Download as pdf or txt
You might also like
- Process RecordingDocument3 pagesProcess Recordingdyosa 433% (9)
- UHS Pre-Enrolment Med Clearance - FinalDocument3 pagesUHS Pre-Enrolment Med Clearance - FinalMikayla DutingNo ratings yet
- Medical Auditing Training: CPMA®: Practical Application WorkbookDocument28 pagesMedical Auditing Training: CPMA®: Practical Application WorkbookAnthony El Hage100% (1)
- CASESHEETPHARMDDocument6 pagesCASESHEETPHARMDSai SharathNo ratings yet
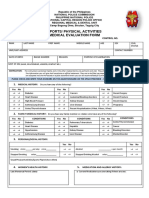
- Medical Evaluation Form 2022Document2 pagesMedical Evaluation Form 2022jimmy p. lamhi50% (2)
- Quiz Hospital DocumentationDocument5 pagesQuiz Hospital DocumentationJessica EdiosNo ratings yet
- Pre Lab Work Health AssessmentDocument11 pagesPre Lab Work Health AssessmentSarah Jane VasquezNo ratings yet
- MFC PDFDocument5 pagesMFC PDFdipmipNo ratings yet
- Gravida: Para: Ab:: Mark N/a If Not Applicable)Document11 pagesGravida: Para: Ab:: Mark N/a If Not Applicable)heahou8716No ratings yet
- Template For SOAP CasesDocument6 pagesTemplate For SOAP CasesJoudy JoudNo ratings yet
- General Assessment TemplateDocument8 pagesGeneral Assessment TemplateBob HopeNo ratings yet
- BLANK Nursing Process PaperDocument10 pagesBLANK Nursing Process PaperSNOOKI513No ratings yet
- PFT Form 2023Document2 pagesPFT Form 2023Custodial Facility Pasig CPSNo ratings yet
- Health: No Known AllergiesDocument12 pagesHealth: No Known AllergiesSeanmarie CabralesNo ratings yet
- Maklumat Penting - Atau Hospital/Klinik Swasta. - : Form Pd1Document9 pagesMaklumat Penting - Atau Hospital/Klinik Swasta. - : Form Pd1Syazwi BaharuddinNo ratings yet
- Pharmacist Workup of Drug Therapy in Pharmaceutical Care: Problem Oriented Pharmacist RecordDocument20 pagesPharmacist Workup of Drug Therapy in Pharmaceutical Care: Problem Oriented Pharmacist RecordDzaky UlayyaNo ratings yet
- Clinical Prep SheetDocument6 pagesClinical Prep Sheetapi-232466940No ratings yet
- Clinical Pathways and Variance AnalysisDocument42 pagesClinical Pathways and Variance AnalysisdrgrizahNo ratings yet
- RLE Simulation Scenario For Clinical Practice: (Care of Patients With Alterations in Oxygenation)Document12 pagesRLE Simulation Scenario For Clinical Practice: (Care of Patients With Alterations in Oxygenation)Biway RegalaNo ratings yet
- DCF FormDocument5 pagesDCF FormJEMY JOSENo ratings yet
- Pre Medical Evaluatiom Form PFT 1 PDFDocument2 pagesPre Medical Evaluatiom Form PFT 1 PDFAIEN WENDELEIH Q. CAPINPIN100% (2)
- Case Presentation Format RevisedDocument11 pagesCase Presentation Format RevisedAntonio Liezeth JaneNo ratings yet
- 2023 Spring - NURS 252-St Data SheetDocument7 pages2023 Spring - NURS 252-St Data SheetmalakajameahNo ratings yet
- PN CJM AssignmentDocument7 pagesPN CJM Assignmenttcarmen49No ratings yet
- International Ice Hockey Federation Therapeutic Use Exemption (TUE) Application FormDocument7 pagesInternational Ice Hockey Federation Therapeutic Use Exemption (TUE) Application FormDaniel PenninckNo ratings yet
- Case Presentation FormatDocument11 pagesCase Presentation FormatSweetzel MoratallaNo ratings yet
- RLE Simulation Scenario For Clinical Practice: (Care of Patients With Alterations in Oxygenation)Document13 pagesRLE Simulation Scenario For Clinical Practice: (Care of Patients With Alterations in Oxygenation)Biway RegalaNo ratings yet
- Discharge Summary 1Document1 pageDischarge Summary 1mouli poliparthiNo ratings yet
- UHS Employee Health Info FormDocument7 pagesUHS Employee Health Info FormCrystal AnnNo ratings yet
