
Oritavancin Orbactiv Monograph
Oritavancin Orbactiv Monograph
You might also like
- 10.beta Lactamase InhibitorsDocument15 pages10.beta Lactamase InhibitorsJagirNo ratings yet
- Orthopaedic Infection in Adults UHL GuidelineDocument10 pagesOrthopaedic Infection in Adults UHL GuidelineFadlu ManafNo ratings yet
- Folfiri+cetu Gi Col PDocument12 pagesFolfiri+cetu Gi Col PJayelle2No ratings yet
- Monkeypox and Pregnancy - What Maternal-Fetal Medicine Subspecialists Need To KnowDocument7 pagesMonkeypox and Pregnancy - What Maternal-Fetal Medicine Subspecialists Need To KnowariniNo ratings yet
- Post Partum Infections Obstet MedDocument5 pagesPost Partum Infections Obstet MedMutiaIlyasNo ratings yet
- Assessment of Antibiotic Utilization in Sepsis Order Sets Initiated in The Emergency Department Draft 2Document45 pagesAssessment of Antibiotic Utilization in Sepsis Order Sets Initiated in The Emergency Department Draft 2api-652562554No ratings yet
- V5 Revised Advisory On The Use of HCQ SARS CoV2 Infection PDFDocument4 pagesV5 Revised Advisory On The Use of HCQ SARS CoV2 Infection PDFMuhammad ZaibNo ratings yet
- Folfiri Beva Gi Col PDocument12 pagesFolfiri Beva Gi Col Pvera docNo ratings yet
- COVID-19 Protocol With TranslationDocument5 pagesCOVID-19 Protocol With TranslationStuart DitchekNo ratings yet
- EDT007Document110 pagesEDT007mahchusNo ratings yet
- Cefuroxime ZoltaxDocument2 pagesCefuroxime ZoltaxMJformorejokes minecraftNo ratings yet
- PHCh6 Obs& Gynaecology 2014Document56 pagesPHCh6 Obs& Gynaecology 2014Az-Zahraa NaasNo ratings yet
- Protocol 012Document17 pagesProtocol 012hatem newishyNo ratings yet
- Cowart2019 PDFDocument8 pagesCowart2019 PDFTHANHNo ratings yet
- VAP SlidesDocument25 pagesVAP SlidesGladys OliviaNo ratings yet
- Leaflet Artwork Design AVICOV Tablet Salut Selaput 200 MGDocument1 pageLeaflet Artwork Design AVICOV Tablet Salut Selaput 200 MGHenryNo ratings yet
- Surgical Antibiotic Prophylaxis - Orthopaedic Surgery in AdultsDocument7 pagesSurgical Antibiotic Prophylaxis - Orthopaedic Surgery in AdultsConstantin BudinNo ratings yet
- 13 Summary of Product Characteristics Labelling Package LeafletDocument20 pages13 Summary of Product Characteristics Labelling Package LeafletEnrique Carranza100% (1)
- Practice School - Bhavya PDFDocument25 pagesPractice School - Bhavya PDFBhavyaNo ratings yet
- Phenobarbitone SodiumDocument5 pagesPhenobarbitone SodiumArsia CallistioNo ratings yet
- LytalkristinDocument37 pagesLytalkristinapi-747604497No ratings yet
- Delafloxacin JCDocument11 pagesDelafloxacin JCDanny PhamNo ratings yet
- SHC SMUG RibavirinDocument2 pagesSHC SMUG RibavirinMario BulaciosNo ratings yet
- The Journal of Clinical Pharma - 2015 - Chen - Lack of Effect of Multiple Doses of Vortioxetine On The Pharmacokinetics andDocument9 pagesThe Journal of Clinical Pharma - 2015 - Chen - Lack of Effect of Multiple Doses of Vortioxetine On The Pharmacokinetics andRhima AnistyaNo ratings yet
