Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Interpretation of Arterial Blood Gases (ABGs)Document6 pagesInterpretation of Arterial Blood Gases (ABGs)afalfitraNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
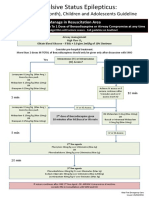
- Status Epilepticus A3v2Document1 pageStatus Epilepticus A3v2afalfitraNo ratings yet
- Experimental NeurologyDocument12 pagesExperimental NeurologyafalfitraNo ratings yet
- EAbara How To Write A Case ReportDocument19 pagesEAbara How To Write A Case ReportafalfitraNo ratings yet
- Zhao 2015Document6 pagesZhao 2015afalfitraNo ratings yet
- Grade 10 - Life Science - November Paper 1 - MemoDocument8 pagesGrade 10 - Life Science - November Paper 1 - MemoJustinCase1991No ratings yet
- Scott Werner-Divine Invocation .DNADocument1 pageScott Werner-Divine Invocation .DNAYoel SNo ratings yet
- Klinik For Manuel Medicin05bDocument4 pagesKlinik For Manuel Medicin05bFerris BuhlerNo ratings yet
- What Is A CellDocument2 pagesWhat Is A CellJocelinyenNo ratings yet
- Anatomy and Biomechanics of SpineDocument53 pagesAnatomy and Biomechanics of SpineSUYASH TIMALSINANo ratings yet
- CH 32 Gallbladder and Extrahepatic Biliary SystemDocument33 pagesCH 32 Gallbladder and Extrahepatic Biliary SystemElisha BernabeNo ratings yet
- Veterinary Neuropharmacology VPT 321 Lecture Notes TANUVASDocument101 pagesVeterinary Neuropharmacology VPT 321 Lecture Notes TANUVASSunil89% (18)
- Simple Squamous and Pseudo EpitheliumDocument2 pagesSimple Squamous and Pseudo EpitheliumveniceNo ratings yet
- Examination of The Soft Tissues of The ChestDocument8 pagesExamination of The Soft Tissues of The ChestDum MyNo ratings yet
- Struktur Morfologi Dan Anatomi Burung Endemik Sulawesi Cabai Panggul-Kelabu (Dicaeum Celebicum Műller, 1843)Document7 pagesStruktur Morfologi Dan Anatomi Burung Endemik Sulawesi Cabai Panggul-Kelabu (Dicaeum Celebicum Műller, 1843)SaadatulNo ratings yet
- Digestive System IDocument15 pagesDigestive System IElena Arvaniti100% (1)
- Course OutlineDocument4 pagesCourse OutlineAhmed SaeedNo ratings yet
- Lecture-28 Placenta PreviaDocument43 pagesLecture-28 Placenta PreviaMadhu Sudhan Pandeya100% (1)
- Oncology Nursing-2 PDFDocument22 pagesOncology Nursing-2 PDFHebsiba PonnayyanNo ratings yet
- CHP 11Document71 pagesCHP 11Sophia YounNo ratings yet
- Trigeminal Nerve FinalDocument101 pagesTrigeminal Nerve FinalShraddha PatilNo ratings yet
- Lecture 09,10 - Foundations of USG PDFDocument78 pagesLecture 09,10 - Foundations of USG PDFWaqas SaeedNo ratings yet
- p8 The Physiology of The Flocculonodular LobeDocument16 pagesp8 The Physiology of The Flocculonodular LobeHomeground entertainmentNo ratings yet
- VC MT Histology Lecture Compilation 2018Document72 pagesVC MT Histology Lecture Compilation 2018ivan domingoNo ratings yet
- Anatomy and Physiology of The Skin.3Document11 pagesAnatomy and Physiology of The Skin.3alinaNo ratings yet
- Autoimmunity: Ii Mbbs Dr. Sudheer KherDocument29 pagesAutoimmunity: Ii Mbbs Dr. Sudheer KherAbdiladif Ahmed MohamedNo ratings yet
- Blood and Immunity: By: Arian G. Himoc & Angelo H. JaraDocument37 pagesBlood and Immunity: By: Arian G. Himoc & Angelo H. JaraPapyrusNo ratings yet
- Pathology: Disaggregation of Granular and Fibrillar Elements of The Nucleus 5-HETE, N-Formylated Peptides (Formyl-Methyl)Document12 pagesPathology: Disaggregation of Granular and Fibrillar Elements of The Nucleus 5-HETE, N-Formylated Peptides (Formyl-Methyl)Sweta DabhiNo ratings yet
- Report of Nerves TissueDocument20 pagesReport of Nerves Tissuerheny_greenNo ratings yet
- Bone Grafting and Bone Graft SubstitutesDocument41 pagesBone Grafting and Bone Graft SubstitutesKiyasweet HaniNo ratings yet
- Review Aluminum: Impacts and DiseaseDocument15 pagesReview Aluminum: Impacts and DiseaseYuvraj ChaudharyNo ratings yet
- Anatomy MCQDocument10 pagesAnatomy MCQnistaraNo ratings yet
- Joyce Y. Visitacion NCM 104 Bsn-4Aj SY 2008-2009 Musculoskeletal SystemDocument33 pagesJoyce Y. Visitacion NCM 104 Bsn-4Aj SY 2008-2009 Musculoskeletal Systemyawdle100% (6)
- COMPREHENSIVE Anatomical TerminologyDocument32 pagesCOMPREHENSIVE Anatomical TerminologyKavita MahaseNo ratings yet
- CalligraphyDocument1 pageCalligraphyAlejandra LopezNo ratings yet