Download as pdf or txt
You might also like
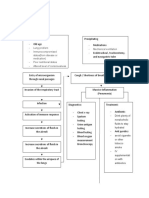
- PneumoniaDocument1 pagePneumonianursing concept mapsNo ratings yet
- Adapting Organization To Environment UncertaintyDocument19 pagesAdapting Organization To Environment UncertaintySameer MiraniNo ratings yet
- Kone Case AnalysisDocument6 pagesKone Case AnalysisNikit Tyagi50% (2)
- Module 5: Practice Problems: Answer: 3 Grams (G)Document11 pagesModule 5: Practice Problems: Answer: 3 Grams (G)Katrina Tiempo Miquiabas0% (1)
- ISO 45001 2018 UpdatedDocument44 pagesISO 45001 2018 UpdatedSagar Shah100% (4)
- Dhamrai Craft Village, Thesis ArchitectureDocument142 pagesDhamrai Craft Village, Thesis ArchitectureMahbuba Moumi100% (7)
- Management of Pneumonia Focus On Empirical AntimicrobialDocument34 pagesManagement of Pneumonia Focus On Empirical AntimicrobialAgus FujiNo ratings yet
- Tatalaksana PneumoniaDocument37 pagesTatalaksana PneumoniaAnonymous R6ex8BM0No ratings yet
- DR Maurits - PNEUMONIA DIES NATALIS KG88 PDFDocument37 pagesDR Maurits - PNEUMONIA DIES NATALIS KG88 PDFdanang andi100% (1)
- Bacterial PneumoniaDocument4 pagesBacterial PneumoniaPabinaNo ratings yet
- Dr. Constatntino: PneumomiaDocument4 pagesDr. Constatntino: PneumomiaAnn Ross VidalNo ratings yet
- Bronchitis: Dr. Bobi Ahmad S, S.KepDocument41 pagesBronchitis: Dr. Bobi Ahmad S, S.Kepdr.Bobi Ahmad Sahid, S.KepNo ratings yet
- Rahma Dan CAPDocument17 pagesRahma Dan CAPpeterNo ratings yet
- Med Surg 1 NotesDocument11 pagesMed Surg 1 NotesMark Jefferson LunaNo ratings yet
- Final Pneumonia AlgorithmDocument1 pageFinal Pneumonia AlgorithmWajih FarhanNo ratings yet
- Pathophysiology PneumoniaDocument2 pagesPathophysiology PneumoniaChiro Rouy Malaluan100% (2)
- Ceftizadime. EDHDocument2 pagesCeftizadime. EDH1adie1907No ratings yet
- Drug StudyDocument22 pagesDrug StudySierraSiwaNo ratings yet
- Drug StudyDocument22 pagesDrug StudySierraSiwaNo ratings yet
- Drug Study 4Document5 pagesDrug Study 4Saito SanNo ratings yet
- DIPTHERIADocument2 pagesDIPTHERIADr KhatidjaNo ratings yet
- Pneumonia Cheat Sheet: by ViaDocument3 pagesPneumonia Cheat Sheet: by ViaGayle MarieNo ratings yet
- Lower Rspiratory Tract - Pneumonia-: BalanceDocument7 pagesLower Rspiratory Tract - Pneumonia-: BalanceSofronio OmboyNo ratings yet
- Adult PathophysiologyDocument163 pagesAdult PathophysiologyRuthaliya IbrahimNo ratings yet
- Exam 2 Study Guide 2018Document21 pagesExam 2 Study Guide 2018EvanNo ratings yet
- Infeksi 1 GabunganDocument78 pagesInfeksi 1 Gabungan404notfoundNo ratings yet
- Drug TabulationDocument6 pagesDrug TabulationKANT JAMES D. MAHANNo ratings yet
- 6 CapDocument24 pages6 CapAyush GodhaniNo ratings yet
- Pneumonia (Fix)Document64 pagesPneumonia (Fix)Kornelis AribowoNo ratings yet
- Antimicrobials IT12021Document56 pagesAntimicrobials IT12021angelamnsrNo ratings yet
- Pneumonia: Anas Bahnassi PHDDocument26 pagesPneumonia: Anas Bahnassi PHDyasmine abdelkarimNo ratings yet
- 118 ReviewerDocument6 pages118 ReviewerAna Rose Dela CruzNo ratings yet
- 7.chest and Lower Respiratory Tract DisordersDocument8 pages7.chest and Lower Respiratory Tract Disorders2BGrp3Plaza, Anna MaeNo ratings yet