- Antibiotic Stewardship Program PerspectiveDocument8 pagesAntibiotic Stewardship Program PerspectiveOsmanNo ratings yet
- SmpcserumDocument15 pagesSmpcserumGabriela MatuteNo ratings yet
- Whole Virion, Inactivated Corona Virus VaccineDocument42 pagesWhole Virion, Inactivated Corona Virus VaccineEnrique CarranzaNo ratings yet
- VarilrixDocument13 pagesVarilrixSoham SarangiNo ratings yet
- Intravenous To Oral ConversionDocument6 pagesIntravenous To Oral ConversiondoodrillNo ratings yet
- Day 1 PPS - de Los ReyesDocument51 pagesDay 1 PPS - de Los ReyesRye CalderonNo ratings yet
- Azithromycin Vs Erythromycin For The Management of Preterm Premature Rupture of MembranesDocument8 pagesAzithromycin Vs Erythromycin For The Management of Preterm Premature Rupture of Membranesizza istqmhNo ratings yet
- Peritonitis in Peritoneal Dialysis Patients 1.0 PDFDocument12 pagesPeritonitis in Peritoneal Dialysis Patients 1.0 PDFIndo MahardikaNo ratings yet
- เอกสารกำกับยา ภาษาอังกฤษ SinovacDocument12 pagesเอกสารกำกับยา ภาษาอังกฤษ SinovacAtawit SomsiriNo ratings yet
- I.5 - Ab Necrotizing FasciitisDocument16 pagesI.5 - Ab Necrotizing FasciitisShameen KhanNo ratings yet
- St. Vincent's Hospital Antibiotic Policy: GreenDocument2 pagesSt. Vincent's Hospital Antibiotic Policy: GreenistiqomahNo ratings yet
- V.3 21195 Sinopharm Vaccine Explainer 24Document6 pagesV.3 21195 Sinopharm Vaccine Explainer 24Mohammad Hisham BhawpalNo ratings yet
- Anticoagulant Protocol by Shymaa Shehata June 2022Document16 pagesAnticoagulant Protocol by Shymaa Shehata June 2022Esraa MoawadNo ratings yet
- Kanagalingam2015 PDFDocument10 pagesKanagalingam2015 PDFwatidinaNo ratings yet
- Therapeutic Monitoring of Vancomycin IDSADocument29 pagesTherapeutic Monitoring of Vancomycin IDSAArturo ArturoNo ratings yet
- Post Anaesthetic Care Unit (PACU) Opioid Administration For AdultsDocument7 pagesPost Anaesthetic Care Unit (PACU) Opioid Administration For Adultsbellahunter92No ratings yet
- Pharmacovigilance: FROMDocument46 pagesPharmacovigilance: FROMmeyhal17No ratings yet
- Highlights of Prescribing InformationDocument29 pagesHighlights of Prescribing Informationproject111995No ratings yet
- Antibiotic GuidelinesDocument54 pagesAntibiotic GuidelineskhattakpsychoNo ratings yet
- FLCCC Alliance Frequently Asked Questions On IvermectinDocument12 pagesFLCCC Alliance Frequently Asked Questions On IvermectinAndrés Mario Rivera RojasNo ratings yet
- Volume Probiotic Adjuvant Therapy Chronic Urticaria 4842allasp1Document8 pagesVolume Probiotic Adjuvant Therapy Chronic Urticaria 4842allasp1fatima amaliaNo ratings yet
- Tion - PDF: Page 1 of 3Document3 pagesTion - PDF: Page 1 of 3Jaidev sourotNo ratings yet
- 2014.04.17 PoltechDTPA SPCHDocument2 pages2014.04.17 PoltechDTPA SPCHLuis Fernando RicardoNo ratings yet
- Nejmoa 1310422Document11 pagesNejmoa 1310422mz zumrodinNo ratings yet
- Bookshelf NBK544685Document36 pagesBookshelf NBK544685ferdianriskaNo ratings yet
