Download as pdf or txt
You might also like
- Arterial Blood Gas Analysis - making it easyFrom EverandArterial Blood Gas Analysis - making it easyRating: 4.5 out of 5 stars4.5/5 (4)
- Uhone Broker GuideDocument28 pagesUhone Broker Guidestech137No ratings yet
- Performance of A High-Solidity Wells Turbine For An OWC Wave Power PlantDocument6 pagesPerformance of A High-Solidity Wells Turbine For An OWC Wave Power PlantAna Elisa Rodrigues do CoutoNo ratings yet
- Acid-Base Disorder 27 July 2017 PDFDocument48 pagesAcid-Base Disorder 27 July 2017 PDFPauline ChanNo ratings yet
- 2016 Acid Base DisordersDocument48 pages2016 Acid Base DisordersbellabelbonNo ratings yet
- ABG BangaloreDocument34 pagesABG Bangaloredr.rrajesh92No ratings yet
- Abg InterpretationDocument52 pagesAbg InterpretationCirugia Cardiovascular NeivaNo ratings yet
- ABG AnalysisDocument26 pagesABG Analysisf5psw2zk6fNo ratings yet
- Arterial Blood Gas: IM 2013 (AVM)Document66 pagesArterial Blood Gas: IM 2013 (AVM)Wilsonne ChuaNo ratings yet
- Acid Base Disorders: Mr. Ahmed Alnaji Mbchb. Mrcs 1+2 Palestinian Board G. Surgery European Gaza HospitalDocument60 pagesAcid Base Disorders: Mr. Ahmed Alnaji Mbchb. Mrcs 1+2 Palestinian Board G. Surgery European Gaza Hospitalpt.mahmoudNo ratings yet
- Acid/Base Am Didactic Teaching Guide: Learning ObjectivesDocument3 pagesAcid/Base Am Didactic Teaching Guide: Learning ObjectivesAdrian CamposNo ratings yet
- Blood Gas InterpretationDocument55 pagesBlood Gas InterpretationtommyNo ratings yet
- ABGs InterpretationDocument33 pagesABGs InterpretationHamza DossaNo ratings yet
- Arterial Blood Gas Analysis: FK Uph May26, 2022Document52 pagesArterial Blood Gas Analysis: FK Uph May26, 2022FirmanHidayatNo ratings yet
- Arterial Blood GAS InterpretationDocument25 pagesArterial Blood GAS Interpretationliyahanna02No ratings yet
- Y5 RN - Abgs 27oct2010Document5 pagesY5 RN - Abgs 27oct2010Canh VanNo ratings yet
- Arterial Blood Gas: AnalysisDocument51 pagesArterial Blood Gas: Analysisnaven100% (2)
- Arterial Blood Gas - ppt1Document53 pagesArterial Blood Gas - ppt1Madhuri100% (2)
- Acid - Base BalanceDocument42 pagesAcid - Base BalancePao AliNo ratings yet
- Acid Base BalanceDocument44 pagesAcid Base BalanceKenny JapNo ratings yet
- Saumya Gupta Moderator: Dr. Vishal GuptaDocument41 pagesSaumya Gupta Moderator: Dr. Vishal Guptaimranqazi11No ratings yet
- 09 ACID BASE DisterbencesDocument28 pages09 ACID BASE DisterbencesanojNo ratings yet
- Abg PDFDocument40 pagesAbg PDFjohn ginnNo ratings yet
- Blood Gases (Abgs) Interpretation Dr/Baha Eldin Hassan Ahmed Fellow Paediatric Critical CareDocument48 pagesBlood Gases (Abgs) Interpretation Dr/Baha Eldin Hassan Ahmed Fellow Paediatric Critical Carehagir alhajNo ratings yet
- Blood Gas AnalysisDocument52 pagesBlood Gas AnalysisKresna Dharma SuryanaNo ratings yet
- Stepwise Approach To Acid-Base AnalysisDocument16 pagesStepwise Approach To Acid-Base AnalysisTryanto Amrisal MohammadNo ratings yet
- ABG MMHG InterpretationDocument92 pagesABG MMHG InterpretationManmeet SNo ratings yet
- Arterial Blood Gas Analysis: DR - Rakesh Chandra Chaurasia PGT 3 Ims, Bhu Moderator: DR - Manjaree Mishra Asset - ProfDocument64 pagesArterial Blood Gas Analysis: DR - Rakesh Chandra Chaurasia PGT 3 Ims, Bhu Moderator: DR - Manjaree Mishra Asset - ProfArmaanjeet SinghNo ratings yet
- Arterial Blood GasDocument55 pagesArterial Blood GasRathis Dasan100% (1)
- ABGDocument45 pagesABGHasan SudirgoNo ratings yet