- USM Abx PDFDocument4 pagesUSM Abx PDFEidi IdhamNo ratings yet
- Comparative - URT and PneumoniaDocument4 pagesComparative - URT and Pneumoniange257No ratings yet
- Dipiro PneumoniaDocument8 pagesDipiro Pneumoniameri dayaniNo ratings yet
- Diphteria, Pertussis and Staphylococcal Infections-1Document15 pagesDiphteria, Pertussis and Staphylococcal Infections-1Nwosu Ogbonna GabrielNo ratings yet
- Screenshot 2023-03-20 at 10.30.42 PMDocument66 pagesScreenshot 2023-03-20 at 10.30.42 PMFATEN ATHIRAH BINTI ABDUL RAZAKNo ratings yet
- Favipiravir 071120Document55 pagesFavipiravir 071120w5bwmbfrtwNo ratings yet
- 1.1 Overview & OutcomesDocument5 pages1.1 Overview & OutcomesShayla HudsonNo ratings yet
- Pneumonia in Children: Monocytogenes, Chlamydia TrachomatisDocument1 pagePneumonia in Children: Monocytogenes, Chlamydia TrachomatisAlcala, Mariaden A.100% (1)
- 7fa8e6ac-47db-4f0f-90f3-bb6e1ece863cDocument18 pages7fa8e6ac-47db-4f0f-90f3-bb6e1ece863cSatendra SrivastavaNo ratings yet
- Penggolongan Obat Berdasar Kelas TerapiDocument6 pagesPenggolongan Obat Berdasar Kelas TerapiSyaira MuhlisaNo ratings yet
- IMG EmpAposterDocument1 pageIMG EmpAposterChiu LeoNo ratings yet
- Pneumonia Kuliah 2024Document40 pagesPneumonia Kuliah 2024flowerpearlyNo ratings yet
- Week 1 TropMedDocument96 pagesWeek 1 TropMedmyqurandiaryNo ratings yet
- Drug StudyDocument1 pageDrug Studynuguitnorelyn30No ratings yet
- Pneumonia: or Generalized Patchy InfiltrateDocument3 pagesPneumonia: or Generalized Patchy InfiltrateizyanzatiNo ratings yet
- Case Analysis PediatricsDocument31 pagesCase Analysis PediatricsLYNDLY AGAGEONo ratings yet
- Respiratory 1Document28 pagesRespiratory 1Howell MathewNo ratings yet
- Kuliah Respirologi Anak: Divisi Respirologi Departemen Ilmu Kesehatan Anak FK Undip / Rsup DR Kariadi SemarangDocument114 pagesKuliah Respirologi Anak: Divisi Respirologi Departemen Ilmu Kesehatan Anak FK Undip / Rsup DR Kariadi SemarangLailatuz ZakiyahNo ratings yet
- Antibiotics in Critically IllnessDocument106 pagesAntibiotics in Critically IllnessFransisca Dewi KumalaNo ratings yet
- 1 Ceftizidime - EDHDocument3 pages1 Ceftizidime - EDH1adie1907No ratings yet
- LungsDocument34 pagesLungsErshelle Mae MorlaNo ratings yet
- Pneumonia (Dr. Tjahyo, Sp.A)Document22 pagesPneumonia (Dr. Tjahyo, Sp.A)Yoseph MarianoNo ratings yet
- Pneumonia - Knowledge at AMBOSSDocument3 pagesPneumonia - Knowledge at AMBOSSKC Dela RosaNo ratings yet
- InfectionDocument96 pagesInfectionBassem Georguos LabibNo ratings yet
- Pneumonia Presentatition1Document8 pagesPneumonia Presentatition1Titian DiasNo ratings yet
- NCM112 LP2 TransesDocument9 pagesNCM112 LP2 TransesChristine CalleyNo ratings yet
- Pneumonia: Romero, Pamela Sanchez, DianeDocument13 pagesPneumonia: Romero, Pamela Sanchez, DianePam RomeroNo ratings yet
- 4 Drug Studies AppendectomyDocument9 pages4 Drug Studies AppendectomyCharish Ann VillanuevaNo ratings yet
- HT Emergencies FinalDocument1 pageHT Emergencies Finalsubha95No ratings yet
- The Management of MycosisDocument43 pagesThe Management of Mycosissyarah mutiaNo ratings yet
- Transes 2 (PCOL)Document11 pagesTranses 2 (PCOL)Ashley Judd EmpaynadoNo ratings yet