- Preschool Health Assessment FormDocument2 pagesPreschool Health Assessment FormSammi GuptaNo ratings yet
- A Guide To Clinical Case Study and Its PresentationDocument13 pagesA Guide To Clinical Case Study and Its PresentationVince Troy AquinoNo ratings yet
- Care Plan For CHFDocument9 pagesCare Plan For CHFJon Djchimz IsidroNo ratings yet
- 01.17bmQT10 Health Examination ReportDocument6 pages01.17bmQT10 Health Examination ReportKita 09No ratings yet
- PFT Medical Evaluation Form 1Document3 pagesPFT Medical Evaluation Form 1Dexter VenguaNo ratings yet
- Format For Medical FitnessDocument4 pagesFormat For Medical FitnessParas JaniNo ratings yet
- Health ScreeningDocument3 pagesHealth Screeningpixelkum1No ratings yet
- Patient Counseling FormDocument2 pagesPatient Counseling FormMarifuddin Hussaini50% (2)
- Nurse Report Sheet OriginalDocument2 pagesNurse Report Sheet Originalhvera01No ratings yet
- Must Use Forms Provided Must Be TypedDocument8 pagesMust Use Forms Provided Must Be TypedVincent Karimi GichimuNo ratings yet
- Philippine Dental Association Covid 19 Monitoring FormDocument1 pagePhilippine Dental Association Covid 19 Monitoring Formrhusolano rhusolanoNo ratings yet
- Pat Semester 2Document27 pagesPat Semester 2api-300946501No ratings yet
- Federation Internationale de Motocyclisme Therapeutic Use Exemption (TUE) Application FormDocument7 pagesFederation Internationale de Motocyclisme Therapeutic Use Exemption (TUE) Application FormTessa HernandezNo ratings yet
- Dho-Itr - 6yrs Old and Above-RawDocument4 pagesDho-Itr - 6yrs Old and Above-RawLouises Sayson-OlayanNo ratings yet
- PDF TextDocument1 pagePDF TextsayyedatfatmaNo ratings yet
- Idoc - Pub Medical Check Up FormDocument4 pagesIdoc - Pub Medical Check Up FormBobly SweaggerNo ratings yet
- Care Plan Oct 23 380Document18 pagesCare Plan Oct 23 380api-256360167No ratings yet
- 1-Thyroid Profile Total - PO1106326185-399Document6 pages1-Thyroid Profile Total - PO1106326185-399Arup KumarNo ratings yet
- Case Study of HerniaDocument9 pagesCase Study of HerniaᏚᏔᎬᎬᎿ ᎶᎥᎡᏞNo ratings yet
- Case Study FormatDocument4 pagesCase Study Formatychinguile1No ratings yet
- Clinical Judgment Plan of Care Long FormDocument12 pagesClinical Judgment Plan of Care Long Formapi-699835864No ratings yet
- The Turkey Book - An Introductory Manual For The WardsDocument147 pagesThe Turkey Book - An Introductory Manual For The WardsThe Physician Assistant LifeNo ratings yet
- Care Plan TemplateDocument12 pagesCare Plan TemplateemipNo ratings yet
- 57035d7950aaf-BCCI TUE Application Form V1.2015 PDFDocument3 pages57035d7950aaf-BCCI TUE Application Form V1.2015 PDFbhavyapruthiNo ratings yet
- Medical Examination 5Document1 pageMedical Examination 5Melanie AgustinNo ratings yet
- Nursing Health HistoryDocument5 pagesNursing Health HistoryAsh JaneNo ratings yet
- 325 Care Plan - 1Document17 pages325 Care Plan - 1mp1757No ratings yet
- Citizens CharterDocument29 pagesCitizens CharterHarold Paulo MejiaNo ratings yet
- Clinical Treatment PDFDocument1 pageClinical Treatment PDFDanielle YoderNo ratings yet
- Case LoadDocument3 pagesCase LoadFrancis Raphael PitogoNo ratings yet
- Ob/Neonatal Liability IssuesDocument107 pagesOb/Neonatal Liability IssuesCamille DiCostanzo PickelNo ratings yet
- Symptoms in the Pharmacy: A Guide to the Management of Common IllnessFrom EverandSymptoms in the Pharmacy: A Guide to the Management of Common IllnessNo ratings yet
- HuxleyDocument5 pagesHuxleyAlessandro IevaNo ratings yet
