
Brochure and Legal Analysis
Brochure and Legal Analysis
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- MonFore EvictedDocument14 pagesMonFore EvictedPat PowersNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Rounds for Senate 2024 2q FECDocument78 pagesRounds for Senate 2024 2q FECPat PowersNo ratings yet
- 2q FEC Sheryl Johnson for CongressDocument48 pages2q FEC Sheryl Johnson for CongressPat PowersNo ratings yet
- South Dakota Carbon Capture MemoDocument2 pagesSouth Dakota Carbon Capture MemoPat PowersNo ratings yet
- Sutton Disclosure 2020 Pre-PrimaryDocument6 pagesSutton Disclosure 2020 Pre-PrimaryPat Powers100% (1)
- Tony Kay Ser Pre-Primary ReportDocument9 pagesTony Kay Ser Pre-Primary ReportPat PowersNo ratings yet
- Dakota First Action - Toby Doeden AffidavitDocument11 pagesDakota First Action - Toby Doeden AffidavitPat PowersNo ratings yet
- FRC GOPPlatformSurveyDocument16 pagesFRC GOPPlatformSurveyPat PowersNo ratings yet
- 23civ24-000005 - Order To Show CauseDocument2 pages23civ24-000005 - Order To Show CausePat PowersNo ratings yet
- Sanders FEC FilingsDocument5 pagesSanders FEC FilingsPat PowersNo ratings yet
- Sutton Disclosure 2020 Pre-PrimaryDocument6 pagesSutton Disclosure 2020 Pre-PrimaryPat Powers100% (1)
- Heidi Heitkamp 2019 Year-End FEC ReportDocument55 pagesHeidi Heitkamp 2019 Year-End FEC ReportRob PortNo ratings yet
- ShadOlson SCAN0001 RedactedDocument4 pagesShadOlson SCAN0001 RedactedPat PowersNo ratings yet
- FRC DRAFT Meeting Minutes 3-14-2023Document3 pagesFRC DRAFT Meeting Minutes 3-14-2023Pat PowersNo ratings yet
- 66civ23-000155 Memorandum DecisionDocument5 pages66civ23-000155 Memorandum DecisionPat PowersNo ratings yet
- Kent Roe SdcfdisclosureDocument2 pagesKent Roe SdcfdisclosurePat PowersNo ratings yet
- FEC Termination Filing For Annette Bosworth MDDocument6 pagesFEC Termination Filing For Annette Bosworth MDPat PowersNo ratings yet
- Sutton Disclosure 2020 Pre-PrimaryDocument6 pagesSutton Disclosure 2020 Pre-PrimaryPat Powers100% (1)
- NoemopinionSCTbrf Filed 12-15-23Document59 pagesNoemopinionSCTbrf Filed 12-15-23Pat PowersNo ratings yet
- Heidi Heitkamp 2019 Year-End FEC ReportDocument55 pagesHeidi Heitkamp 2019 Year-End FEC ReportRob PortNo ratings yet
- Taffy Howard 2024 Campaign Finance DisclosureDocument2 pagesTaffy Howard 2024 Campaign Finance DisclosurePat PowersNo ratings yet
- Sutton Disclosure 2020 Pre-PrimaryDocument6 pagesSutton Disclosure 2020 Pre-PrimaryPat Powers100% (1)
- Castleberry Settlement AgreementDocument4 pagesCastleberry Settlement AgreementPat PowersNo ratings yet
- Ltr. MJJ To Johnson Const Amend Prohibit Legis Repeal or Change Initiated Measure. Darft 6.28.2023Document3 pagesLtr. MJJ To Johnson Const Amend Prohibit Legis Repeal or Change Initiated Measure. Darft 6.28.2023Pat PowersNo ratings yet
- YanktonGOP1 1Document5 pagesYanktonGOP1 1Pat PowersNo ratings yet
- Dusty Johnson October 2024 FECDocument161 pagesDusty Johnson October 2024 FECPat PowersNo ratings yet
- Schoenbeck Law Review Article On ImpeachmentDocument20 pagesSchoenbeck Law Review Article On ImpeachmentPat PowersNo ratings yet
- Zach Kovach FECDocument10 pagesZach Kovach FECPat PowersNo ratings yet
- AustinGossArrest ImpersonatingGovNoemDocument5 pagesAustinGossArrest ImpersonatingGovNoemPat PowersNo ratings yet
- SD Freedom Caucus 061223Document6 pagesSD Freedom Caucus 061223Pat PowersNo ratings yet


































































Download as pdf
Uae SITS RULE ae
RUE aa eee
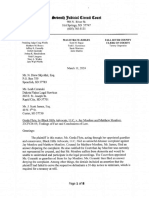
Assisted Suicide — currently legal in only five states and the District of Columbia
South Dakota has one of the highest suicide rates in the nation,
including the 2015 outbreak of suicides on the Pine Ridge Indian Reservation '?'°
LETHAL ADDICTIVE DRUGS GO UNUSED
10 patient fils he lethal prescription — typically a,
100 pills — but decides agoinst taking it, there are @
1 safeguards to ensure the drugs stay out of the a.