- A Case-Based Approach To Acid-Base Disorders - J. Muir HandoutDocument69 pagesA Case-Based Approach To Acid-Base Disorders - J. Muir HandoutCloudySkyNo ratings yet
- ABG InterpretationDocument55 pagesABG Interpretationkhoja72100% (1)
- Acid - Base Balance & Abg AnalysisDocument71 pagesAcid - Base Balance & Abg AnalysisMohan KrishnaNo ratings yet
- LRP CriticalCare Sample2Document46 pagesLRP CriticalCare Sample2Aniket ChoudharyNo ratings yet
- Acid Base BalaneceDocument11 pagesAcid Base BalaneceHAMMYER ALROKHAMINo ratings yet
- Lecture 3 ABGS CardioDocument18 pagesLecture 3 ABGS CardioJawad MohammadNo ratings yet
- How To Interpret BGA (Ali Haedar)Document15 pagesHow To Interpret BGA (Ali Haedar)Bayu AkbarNo ratings yet
- ABG Algorithm PDFDocument2 pagesABG Algorithm PDFamin2014No ratings yet
- Acid Base 2013Document60 pagesAcid Base 2013Belial ZaheuerNo ratings yet
- Acid - Base BalanceDocument41 pagesAcid - Base BalanceEgun Nuel DNo ratings yet
- Maimun Zulhaidah A Tinny R Indra Clinical Pathology DeptDocument47 pagesMaimun Zulhaidah A Tinny R Indra Clinical Pathology DeptSunny AghniNo ratings yet
- Interpreting ABG - An Interative Session: Dr. Manjunath Patil Professor, Dept. of Anaesthesiology J.N.Medical CollegeDocument31 pagesInterpreting ABG - An Interative Session: Dr. Manjunath Patil Professor, Dept. of Anaesthesiology J.N.Medical CollegeMadhan Mohan Reddy KatikareddyNo ratings yet
- Abg PPT NewDocument69 pagesAbg PPT NewMalaka Atapattu100% (3)
- ABG - Manuel Antonio Ko, MD 2008Document58 pagesABG - Manuel Antonio Ko, MD 2008Nguyen Minh DucNo ratings yet
- ABG Analysis: Department of NephrologyDocument31 pagesABG Analysis: Department of NephrologyGovind GNo ratings yet
- AbgDocument7 pagesAbgChin ChanNo ratings yet
- Acid-Base Balance: Graciela Lou F. Mana-Ay, RN, ManDocument68 pagesAcid-Base Balance: Graciela Lou F. Mana-Ay, RN, ManKeshia Joyce LimNo ratings yet
- ABGAnalysis Resident LectureDocument71 pagesABGAnalysis Resident LecturePutu AdhekNo ratings yet
- DkaDocument38 pagesDkaHam SotheaNo ratings yet
- ABGS FinalDocument25 pagesABGS FinalLaraib KanwalNo ratings yet
- ABG InterpertationDocument14 pagesABG Interpertationapi-3757039100% (1)
- Arterial Blood Gas Analysis: BY-Shivam Sachan (JR Ii) Moderator - Dr. R.K YADAV (M.D)Document52 pagesArterial Blood Gas Analysis: BY-Shivam Sachan (JR Ii) Moderator - Dr. R.K YADAV (M.D)imranqazi11No ratings yet
- Blood Gas Analysis CMEDocument12 pagesBlood Gas Analysis CMEpierhot_11No ratings yet
- Arterial Blood Gases: Mike Runyon, MD July 15, 2010Document46 pagesArterial Blood Gases: Mike Runyon, MD July 15, 2010mamiraliNo ratings yet
- ArpitDocument73 pagesArpitDurgesh PushkarNo ratings yet
- "Blood Gas Analysis in A Nutshell: DR Anshuman MishraDocument28 pages"Blood Gas Analysis in A Nutshell: DR Anshuman MishraMinaz PatelNo ratings yet
- Acid Base BalanceDocument46 pagesAcid Base Balanceleesteph78No ratings yet
- Acid Base BalanceDocument45 pagesAcid Base BalanceSameer Ul BashirNo ratings yet
- Acid - Base DisordersDocument20 pagesAcid - Base DisordersDavid LadinNo ratings yet
- Metabolic Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandMetabolic Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Obtain 12 Lead ECG and Cardiology ConsultationDocument2 pagesObtain 12 Lead ECG and Cardiology ConsultationPauline ChanNo ratings yet
- Acid-Base Disorder 27 July 2017 PDFDocument48 pagesAcid-Base Disorder 27 July 2017 PDFPauline ChanNo ratings yet
- Psych Drugs Info SheetDocument4 pagesPsych Drugs Info SheetPauline ChanNo ratings yet
- Cardio Dept Elective FormDocument1 pageCardio Dept Elective FormPauline ChanNo ratings yet
