
Br. J. Anaesth.-2014-Lamb-242-9
Br. J. Anaesth.-2014-Lamb-242-9
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Working Capital Simulation: Managing Growth V2Document5 pagesWorking Capital Simulation: Managing Growth V2Abdul Qader100% (6)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Risk Assessment For Installation of BMS M Tower PDFDocument15 pagesRisk Assessment For Installation of BMS M Tower PDFAndrew HivNo ratings yet
- 13 Japan Under The ShogunDocument22 pages13 Japan Under The Shogunapi-29949541290% (10)
- DOC571RevC AesculapNeedleComparisonChart 3 FoldBrochureDocument2 pagesDOC571RevC AesculapNeedleComparisonChart 3 FoldBrochureMuhammad SaadNo ratings yet
- Spleenomegaly & Hypersplenism Etiology Pathogenesis and Surgical ManagementDocument53 pagesSpleenomegaly & Hypersplenism Etiology Pathogenesis and Surgical ManagementMuhammad SaadNo ratings yet
- Residency Survival Guide: Canadian Association of General Surgeons Residents CommitteeDocument53 pagesResidency Survival Guide: Canadian Association of General Surgeons Residents CommitteeIrina MincuNo ratings yet
- IndexDocument2 pagesIndexMuhammad SaadNo ratings yet
- SurgeryDocument6 pagesSurgeryMuhammad Saad100% (1)
- Therapeutic EnzymesDocument39 pagesTherapeutic EnzymesMuhammad SaadNo ratings yet
- Pain Management-PRN OrdersDocument2 pagesPain Management-PRN OrdersMuhammad SaadNo ratings yet
- Guidelines For: Continuing Medical Education (CME) / Continuing Dental Education (eDE)Document12 pagesGuidelines For: Continuing Medical Education (CME) / Continuing Dental Education (eDE)Muhammad SaadNo ratings yet
- 0080calibration MultipleDocument10 pages0080calibration MultiplePanneer SelvamNo ratings yet
- Basic Electricity. B TechDocument14 pagesBasic Electricity. B TechValentine Nwankwo100% (1)
- Electrical Machines and Control: REAL TransformersDocument25 pagesElectrical Machines and Control: REAL TransformersAmmar Syahid RabbaniNo ratings yet
- Tamara Bassam Abu Alwan: Visual Artist, PainterDocument2 pagesTamara Bassam Abu Alwan: Visual Artist, PainterTamara BellNo ratings yet
- SYDE 252 Linear Systems and Signals Fall 2005 Professor Ed Jernigan Systems Design Engineering University of WaterlooDocument70 pagesSYDE 252 Linear Systems and Signals Fall 2005 Professor Ed Jernigan Systems Design Engineering University of Waterloocartoon_nateNo ratings yet
- Traditional Tamil CropsDocument4 pagesTraditional Tamil CropsRahul KumarNo ratings yet
- Scheme Samsung NP r525 Bremen D Ba41 01197aDocument61 pagesScheme Samsung NP r525 Bremen D Ba41 01197aJerry BalbinNo ratings yet
- Program Mechanics Sy 2021-2022Document10 pagesProgram Mechanics Sy 2021-2022Deogracia BorresNo ratings yet
- Assignment For Week 1 - 2022Document5 pagesAssignment For Week 1 - 2022Rajveer deepNo ratings yet
- Screenshot 2020-12-24 at 11.13.39Document35 pagesScreenshot 2020-12-24 at 11.13.39Finca NurizzatiNo ratings yet
- 2n Quarter SCIENCE 8 - Quiz 2Document2 pages2n Quarter SCIENCE 8 - Quiz 2Jerwin Canteras100% (1)
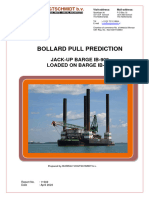
- Bollardpull Prediction IB-919 Loaded With IB-909Document14 pagesBollardpull Prediction IB-919 Loaded With IB-909jaap.w.jonkerNo ratings yet