hands of children and pres drug dealers.
The measure provides for patients fo obtain lethal
drugs and then simply store them in their home.
In Otegon, 554 people filed their prescriptions
‘and decided not to end their lives, leaving tens
of thousands of highly addictive barpiturates
unaccounted far?
de. The
MENTAL HEALTH CONDITIONS
ARE IGNORED
Teen Aer saa E ed
‘with the. most data, oniy 4% of patients who
Ce eee
Cee
Peet
eR esc)
measure, doctors are oy
teeter
formenial health
eterna)
Peers
Cee esac ere ial
ee ee cea
eee Ie eis
WHOSE CHOICE |S IT?
OPENS DOOR TO ABUSE OF ELDERLY OR INFIRM
TORU ay aero Rue reer ae -olgl
Petes Segue ene outed ae ena
eel ea ne ofeach ea ony
Nea ee sete meted takes SN
eae etary
Same ecg
eee Mule ge ey
Peteel eo tease ed
iti hee lias \
Cee Maer ncaa
Cer ge checa cle gh tear}
(Section 3). Once lethal prescription is
written, an abusive caregiver of relative
Ren hares oa iq
can pick it up and give it to the patient in
erg ener)
een cn eps atn
Sea Eee et ot)
Cie cai aaa!
peeked
| South | Citizens Aga
Dakota Assisted Suic
Serious Side Effects
of Assisted Suicide Laws
NO MENTAL HEALTH NO WAY TO PREDICT AN
EVALUATION REQUIRED ACCURATE PROGNOSIS
NO EDUCATION ON
PROPER USE OR DISPOSAL
NO FAMILY NOTIFICATION
REQUIRED
NO 1D NECESSARY
FOR PICKUP
suite th
a
NO PROTECTION FROM
means ABUSE
NO DOGTOR OR NURSE
IS PRESENT
rE a THESE ARE ONLY SOME OF THE FLAWS
im IN BILLS WHICH LEGALIZE ASSISTED SUICIDE
South | Citizens Against
oskote, Assisted Suicide
2017 Ai
lysis of Proposed South Dakota Initiated Measure
to Permit Doctor-Prescribed Suicide
The South Dakota Initiated Measure would permit a physician to prescribe "medication
for a patient to self-administer "to end the patient’ life in a humane and dignified manner."
Many people assume that this would be "
peacefully away." But that is totally false
pill" that a patient would take and then "slip
Jn Oregon, the vast majority of prescriptions for "death with dignity" are for secobarbital (a
sedative). For use as a sedative, the usual dosage is one capsule. The usual prescription under
‘bed suicide law is for 90 to 100 eapsutes,?
the state'y doctor-pres
Under the South Dakota initiated measure:
Physi
ns could preseribe a lethal overdose of drugs to patients who could live for many years.
Proponents of doctor-prescribed suicide invariably point to the requirement that a person must be
terminally ill to obtain the prescription for what they call "death with dignity.” They further explain
that the person must have been diagnosed with a six-month or less life expectancy. They call this a
safeguard
But they leave out the Fact that, in the proposed South Dakota law — as well as in all the assisted-
suicide laws that have passed in the various states ~ the definition of "terminal" allows doctors to
prescribe lethal drugs to individuals even if the patients could live for many years,”
This is because the South Dakota measure defines "terminal disease” as an incurable or irreversible
disease that will "produce death within six months."* But it does not specify that death will occur
with or without appropriate treatment.
There is documentation that this has occurred under Oregon’s assisted suicide law. In official
reports from Oregon, diabetes is noted as the underlying terminal condition that made the patient
eligible for a lethal prescription.’ If insulin-dependent diabetics do not take insulin, they will die
within six months, So, they meet the requirements for the definition of "terminal." If they do
take the medication. they can live for many years.