- Clin Infect Dis.-2010-Fishbain-79-84Document6 pagesClin Infect Dis.-2010-Fishbain-79-84Edson MarquesNo ratings yet
- Annex I Summary of Product CharacteristicsDocument33 pagesAnnex I Summary of Product CharacteristicsVimala BohoNo ratings yet
- Does Nephrotoxicity Develop Less Frequently When Vancomycin Is Combined With Imipenem-Cilastatin Than With Meropenem? A Comparative StudyDocument8 pagesDoes Nephrotoxicity Develop Less Frequently When Vancomycin Is Combined With Imipenem-Cilastatin Than With Meropenem? A Comparative StudyAsma BahriNo ratings yet
- Vero RabDocument8 pagesVero RabHandoyo KooNo ratings yet
- Classification: Cefditoren, As This Agent May CauseDocument3 pagesClassification: Cefditoren, As This Agent May CauseHavier EsparagueraNo ratings yet
- AEFI Surveillance and management-RVVDocument19 pagesAEFI Surveillance and management-RVVadi100% (1)
- Case Study FormatDocument4 pagesCase Study FormatKOBE TOMAGANNo ratings yet
- Invanz Epar Product Information enDocument32 pagesInvanz Epar Product Information enanaNo ratings yet
- 4 EpilepsiDocument7 pages4 EpilepsiNorman SukmadiNo ratings yet
- FosfomycinDocument4 pagesFosfomycinwantolla84No ratings yet
- Antivirals For Covid-19 and BreastfeedingDocument3 pagesAntivirals For Covid-19 and Breastfeedingkatherine juliaNo ratings yet
- Antibacterial Effect of Cassia Fistula Extract On Pathogenic Bacteria of Veterinary ImportanceDocument5 pagesAntibacterial Effect of Cassia Fistula Extract On Pathogenic Bacteria of Veterinary ImportanceAsif MajeedNo ratings yet
- PHARCHEM2 List AntimicrobialsDocument14 pagesPHARCHEM2 List AntimicrobialsLA BriguelaNo ratings yet
- 1 PDFDocument9 pages1 PDFFlorencia IrenaNo ratings yet
- Henson 2019Document5 pagesHenson 2019Edimar Joshua FrialaNo ratings yet
- 1a..antimicrobials IntroductionDocument84 pages1a..antimicrobials IntroductionAnonymous RlDDdTAsKJNo ratings yet
- Title Perioperative Antibiotic Prophylaxis in Orthognathic SurgeryDocument80 pagesTitle Perioperative Antibiotic Prophylaxis in Orthognathic SurgeryKuriyan ArimboorNo ratings yet
- Cephalosporins - 1st Generation To 5th GenerationDocument4 pagesCephalosporins - 1st Generation To 5th GenerationDr. Sadaf khanNo ratings yet
- Anatomy and Physiology Assignment 2Document5 pagesAnatomy and Physiology Assignment 2api-238869728No ratings yet
- Incidence and Role of Salmonella in Seafood SafetyDocument9 pagesIncidence and Role of Salmonella in Seafood SafetygiuseppegnrNo ratings yet
- LuyaDocument105 pagesLuyaKaye FCNo ratings yet
- Journal - Bacteria Virtual LabDocument1 pageJournal - Bacteria Virtual Labapi-348935712No ratings yet
- Adhatoda VasicaDocument10 pagesAdhatoda VasicaMohan PalanisamiNo ratings yet
- Pharmacist's Letter: Prescriber's LetterDocument6 pagesPharmacist's Letter: Prescriber's LetterJaved AkhtarNo ratings yet
- Topical Issues in Anesthesia 2016Document207 pagesTopical Issues in Anesthesia 2016Ketzalzin DmgNo ratings yet
- 1 s2.0 S0304416513000512 MainDocument26 pages1 s2.0 S0304416513000512 MainRiza MurniatiNo ratings yet
