Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Profile For Females: Conners' Parent Rating Scale-Revised (S)Document2 pagesProfile For Females: Conners' Parent Rating Scale-Revised (S)Claudya Abarca56% (9)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Argumentative Essay 4 VaccinesDocument9 pagesArgumentative Essay 4 Vaccinesapi-30225964750% (8)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 1001 Great Ideas For Teaching and Raising Children With Autism or Asperger's - Ellen Notbohm, Veronica ZyskDocument1,312 pages1001 Great Ideas For Teaching and Raising Children With Autism or Asperger's - Ellen Notbohm, Veronica ZyskTijana Brzić0% (1)
- What Your Doctor May Not Tell You About Children's VaccinationsDocument332 pagesWhat Your Doctor May Not Tell You About Children's VaccinationsConventionalThinker100% (11)
- Iseasemanagement/allergy/rhino-Sinusitis/: PublisDocument13 pagesIseasemanagement/allergy/rhino-Sinusitis/: PublisAnonymous 65zjdAVNo ratings yet
- Output Hasil Analisa DataDocument7 pagesOutput Hasil Analisa DataAnonymous 65zjdAVNo ratings yet
- Erythema Nodosum Clinical Presentation - History, Physical, CausesDocument4 pagesErythema Nodosum Clinical Presentation - History, Physical, CausesAnonymous 65zjdAVNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaAnonymous 65zjdAVNo ratings yet
- Oneway: ONEWAY Presentasi BY Perlakuan /plot Means /missing Analysis /POSTHOC TUKEY ALPHA (0.05)Document4 pagesOneway: ONEWAY Presentasi BY Perlakuan /plot Means /missing Analysis /POSTHOC TUKEY ALPHA (0.05)Anonymous 65zjdAVNo ratings yet
- Trends in The Prevalence of Cerebral Palsy in A Population-Based StudyDocument8 pagesTrends in The Prevalence of Cerebral Palsy in A Population-Based StudyAnonymous 65zjdAVNo ratings yet
- Trends in The Prevalence of Cerebral Palsy in A Population-Based StudyDocument8 pagesTrends in The Prevalence of Cerebral Palsy in A Population-Based StudyAnonymous 65zjdAVNo ratings yet
- Manus FracturesDocument25 pagesManus FracturesAnonymous 65zjdAVNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaAnonymous 65zjdAVNo ratings yet
- Atlas of Pediatric Surgical DiseasesDocument30 pagesAtlas of Pediatric Surgical DiseasesMuhammad Bilal MirzaNo ratings yet
- Eviceration Enoculation ExenterationDocument9 pagesEviceration Enoculation ExenterationAnonymous 65zjdAVNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaAnonymous 65zjdAVNo ratings yet
- Neural TubeDocument1 pageNeural TubeAnonymous 65zjdAVNo ratings yet
- JurnalDocument5 pagesJurnalAnonymous 65zjdAVNo ratings yet
- Calculating Vaccine NeedsDocument3 pagesCalculating Vaccine NeedsPEDRO M. MAGADAN67% (3)
- AkhtarDocument1 pageAkhtarMukesh MistriNo ratings yet
- Vaccine Manufacturers IndiaDocument6 pagesVaccine Manufacturers Indiayash shahNo ratings yet
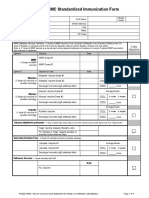
- VSLO Immunization Form - Fillable PDF - 1.8.2021Document4 pagesVSLO Immunization Form - Fillable PDF - 1.8.2021Yazeed QadadhaNo ratings yet
- MMR Vaccine: Review of Benefits and RisksDocument6 pagesMMR Vaccine: Review of Benefits and RisksAldo Pravando JulianNo ratings yet
- Vaccine InfographicDocument13 pagesVaccine Infographicapi-317908084No ratings yet
- Prinsipal: PT. Biofarma: Pt. Merapi Utama Pharma Daftar Harga Berlaku: 4 Januari 2021Document3 pagesPrinsipal: PT. Biofarma: Pt. Merapi Utama Pharma Daftar Harga Berlaku: 4 Januari 2021AtmaNo ratings yet
- Immunisation Card 1Document3 pagesImmunisation Card 1ShuvajoyyyNo ratings yet
- 2019 Guide For ImmunizationDocument195 pages2019 Guide For ImmunizationReigner paul DavidNo ratings yet
- Adult Combined ScheduleDocument6 pagesAdult Combined SchedulesharvaniNo ratings yet
- Immunization Policy Guidline - Kenya 2013Document72 pagesImmunization Policy Guidline - Kenya 2013okwadha simionNo ratings yet
- School Based Immunization Form Grade 1Document1 pageSchool Based Immunization Form Grade 1maristellaNo ratings yet
- Epi and ImmunizationsDocument66 pagesEpi and ImmunizationsreadmeamllionNo ratings yet
- AAEP Core Vaccinations For Adult HorsesDocument1 pageAAEP Core Vaccinations For Adult HorsesLauren ThompsonNo ratings yet
- استراتيجيات التربية الخاصةDocument44 pagesاستراتيجيات التربية الخاصةNoha EldershawyNo ratings yet
- Types of VaccinesDocument3 pagesTypes of VaccinesKhairul ZakirahNo ratings yet
- Baby Immunization ScheduleDocument1 pageBaby Immunization Schedulesunil kalaNo ratings yet
- References Mayenine - 092640Document5 pagesReferences Mayenine - 092640Lambert FonyuyNo ratings yet
- EpiDocument5 pagesEpiMarie Dinah SalvinoNo ratings yet
- CHN Immunization NotesDocument9 pagesCHN Immunization NotesJustin AncogNo ratings yet
- Revised Catalise 2017Document4 pagesRevised Catalise 2017Carolina UrrutiaNo ratings yet
- Rationalization of AWC Wcdpo SiwanDocument17 pagesRationalization of AWC Wcdpo SiwanAK ContinentalNo ratings yet
- Guidelines Updates - Plab 1 Keys-1Document2 pagesGuidelines Updates - Plab 1 Keys-1Cynthia GNo ratings yet
- Vaccine Project - FinalDocument2 pagesVaccine Project - Finalchelsea garzaNo ratings yet
- THC AspergerDocument168 pagesTHC AspergerMICHAELNo ratings yet
- Editorial: Breastmilk: It's Not Just For Breakfast Anymore!Document1 pageEditorial: Breastmilk: It's Not Just For Breakfast Anymore!lila bNo ratings yet