- The Flu: A Guide for Prevention and TreatmentFrom EverandThe Flu: A Guide for Prevention and TreatmentRating: 5 out of 5 stars5/5 (1)
- Turning Soils Into Sponges: How Farmers Can Fight Floods and DroughtsDocument20 pagesTurning Soils Into Sponges: How Farmers Can Fight Floods and DroughtsHusam Moh'd MurshidNo ratings yet
- X X X X X X X X X X X X X X: Sec Tan Sin Tan Sin CSC Cot Cos CSC Cot Cot Cos Tan SecDocument7 pagesX X X X X X X X X X X X X X: Sec Tan Sin Tan Sin CSC Cot Cos CSC Cot Cot Cos Tan SecKevin Christian Plata100% (1)
- Myro Sebastien M. Mera 202011465 1 Year BSCE NSTP 2 - Tv13: Source: GMA Network, 2017Document52 pagesMyro Sebastien M. Mera 202011465 1 Year BSCE NSTP 2 - Tv13: Source: GMA Network, 2017Jered MiluhonNo ratings yet
- Lethe Bear Varimixer RN10 VL2 MANDocument21 pagesLethe Bear Varimixer RN10 VL2 MANGolden OdyesseyNo ratings yet
- Mobile Phone: Service ManualDocument128 pagesMobile Phone: Service ManualsamuelNo ratings yet
- Computation Theory: Lecture TwoDocument9 pagesComputation Theory: Lecture TwoColmain NassiriNo ratings yet
- MFC J410WDocument32 pagesMFC J410Wcoffee451No ratings yet
- Fundamentals of Digital IC Design: ECE 428 Programmable ASIC DesignDocument29 pagesFundamentals of Digital IC Design: ECE 428 Programmable ASIC DesignBadangNo ratings yet
- Eco 270Document9 pagesEco 270Tarun Shankar ChoudharyNo ratings yet
- Power Engineering PM Check ListDocument11 pagesPower Engineering PM Check ListSelvn SubramanianNo ratings yet
- Chemistry-Ch 3 - Chemical BondingDocument8 pagesChemistry-Ch 3 - Chemical BondingHassan RiazNo ratings yet
- Introduction To Nearshore HydrodynamicsDocument10 pagesIntroduction To Nearshore Hydrodynamicsjuand_121No ratings yet
- The Haryana Value Added Tax ACT, 2003Document83 pagesThe Haryana Value Added Tax ACT, 2003adwiteya groverNo ratings yet
- Parametric Kerf Bending - ArticleDocument25 pagesParametric Kerf Bending - ArticleMIS-TRYNo ratings yet
- Free IDS V86 Software Download Link For FORD - MAZDA IDS V86Document2 pagesFree IDS V86 Software Download Link For FORD - MAZDA IDS V86Yousef ShishaniNo ratings yet
- Booklist Grade 3Document3 pagesBooklist Grade 3solid_impactNo ratings yet
- Thank You For The Broken HeartDocument76 pagesThank You For The Broken Heartkaito_shinigamiNo ratings yet
- Welcome To Presentation On Discharge of SuretyDocument18 pagesWelcome To Presentation On Discharge of SuretyAmit Gurav94% (16)
- Exercise 5: Chapter 6, Section 6.1, Page 396Document2 pagesExercise 5: Chapter 6, Section 6.1, Page 396allauddinbaloch84No ratings yet
- IAS 36 Impairment of Assets (2021)Document12 pagesIAS 36 Impairment of Assets (2021)Tawanda Tatenda HerbertNo ratings yet
- 05j - 21BB Model Region Berlin-Brandenburg PDFDocument9 pages05j - 21BB Model Region Berlin-Brandenburg PDFdean j almy IIINo ratings yet
- To Cleaning & Degreasing Within The Industrial ManufacturingDocument8 pagesTo Cleaning & Degreasing Within The Industrial ManufacturingukalNo ratings yet
- Sirius Timer Relay ManualDocument28 pagesSirius Timer Relay ManualVinoth MahendranNo ratings yet
- Cayle y ResultsDocument40 pagesCayle y ResultsAyan NadeemNo ratings yet
- Zodia Taur EnglezaDocument3 pagesZodia Taur EnglezaoantaNo ratings yet