- HNA BARU RevisiDocument23 pagesHNA BARU RevisinooNo ratings yet
- Food SafetyDocument329 pagesFood Safetykave4923100% (15)
- Chap 1 2.0Document6 pagesChap 1 2.0Landhel Galinato LoboNo ratings yet
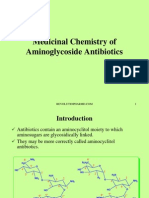
- Medicinal Chemistry of Aminoglycoside AntibioticsDocument31 pagesMedicinal Chemistry of Aminoglycoside AntibioticsKevin Chapley100% (3)
- h1n1 Master TonicDocument2 pagesh1n1 Master TonicmmetaNo ratings yet
- Pharmd - 3Y - 3.5 - Medicinal ChemistryDocument41 pagesPharmd - 3Y - 3.5 - Medicinal ChemistrySyed Ali ShahNo ratings yet
- BARU 3 Ptsa 150923Document117 pagesBARU 3 Ptsa 150923Joyoboyo PrimaNo ratings yet
- Ventilator Associated Pneumonia TreatmentDocument43 pagesVentilator Associated Pneumonia Treatmentmkc71No ratings yet
- Antibiotics Guide 2013Document30 pagesAntibiotics Guide 2013Stefani NoviliaNo ratings yet
- Study of Antibiotic-Resistance and Sensitivity Pattern in A Tertiary Care Teaching HospitalDocument8 pagesStudy of Antibiotic-Resistance and Sensitivity Pattern in A Tertiary Care Teaching HospitalIJAR JOURNALNo ratings yet
- ANTIBIOTICE RetetaDocument4 pagesANTIBIOTICE RetetairrrsNo ratings yet
- 7 MRSA and Controling-12Document12 pages7 MRSA and Controling-12RavinderenPichanNo ratings yet
- DRUG STUDY: Rocephin - Ceftriaxone SodiumDocument1 pageDRUG STUDY: Rocephin - Ceftriaxone SodiumYum C100% (1)
- Cefepime MaxipimeDocument2 pagesCefepime MaxipimeKristi Wray100% (1)
























































































Download as pdf or txt
You might also like
- 10.beta Lactamase InhibitorsDocument15 pages10.beta Lactamase InhibitorsJagirNo ratings yet
- Orthopaedic Infection in Adults UHL GuidelineDocument10 pagesOrthopaedic Infection in Adults UHL GuidelineFadlu ManafNo ratings yet
- Folfiri+cetu Gi Col PDocument12 pagesFolfiri+cetu Gi Col PJayelle2No ratings yet
- Monkeypox and Pregnancy - What Maternal-Fetal Medicine Subspecialists Need To KnowDocument7 pagesMonkeypox and Pregnancy - What Maternal-Fetal Medicine Subspecialists Need To KnowariniNo ratings yet
- Post Partum Infections Obstet MedDocument5 pagesPost Partum Infections Obstet MedMutiaIlyasNo ratings yet
- Assessment of Antibiotic Utilization in Sepsis Order Sets Initiated in The Emergency Department Draft 2Document45 pagesAssessment of Antibiotic Utilization in Sepsis Order Sets Initiated in The Emergency Department Draft 2api-652562554No ratings yet
- V5 Revised Advisory On The Use of HCQ SARS CoV2 Infection PDFDocument4 pagesV5 Revised Advisory On The Use of HCQ SARS CoV2 Infection PDFMuhammad ZaibNo ratings yet
- Folfiri Beva Gi Col PDocument12 pagesFolfiri Beva Gi Col Pvera docNo ratings yet
- COVID-19 Protocol With TranslationDocument5 pagesCOVID-19 Protocol With TranslationStuart DitchekNo ratings yet
- EDT007Document110 pagesEDT007mahchusNo ratings yet
- Cefuroxime ZoltaxDocument2 pagesCefuroxime ZoltaxMJformorejokes minecraftNo ratings yet