Another such case was described by Dr. Charles Blanke, an oncologist and professor of medicine
at Oregon Health and Science University. He explained that a young woman with Hodgkin
lymphoma had a 90 percent chance of living for decades with recommended treatment, The
woman, however, refused the treatment. "That was a very challenging situation," he said. "You
have to ask yourself, "Why doesn’t that patient want to take a relatively non-toxic treatment and
live for another seven decades?” Blanke ended up prescribing the deadly overdose for the
wont anyway.
Should doctors he able io prescribe assisted suicide for patients who could live for many years?
Assisted suicide would be transformed from a crime into a "medical treatment.”
This would cause emotional and financial pressure on patients. It would give insurance programs the
‘opportunity to cut costs since they could deny payment for treatments that patients need and want
while approving payment for the Far less eostly prescription for a lethal drug overdose.
‘This has happened in states that permit doctor-preseribed suicide.
Referring to payment tor assisted suicide, the Oregon Department of Human Services explains,
‘Individual insurers determine whether the procedure is covered under their policies, just as they
do any oter medical procedure."
There is documented information about teminally ill patients in Oregon and California who were
denied coverage for treatinent by insurance providers and, instead, were told that doctor
prescribed suicide would be covered.*
In Calitornia, after finding that her insurance company would not cover the chemotherapy het
doctor had prescribed. a woman asked if assisted suicide was covered under her plan. She was
told, "Yes, we do provide that to our patients, and you would only have to pay $1.20 for the
California pays for assisted-suicide drugs obtained by MediCal patients under the state's doctor-
prescribed suicide law."
Uthe SD measure becomes law, will insurance programs do the right thing — or the cheap thing?
Severely depressed or mentally ill patients could receive doctor-preseribed suicide without
receiving any type of counseling.
Even if a patient is suffering from depression or another psychiatric or psychological disorder a
physician needs to refer a patient for counseling only "if appropriate,""! meaning that either the
z or consulting physician believes that the patient’s mental condition is "causing impaired
jucigment.”"" The patient's medical record will include a report of any determinations made during
performed.”
attendi
counselin
This provision is similar to that contained in Oregon's law where, in 2014, only 3 of the 155
patients who received lethal prescriptions were referred for a psychological evaluation." A study
about Oregon's [aw found that it "may not adequately protect all mentally ill patien
Whe wouldn't counseling be required for every patient before a doctor prescribes a lethal dose of
drugs?
‘The most marginalized individuals — poor. hardworking people — would be in particafar
danger.
“Choice” isan appealing word but inequity in health care is a harsh reatity,
The measure states that the doctor must inform the patient of all "feasible alternatives."'* However,
discussing alternatives dees not mean the patient will have the resources to access those options.
Why should the comfortably well off have a choice of treatment options while the poor are left with
the only one they can afford — doctor-preseribed suicide?
The written request for doctor-prescribed suicide could be witnessed by someone who would
gain financially from the patient's death
The written request must be witnessed by two individuals. Only one individual may not be someone
who is entitled to any portion of the patient's estate.'” Thus, one witness may be a potential heir who
is encouraging or pressuring the patient to sign the request. The second witness could be the "best
friend” of the potential heir
The written request could even be signed in the patient’s home. This places elder abuse and domestic
abuse victims in great danger since they are unlikely to share their fears with outsiders or to reveal
that they are being: pressured by family members to "choose" doctor-prescribed suicide.
Why ceun a potential heir, who would gain from the patient's death, be allowed fo witness the written
request?”
A person who would benefit financial
trom the person's death could pick up the tethal
prescription and deliver it to the patient.
‘The drugs can be dispensed to an expressly identified agent of the patient.'* A potential heir could
encourage the patient to authorize him or her to pick up the drugs for delivery to the patient's
residence.
An interpreter could inaccurately convey the patient's request as well as any statement about
feeling coerced or unduly influenced by another person.
Under the bill, a patient must be "competent," defined as the "ability to make and communicate ai
informed decision." This includes “communication through persons familiar with the patient's
manner of communicating."””
This could lead to a patient's wishes being misunderstood, misinterpreted, or disregarded. There is
‘no requirement that such communication be independently verified. Nor is there any requirement
that the interpreter be an individual who would not gain from the patient's death
How woulel anyone know if the communication accurately expresses the patient's decision?
Patients would have no protection once the assisted-suicide prescription is filled,
Like the Oregon law, the bill only addresses activities taking place until the prescription is filled.
There are no provisions to assure that the patient is competent at the time the lethal drug overdose is
taken af that he or she knowingly and willingly took the drugs.
Due to this luck of protection, the bill would place patients at enormous risk. For example, someone
‘who would benefit trom the individual's deati could trick or even force the person into taking the
fatal drugs. And no one would ever know.