- Sargonic and Gutian Periods PDFDocument182 pagesSargonic and Gutian Periods PDFRafael AzothNo ratings yet
- ECON198 Module 1Document4 pagesECON198 Module 1Kevin BelloNo ratings yet
- Music8 LAS Q3 Wk2Document2 pagesMusic8 LAS Q3 Wk2Marl Rina Esperanza100% (1)
- To Deleto4Document2 pagesTo Deleto4Paul Savvy100% (1)
- Econometrics QP CalicutDocument17 pagesEconometrics QP CalicutMadonaNo ratings yet
- Territorial and Extraterritorial Application of Criminal LawDocument8 pagesTerritorial and Extraterritorial Application of Criminal LawVirat SinghNo ratings yet
- Experiment 6 Kirchhoff and PowerDocument13 pagesExperiment 6 Kirchhoff and PowerVenus IlaganNo ratings yet
- Virtualization Without Direct Execution or Jitting: Designing A Portable Virtual Machine InfrastructureDocument16 pagesVirtualization Without Direct Execution or Jitting: Designing A Portable Virtual Machine InfrastructureihoneeNo ratings yet
- Subject ChemistryDocument13 pagesSubject ChemistryNikita JakharNo ratings yet
- Levels of AmputationDocument3 pagesLevels of AmputationPratyaksha TiwariNo ratings yet
- LP 1 Music Q3Document4 pagesLP 1 Music Q3Hazel Rubas SamsonNo ratings yet
- Science Q 3 3wk 5 - 3Document3 pagesScience Q 3 3wk 5 - 3Junior FelipzNo ratings yet
- Instagram GuideDocument21 pagesInstagram GuideMaria GelevaNo ratings yet
- DVB RodmDocument2 pagesDVB RodmAnanda BhattacharyyaNo ratings yet
- Grade 11 Provincial Examination Mathematics P1 (English) June 2022 Question PaperDocument7 pagesGrade 11 Provincial Examination Mathematics P1 (English) June 2022 Question PaperSiyamtanda DlangaNo ratings yet













































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Working Capital Simulation: Managing Growth V2Document5 pagesWorking Capital Simulation: Managing Growth V2Abdul Qader100% (6)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Risk Assessment For Installation of BMS M Tower PDFDocument15 pagesRisk Assessment For Installation of BMS M Tower PDFAndrew HivNo ratings yet
- 13 Japan Under The ShogunDocument22 pages13 Japan Under The Shogunapi-29949541290% (10)
- DOC571RevC AesculapNeedleComparisonChart 3 FoldBrochureDocument2 pagesDOC571RevC AesculapNeedleComparisonChart 3 FoldBrochureMuhammad SaadNo ratings yet
- Spleenomegaly & Hypersplenism Etiology Pathogenesis and Surgical ManagementDocument53 pagesSpleenomegaly & Hypersplenism Etiology Pathogenesis and Surgical ManagementMuhammad SaadNo ratings yet
- Residency Survival Guide: Canadian Association of General Surgeons Residents CommitteeDocument53 pagesResidency Survival Guide: Canadian Association of General Surgeons Residents CommitteeIrina MincuNo ratings yet
- IndexDocument2 pagesIndexMuhammad SaadNo ratings yet
- SurgeryDocument6 pagesSurgeryMuhammad Saad100% (1)
- Therapeutic EnzymesDocument39 pagesTherapeutic EnzymesMuhammad SaadNo ratings yet
- Pain Management-PRN OrdersDocument2 pagesPain Management-PRN OrdersMuhammad SaadNo ratings yet
- Guidelines For: Continuing Medical Education (CME) / Continuing Dental Education (eDE)Document12 pagesGuidelines For: Continuing Medical Education (CME) / Continuing Dental Education (eDE)Muhammad SaadNo ratings yet