- PHCh6 Obs& Gynaecology 2014Document56 pagesPHCh6 Obs& Gynaecology 2014Az-Zahraa NaasNo ratings yet
- Protocol 012Document17 pagesProtocol 012hatem newishyNo ratings yet
- Cowart2019 PDFDocument8 pagesCowart2019 PDFTHANHNo ratings yet
- VAP SlidesDocument25 pagesVAP SlidesGladys OliviaNo ratings yet
- Leaflet Artwork Design AVICOV Tablet Salut Selaput 200 MGDocument1 pageLeaflet Artwork Design AVICOV Tablet Salut Selaput 200 MGHenryNo ratings yet
- Surgical Antibiotic Prophylaxis - Orthopaedic Surgery in AdultsDocument7 pagesSurgical Antibiotic Prophylaxis - Orthopaedic Surgery in AdultsConstantin BudinNo ratings yet
- 13 Summary of Product Characteristics Labelling Package LeafletDocument20 pages13 Summary of Product Characteristics Labelling Package LeafletEnrique Carranza100% (1)
- Practice School - Bhavya PDFDocument25 pagesPractice School - Bhavya PDFBhavyaNo ratings yet
- Phenobarbitone SodiumDocument5 pagesPhenobarbitone SodiumArsia CallistioNo ratings yet
- LytalkristinDocument37 pagesLytalkristinapi-747604497No ratings yet
- Delafloxacin JCDocument11 pagesDelafloxacin JCDanny PhamNo ratings yet
- SHC SMUG RibavirinDocument2 pagesSHC SMUG RibavirinMario BulaciosNo ratings yet
- The Journal of Clinical Pharma - 2015 - Chen - Lack of Effect of Multiple Doses of Vortioxetine On The Pharmacokinetics andDocument9 pagesThe Journal of Clinical Pharma - 2015 - Chen - Lack of Effect of Multiple Doses of Vortioxetine On The Pharmacokinetics andRhima AnistyaNo ratings yet
- Antibiotic Stewardship Program PerspectiveDocument8 pagesAntibiotic Stewardship Program PerspectiveOsmanNo ratings yet
- SmpcserumDocument15 pagesSmpcserumGabriela MatuteNo ratings yet
- Whole Virion, Inactivated Corona Virus VaccineDocument42 pagesWhole Virion, Inactivated Corona Virus VaccineEnrique CarranzaNo ratings yet
- VarilrixDocument13 pagesVarilrixSoham SarangiNo ratings yet
- Intravenous To Oral ConversionDocument6 pagesIntravenous To Oral ConversiondoodrillNo ratings yet
- Day 1 PPS - de Los ReyesDocument51 pagesDay 1 PPS - de Los ReyesRye CalderonNo ratings yet
- Azithromycin Vs Erythromycin For The Management of Preterm Premature Rupture of MembranesDocument8 pagesAzithromycin Vs Erythromycin For The Management of Preterm Premature Rupture of Membranesizza istqmhNo ratings yet
- Peritonitis in Peritoneal Dialysis Patients 1.0 PDFDocument12 pagesPeritonitis in Peritoneal Dialysis Patients 1.0 PDFIndo MahardikaNo ratings yet
- เอกสารกำกับยา ภาษาอังกฤษ SinovacDocument12 pagesเอกสารกำกับยา ภาษาอังกฤษ SinovacAtawit SomsiriNo ratings yet
- I.5 - Ab Necrotizing FasciitisDocument16 pagesI.5 - Ab Necrotizing FasciitisShameen KhanNo ratings yet
- St. Vincent's Hospital Antibiotic Policy: GreenDocument2 pagesSt. Vincent's Hospital Antibiotic Policy: GreenistiqomahNo ratings yet
- V.3 21195 Sinopharm Vaccine Explainer 24Document6 pagesV.3 21195 Sinopharm Vaccine Explainer 24Mohammad Hisham BhawpalNo ratings yet