Why uren'r there any sofeguards at the most important stage of the process — at the time the patient
rakes the deugs that will cause death?
Death certificates would be fa
ed.
The attending physician who wrote the prescription (who would not need to be present when the
patient takes the drugs) may sign the patient's death certificate, which "shall list the underlying
‘erminal disease as the eause of d
Isn't it ironic, that at a time when there are warnings about the danger of opioids
illing people, there is also a campaign to promote opioids to kill a certain category
of peopie?
hts Council consultant, has noted, there is a mixed
"Don't abuse opioids, because they can kill you ~ unless you have a terminal illness
and want them to kill you, in which case your overdose will be considered ‘death with
dignity."
Initiative. Section 111)
> Fora fll documented description of drugs used for doctor-prescribed suicide, see : "2016 Summary of Drugs
Used for Doctor-Prescribed Suicide." Available at: http:/www.patientstightseouncil.org/site/2017-summary-of-
Urugs-usedfor-doctor-prescribed-suicide. (Last accessed 9/15/17.)
‘See "Comparison of State Laws Permitting Doctor-Prescribed Suicide: Laws as of September 2017," Available at:
i www. patientsrightscouneil orgsite/eomparison-of state-aws-permitting-doctorpreseribed-sueide
Initiative, Section 1 (12).
* ieial repor for 2016 deaths under Oregon's Death with Dignity Act, Oregon Public Health Division, "Oregon's
Death with Dignity Act ~2016, ” pg. 1, fa. 2. Available at
hutp: public health oregon. gov/ProviderPartnerResources/EvaluationResearchyDeathwithDignityAcvDocuments!
year pdf. (Last avcesved 8/17/U7.)
* Tara Bannow, "Rural Oregonians Sill Face Death with Dignity Barriers," Bend Bulletin, Avgust 14,2017
Asailable at: brtp//6w 4 bendbutletin.com/health’5312373-15 Horegonians-can-choose-how-their-roads-end, (Last
avcessed 8/17/17.)
Oregon Dept, of Human Services, "FAQs about the Death with Dignity Act.” Available a:
hp: public-health orezon.gov/ProviderPartnerResources/EvaluationResearch/DeathwithDignityAcl Documents! faq
spat. Last aceessed 8/9/17.)
“See, for example: Bradford Richardson, "Assisted-suicide law prompts insurance company to deny coverage 10
terininally ill California woman," Washington Times, October 20, 2016. Available at
Inepe- www cashinatontimes.com/news/2016foct/20/assisted-suicide-law-prompts-insorance-company-den. (Last
accessed 8/3/17.)
Aso see: Susan Donaldson James, “Death Drugs Cause Uproar in Oregon." ABC News, August 6, 2008. Available
ahi adenews.vo.comfealth/story?id-5517497&page~I. (Last accessed 8/3/17.)
Bradtord Richardson, "ASsisted-suieide law prompts insurance company to deny coverage to terminally ill
Calitoria woman,” WFayhigion Times, October 20, 2016, Availabe at
itp: 4996 swashingtontimes.convinews/201 6/00 20/assisted-suicide-law-prompts-insurance-company-den, (Last
svessed 833/17.)
Kimberiy Leonard, "Californians Can Choose to Die ~ With the Hetp of Taxpayers,” U:S. News & World Report,
March 21, 2016. Available at: hitps:!/www.usnews.com/news/articles/2016-03-2 |/in-califoraia-zovemment-to-
ith-dignity. (Last aceessed 8/3/17.)
pich-upethe-tab-For-a
Init
Initiative, Seetion 6
Inigiative, Seetion 12 (3).
Oficial report tor 2014 deat
hip: public-health. oregon gov/ProviderParinerRe:
weit! Ppa, (Last aevessed 3/15/17.)
ive, Section 4
nler Oregon's Death with Dignity Act, p. 5. Available at
uurces/E valuationResearchDeathnwithDignity Act/Documents!
Linda Ganzini, Elizabeth R. Goy, Steven K. Dobscha, "Prevalence of depression and anxiety in patients
‘requesting physicians’ aid in dying: eross sectional survey,” British Medical Journal, Oct. 25, 2008, pp. 973-78.
'"jnitiative, Section 4 (3) (e)
"Initiative, Section 3,
"Initiative, Section 412} (b),
"Initiative, Seetion 1 (2)
© Initiative, Section 4 (12).
" Wesley J. Smith, "Stop Assisied-Suleide Opioid Abuse,
‘st Things, August 4, 2017.