- 0080calibration MultipleDocument10 pages0080calibration MultiplePanneer SelvamNo ratings yet
- Basic Electricity. B TechDocument14 pagesBasic Electricity. B TechValentine Nwankwo100% (1)
- Electrical Machines and Control: REAL TransformersDocument25 pagesElectrical Machines and Control: REAL TransformersAmmar Syahid RabbaniNo ratings yet
- Tamara Bassam Abu Alwan: Visual Artist, PainterDocument2 pagesTamara Bassam Abu Alwan: Visual Artist, PainterTamara BellNo ratings yet
- SYDE 252 Linear Systems and Signals Fall 2005 Professor Ed Jernigan Systems Design Engineering University of WaterlooDocument70 pagesSYDE 252 Linear Systems and Signals Fall 2005 Professor Ed Jernigan Systems Design Engineering University of Waterloocartoon_nateNo ratings yet
- Traditional Tamil CropsDocument4 pagesTraditional Tamil CropsRahul KumarNo ratings yet
- Scheme Samsung NP r525 Bremen D Ba41 01197aDocument61 pagesScheme Samsung NP r525 Bremen D Ba41 01197aJerry BalbinNo ratings yet
- Program Mechanics Sy 2021-2022Document10 pagesProgram Mechanics Sy 2021-2022Deogracia BorresNo ratings yet
- Assignment For Week 1 - 2022Document5 pagesAssignment For Week 1 - 2022Rajveer deepNo ratings yet
- Screenshot 2020-12-24 at 11.13.39Document35 pagesScreenshot 2020-12-24 at 11.13.39Finca NurizzatiNo ratings yet
- 2n Quarter SCIENCE 8 - Quiz 2Document2 pages2n Quarter SCIENCE 8 - Quiz 2Jerwin Canteras100% (1)
- Bollardpull Prediction IB-919 Loaded With IB-909Document14 pagesBollardpull Prediction IB-919 Loaded With IB-909jaap.w.jonkerNo ratings yet
- Sargonic and Gutian Periods PDFDocument182 pagesSargonic and Gutian Periods PDFRafael AzothNo ratings yet
- ECON198 Module 1Document4 pagesECON198 Module 1Kevin BelloNo ratings yet
- Music8 LAS Q3 Wk2Document2 pagesMusic8 LAS Q3 Wk2Marl Rina Esperanza100% (1)
- To Deleto4Document2 pagesTo Deleto4Paul Savvy100% (1)
- Econometrics QP CalicutDocument17 pagesEconometrics QP CalicutMadonaNo ratings yet
- Territorial and Extraterritorial Application of Criminal LawDocument8 pagesTerritorial and Extraterritorial Application of Criminal LawVirat SinghNo ratings yet
- Experiment 6 Kirchhoff and PowerDocument13 pagesExperiment 6 Kirchhoff and PowerVenus IlaganNo ratings yet
- Virtualization Without Direct Execution or Jitting: Designing A Portable Virtual Machine InfrastructureDocument16 pagesVirtualization Without Direct Execution or Jitting: Designing A Portable Virtual Machine InfrastructureihoneeNo ratings yet
- Subject ChemistryDocument13 pagesSubject ChemistryNikita JakharNo ratings yet
- Levels of AmputationDocument3 pagesLevels of AmputationPratyaksha TiwariNo ratings yet
- LP 1 Music Q3Document4 pagesLP 1 Music Q3Hazel Rubas SamsonNo ratings yet
- Science Q 3 3wk 5 - 3Document3 pagesScience Q 3 3wk 5 - 3Junior FelipzNo ratings yet
- Instagram GuideDocument21 pagesInstagram GuideMaria GelevaNo ratings yet
- DVB RodmDocument2 pagesDVB RodmAnanda BhattacharyyaNo ratings yet
- Grade 11 Provincial Examination Mathematics P1 (English) June 2022 Question PaperDocument7 pagesGrade 11 Provincial Examination Mathematics P1 (English) June 2022 Question PaperSiyamtanda DlangaNo ratings yet