- Anticoagulant Protocol by Shymaa Shehata June 2022Document16 pagesAnticoagulant Protocol by Shymaa Shehata June 2022Esraa MoawadNo ratings yet
- Kanagalingam2015 PDFDocument10 pagesKanagalingam2015 PDFwatidinaNo ratings yet
- Therapeutic Monitoring of Vancomycin IDSADocument29 pagesTherapeutic Monitoring of Vancomycin IDSAArturo ArturoNo ratings yet
- Post Anaesthetic Care Unit (PACU) Opioid Administration For AdultsDocument7 pagesPost Anaesthetic Care Unit (PACU) Opioid Administration For Adultsbellahunter92No ratings yet
- Pharmacovigilance: FROMDocument46 pagesPharmacovigilance: FROMmeyhal17No ratings yet
- Highlights of Prescribing InformationDocument29 pagesHighlights of Prescribing Informationproject111995No ratings yet
- Antibiotic GuidelinesDocument54 pagesAntibiotic GuidelineskhattakpsychoNo ratings yet
- FLCCC Alliance Frequently Asked Questions On IvermectinDocument12 pagesFLCCC Alliance Frequently Asked Questions On IvermectinAndrés Mario Rivera RojasNo ratings yet
- Volume Probiotic Adjuvant Therapy Chronic Urticaria 4842allasp1Document8 pagesVolume Probiotic Adjuvant Therapy Chronic Urticaria 4842allasp1fatima amaliaNo ratings yet
- Tion - PDF: Page 1 of 3Document3 pagesTion - PDF: Page 1 of 3Jaidev sourotNo ratings yet
- 2014.04.17 PoltechDTPA SPCHDocument2 pages2014.04.17 PoltechDTPA SPCHLuis Fernando RicardoNo ratings yet
- Nejmoa 1310422Document11 pagesNejmoa 1310422mz zumrodinNo ratings yet
- Bookshelf NBK544685Document36 pagesBookshelf NBK544685ferdianriskaNo ratings yet
- Clin Infect Dis.-2010-Fishbain-79-84Document6 pagesClin Infect Dis.-2010-Fishbain-79-84Edson MarquesNo ratings yet
- Annex I Summary of Product CharacteristicsDocument33 pagesAnnex I Summary of Product CharacteristicsVimala BohoNo ratings yet
- Does Nephrotoxicity Develop Less Frequently When Vancomycin Is Combined With Imipenem-Cilastatin Than With Meropenem? A Comparative StudyDocument8 pagesDoes Nephrotoxicity Develop Less Frequently When Vancomycin Is Combined With Imipenem-Cilastatin Than With Meropenem? A Comparative StudyAsma BahriNo ratings yet
- Vero RabDocument8 pagesVero RabHandoyo KooNo ratings yet
- Classification: Cefditoren, As This Agent May CauseDocument3 pagesClassification: Cefditoren, As This Agent May CauseHavier EsparagueraNo ratings yet
- AEFI Surveillance and management-RVVDocument19 pagesAEFI Surveillance and management-RVVadi100% (1)
- Case Study FormatDocument4 pagesCase Study FormatKOBE TOMAGANNo ratings yet
- Invanz Epar Product Information enDocument32 pagesInvanz Epar Product Information enanaNo ratings yet
- 4 EpilepsiDocument7 pages4 EpilepsiNorman SukmadiNo ratings yet
- FosfomycinDocument4 pagesFosfomycinwantolla84No ratings yet
- Antivirals For Covid-19 and BreastfeedingDocument3 pagesAntivirals For Covid-19 and Breastfeedingkatherine juliaNo ratings yet
- Antibacterial Effect of Cassia Fistula Extract On Pathogenic Bacteria of Veterinary ImportanceDocument5 pagesAntibacterial Effect of Cassia Fistula Extract On Pathogenic Bacteria of Veterinary ImportanceAsif MajeedNo ratings yet