Coppright © 2097
Patents Rights Couse
PO. ox 760
Stexhonvile, OH #3982
74282-3810 gr RUC ISHS
ups paontihtscouncl one
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- MonFore EvictedDocument14 pagesMonFore EvictedPat PowersNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Rounds for Senate 2024 2q FECDocument78 pagesRounds for Senate 2024 2q FECPat PowersNo ratings yet
- 2q FEC Sheryl Johnson for CongressDocument48 pages2q FEC Sheryl Johnson for CongressPat PowersNo ratings yet
- South Dakota Carbon Capture MemoDocument2 pagesSouth Dakota Carbon Capture MemoPat PowersNo ratings yet
- Sutton Disclosure 2020 Pre-PrimaryDocument6 pagesSutton Disclosure 2020 Pre-PrimaryPat Powers100% (1)
- Tony Kay Ser Pre-Primary ReportDocument9 pagesTony Kay Ser Pre-Primary ReportPat PowersNo ratings yet
- Dakota First Action - Toby Doeden AffidavitDocument11 pagesDakota First Action - Toby Doeden AffidavitPat PowersNo ratings yet
- FRC GOPPlatformSurveyDocument16 pagesFRC GOPPlatformSurveyPat PowersNo ratings yet
- 23civ24-000005 - Order To Show CauseDocument2 pages23civ24-000005 - Order To Show CausePat PowersNo ratings yet
- Sanders FEC FilingsDocument5 pagesSanders FEC FilingsPat PowersNo ratings yet
- Sutton Disclosure 2020 Pre-PrimaryDocument6 pagesSutton Disclosure 2020 Pre-PrimaryPat Powers100% (1)
- Heidi Heitkamp 2019 Year-End FEC ReportDocument55 pagesHeidi Heitkamp 2019 Year-End FEC ReportRob PortNo ratings yet
- ShadOlson SCAN0001 RedactedDocument4 pagesShadOlson SCAN0001 RedactedPat PowersNo ratings yet
- FRC DRAFT Meeting Minutes 3-14-2023Document3 pagesFRC DRAFT Meeting Minutes 3-14-2023Pat PowersNo ratings yet
- 66civ23-000155 Memorandum DecisionDocument5 pages66civ23-000155 Memorandum DecisionPat PowersNo ratings yet
- Kent Roe SdcfdisclosureDocument2 pagesKent Roe SdcfdisclosurePat PowersNo ratings yet
- FEC Termination Filing For Annette Bosworth MDDocument6 pagesFEC Termination Filing For Annette Bosworth MDPat PowersNo ratings yet
- Sutton Disclosure 2020 Pre-PrimaryDocument6 pagesSutton Disclosure 2020 Pre-PrimaryPat Powers100% (1)
- NoemopinionSCTbrf Filed 12-15-23Document59 pagesNoemopinionSCTbrf Filed 12-15-23Pat PowersNo ratings yet
- Heidi Heitkamp 2019 Year-End FEC ReportDocument55 pagesHeidi Heitkamp 2019 Year-End FEC ReportRob PortNo ratings yet
- Taffy Howard 2024 Campaign Finance DisclosureDocument2 pagesTaffy Howard 2024 Campaign Finance DisclosurePat PowersNo ratings yet
- Sutton Disclosure 2020 Pre-PrimaryDocument6 pagesSutton Disclosure 2020 Pre-PrimaryPat Powers100% (1)
- Castleberry Settlement AgreementDocument4 pagesCastleberry Settlement AgreementPat PowersNo ratings yet
- Ltr. MJJ To Johnson Const Amend Prohibit Legis Repeal or Change Initiated Measure. Darft 6.28.2023Document3 pagesLtr. MJJ To Johnson Const Amend Prohibit Legis Repeal or Change Initiated Measure. Darft 6.28.2023Pat PowersNo ratings yet
- YanktonGOP1 1Document5 pagesYanktonGOP1 1Pat PowersNo ratings yet
- Dusty Johnson October 2024 FECDocument161 pagesDusty Johnson October 2024 FECPat PowersNo ratings yet
- Schoenbeck Law Review Article On ImpeachmentDocument20 pagesSchoenbeck Law Review Article On ImpeachmentPat PowersNo ratings yet
- Zach Kovach FECDocument10 pagesZach Kovach FECPat PowersNo ratings yet
- AustinGossArrest ImpersonatingGovNoemDocument5 pagesAustinGossArrest ImpersonatingGovNoemPat PowersNo ratings yet
- SD Freedom Caucus 061223Document6 pagesSD Freedom Caucus 061223Pat PowersNo ratings yet