritional Status and Nutrient IntakeErinda ChuzaifahNo ratings yet
- NCM 107 HandoutsDocument18 pagesNCM 107 HandoutsGeneva Amandy Roxas50% (2)
- Care Plan TemplateDocument7 pagesCare Plan TemplateMayraPagan-CarmenattyNo ratings yet
- Grammar Expressing Large and Small DifferencesDocument1 pageGrammar Expressing Large and Small Differences丁tingNo ratings yet