- PHARCHEM2 List AntimicrobialsDocument14 pagesPHARCHEM2 List AntimicrobialsLA BriguelaNo ratings yet
- 1 PDFDocument9 pages1 PDFFlorencia IrenaNo ratings yet
- Henson 2019Document5 pagesHenson 2019Edimar Joshua FrialaNo ratings yet
- 1a..antimicrobials IntroductionDocument84 pages1a..antimicrobials IntroductionAnonymous RlDDdTAsKJNo ratings yet
- Title Perioperative Antibiotic Prophylaxis in Orthognathic SurgeryDocument80 pagesTitle Perioperative Antibiotic Prophylaxis in Orthognathic SurgeryKuriyan ArimboorNo ratings yet
- Cephalosporins - 1st Generation To 5th GenerationDocument4 pagesCephalosporins - 1st Generation To 5th GenerationDr. Sadaf khanNo ratings yet
- Anatomy and Physiology Assignment 2Document5 pagesAnatomy and Physiology Assignment 2api-238869728No ratings yet
- Incidence and Role of Salmonella in Seafood SafetyDocument9 pagesIncidence and Role of Salmonella in Seafood SafetygiuseppegnrNo ratings yet
- LuyaDocument105 pagesLuyaKaye FCNo ratings yet
- Journal - Bacteria Virtual LabDocument1 pageJournal - Bacteria Virtual Labapi-348935712No ratings yet
- Adhatoda VasicaDocument10 pagesAdhatoda VasicaMohan PalanisamiNo ratings yet
- Pharmacist's Letter: Prescriber's LetterDocument6 pagesPharmacist's Letter: Prescriber's LetterJaved AkhtarNo ratings yet
- Topical Issues in Anesthesia 2016Document207 pagesTopical Issues in Anesthesia 2016Ketzalzin DmgNo ratings yet
- 1 s2.0 S0304416513000512 MainDocument26 pages1 s2.0 S0304416513000512 MainRiza MurniatiNo ratings yet
- HNA BARU RevisiDocument23 pagesHNA BARU RevisinooNo ratings yet
- Food SafetyDocument329 pagesFood Safetykave4923100% (15)
- Chap 1 2.0Document6 pagesChap 1 2.0Landhel Galinato LoboNo ratings yet
- Medicinal Chemistry of Aminoglycoside AntibioticsDocument31 pagesMedicinal Chemistry of Aminoglycoside AntibioticsKevin Chapley100% (3)
- h1n1 Master TonicDocument2 pagesh1n1 Master TonicmmetaNo ratings yet
- Pharmd - 3Y - 3.5 - Medicinal ChemistryDocument41 pagesPharmd - 3Y - 3.5 - Medicinal ChemistrySyed Ali ShahNo ratings yet
- BARU 3 Ptsa 150923Document117 pagesBARU 3 Ptsa 150923Joyoboyo PrimaNo ratings yet
- Ventilator Associated Pneumonia TreatmentDocument43 pagesVentilator Associated Pneumonia Treatmentmkc71No ratings yet
- Antibiotics Guide 2013Document30 pagesAntibiotics Guide 2013Stefani NoviliaNo ratings yet
- Study of Antibiotic-Resistance and Sensitivity Pattern in A Tertiary Care Teaching HospitalDocument8 pagesStudy of Antibiotic-Resistance and Sensitivity Pattern in A Tertiary Care Teaching HospitalIJAR JOURNALNo ratings yet
- ANTIBIOTICE RetetaDocument4 pagesANTIBIOTICE RetetairrrsNo ratings yet
- 7 MRSA and Controling-12Document12 pages7 MRSA and Controling-12RavinderenPichanNo ratings yet
- DRUG STUDY: Rocephin - Ceftriaxone SodiumDocument1 pageDRUG STUDY: Rocephin - Ceftriaxone SodiumYum C100% (1)
- Cefepime MaxipimeDocument2 pagesCefepime MaxipimeKristi Wray100% (1)