- Environmental Activities PP1 Term 2Document9 pagesEnvironmental Activities PP1 Term 2wallyNo ratings yet
- Lycanthropy From Nebuchadnezzar To Modern Times: ReichDocument2 pagesLycanthropy From Nebuchadnezzar To Modern Times: Reichoutdash2No ratings yet
- Chapter05 Ethics in NegotiationDocument27 pagesChapter05 Ethics in NegotiationAmmar AliNo ratings yet
- A Review of The de Ja' Vu Experience: Alan S. BrownDocument20 pagesA Review of The de Ja' Vu Experience: Alan S. BrownkatiaNo ratings yet
- Mothers LoveDocument45 pagesMothers LovePoonamSidhu53% (19)
- Day 5 - Foundation of Special and Inclusive EducationDocument83 pagesDay 5 - Foundation of Special and Inclusive EducationDarlen May DalidaNo ratings yet
- Wier, Kelley, Formal Observation, Fi, 3-12-15, s4Document4 pagesWier, Kelley, Formal Observation, Fi, 3-12-15, s4api-242012292No ratings yet
- Urbanist Aug Sept 2012 Mott SmithDocument1 pageUrbanist Aug Sept 2012 Mott Smithmaison_orionNo ratings yet
- Concept MapDocument11 pagesConcept MapPak WaldiNo ratings yet
- ENGLISH Lesson Plan 1Document6 pagesENGLISH Lesson Plan 1missfafauNo ratings yet
- Tugasan/Assignment ABPS2103 Cross-Cultural Psychology/ September 2022 Semester - Specific Instruction / Arahan KhususDocument13 pagesTugasan/Assignment ABPS2103 Cross-Cultural Psychology/ September 2022 Semester - Specific Instruction / Arahan KhususHf CreationNo ratings yet
- Terminal ReportDocument9 pagesTerminal ReportKaye MamisaoNo ratings yet
- Marie Diamond Bonus Gift Inner Diamond Meditation Plus Audio LinkDocument7 pagesMarie Diamond Bonus Gift Inner Diamond Meditation Plus Audio Linkbilldockto_141471063No ratings yet
- CHAPTER 6 Training and Development EmployeesDocument48 pagesCHAPTER 6 Training and Development EmployeesAngelo MolinaNo ratings yet
- Modul PembahasanDocument337 pagesModul PembahasanMuhammad Syamsir AnchyNo ratings yet
- Direct and Indirect Speech Reduced SizeDocument10 pagesDirect and Indirect Speech Reduced SizeChrista van StadenNo ratings yet
- Results Management in Norwegian Development CooperationDocument36 pagesResults Management in Norwegian Development CooperationVgslavonNo ratings yet
- Shining in Plain View John Wheeler Sample PDFDocument28 pagesShining in Plain View John Wheeler Sample PDFPeter CohenNo ratings yet
- Sruthi ResumeDocument2 pagesSruthi Resumesruthi kuppiliNo ratings yet
- ASTRAL TRAVEL - 10 Astral Secrets Astral PR - Mkunda DevaDocument8 pagesASTRAL TRAVEL - 10 Astral Secrets Astral PR - Mkunda DevaRandomizer100% (2)
- Eros, Thanatos and The Negation of The Will-To-Live in Larkin's PoetryDocument7 pagesEros, Thanatos and The Negation of The Will-To-Live in Larkin's PoetrythebigfNo ratings yet
- Berrios Psicopatologia HistoricaDocument24 pagesBerrios Psicopatologia HistoricaEleoner RamirezNo ratings yet
- Undergraduate LO RubricsDocument5 pagesUndergraduate LO RubricsSafaruddin Al AfganiNo ratings yet
- Set Achievable and Appropriate Learning Outcomes That Aligned With Learning CompetenciesDocument4 pagesSet Achievable and Appropriate Learning Outcomes That Aligned With Learning Competenciesmhlq14100% (1)
- Persuasion: Jane Austen'SDocument18 pagesPersuasion: Jane Austen'SManshi YadavNo ratings yet
- Robert Gagné 9 Events of LearningDocument2 pagesRobert Gagné 9 Events of LearningDina Ikrama PutriNo ratings yet
- 3141007-Summer 2022Document1 page3141007-Summer 2022Manthan PanchalNo ratings yet
- Ed 105 Chapter 4 6 ActivitiesDocument5 pagesEd 105 Chapter 4 6 ActivitiesLino jay Ombega 2BNo ratings yet