- A Novel Use of Coblation in The Treatment of Subglottic StenosisDocument14 pagesA Novel Use of Coblation in The Treatment of Subglottic StenosisFabian Camelo OtorrinoNo ratings yet
- State Observer - Wikipedia, The Free EncyclopediaDocument6 pagesState Observer - Wikipedia, The Free EncyclopediaNhà Của CọpNo ratings yet
- The Earth As A PlanetDocument5 pagesThe Earth As A PlanetEgzon DalipiNo ratings yet
- Healing Sound - Contemporary Methods For Tibetan Singing BowlsDocument18 pagesHealing Sound - Contemporary Methods For Tibetan Singing Bowlsjaufrerudel0% (1)
- Life of GalileoDocument4 pagesLife of GalileoBilly AslamNo ratings yet
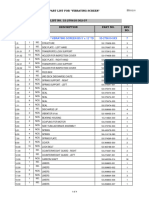
- 0 1 NO. Ga. of Vibrating Screen Bs 5' X 12' TD 53-270610-5XX 7Document4 pages0 1 NO. Ga. of Vibrating Screen Bs 5' X 12' TD 53-270610-5XX 7Benjamin MurphyNo ratings yet
- EC8491 Communication Systems - Notes 1Document138 pagesEC8491 Communication Systems - Notes 1Kaniha KNo ratings yet
- Salvation Series-Lesson5-EternallifeyourchoiceDocument3 pagesSalvation Series-Lesson5-EternallifeyourchoiceKim M. BaraquelNo ratings yet
- Level of Awarenss of Hypertension Among Grade 12 Science Technology Engineering and Mathematics Students of Systems Plus College FoundationDocument35 pagesLevel of Awarenss of Hypertension Among Grade 12 Science Technology Engineering and Mathematics Students of Systems Plus College FoundationMary Grace MendeNo ratings yet
- BoqDocument30 pagesBoqPrashant Singh Chauhan100% (1)
- Potato and Banana Chips-5481588926613949Document40 pagesPotato and Banana Chips-5481588926613949satubhosale100% (1)
- Operating Instructions: Position SwitchDocument7 pagesOperating Instructions: Position SwitchDwiMaryantoNo ratings yet
- Top 1000 Companies Details PDFDocument202 pagesTop 1000 Companies Details PDFNiladri Bhusan HarichandanNo ratings yet
- The Total Test Time Is 1 Hour. Please Beqin by Writinq Your Name BelowDocument13 pagesThe Total Test Time Is 1 Hour. Please Beqin by Writinq Your Name BelowSaci Louis NaniNo ratings yet
- General Solution For The Dynamic Modeling of Parallel RobotsDocument17 pagesGeneral Solution For The Dynamic Modeling of Parallel RobotsHuynh TLoiNo ratings yet
- Acoustic Systems in Biology - Neville H. FletcherDocument348 pagesAcoustic Systems in Biology - Neville H. FletcherJosue PazNo ratings yet
- HHT FFT DifferencesDocument8 pagesHHT FFT Differencesbubo28No ratings yet
- Online MetroCard Recharge - TutorialsDuniyaDocument36 pagesOnline MetroCard Recharge - TutorialsDuniyaGurkirat SinghNo ratings yet
- Demografi Mind MapDocument3 pagesDemografi Mind MapAnis Elina ZulkipliNo ratings yet
- Writing Handout 4-5Document9 pagesWriting Handout 4-5Rosine ZgheibNo ratings yet
- BS en 13230 Part 2-2016Document30 pagesBS en 13230 Part 2-2016jasonNo ratings yet
- BLDC Motor Test SystemsDocument12 pagesBLDC Motor Test SystemsKaung Khar100% (1)
- P e - First-Quarter-Exams 1st-SemDocument7 pagesP e - First-Quarter-Exams 1st-SemJieann BalicocoNo ratings yet
- E E E E: For Installation/s IndustrialDocument1 pageE E E E: For Installation/s IndustrialRJ Padilla0% (1)
- Introduction To Culinary ArtsDocument10 pagesIntroduction To Culinary ArtsNico Urieta De AdeNo ratings yet
- 3492 0022 01 - LDocument16 pages3492 0022 01 - LJoe SmithNo ratings yet
- Optimal Solution Using MODI - MailDocument17 pagesOptimal Solution Using MODI - MailIshita RaiNo ratings yet
- Earth and Life Science ADM 21-30 ReviewerDocument10 pagesEarth and Life Science ADM 21-30 ReviewerABEGAEL ARINDAENGNo ratings yet