Download as pdf or txt
You might also like
- COSHH Risk Assessment For RoundUPDocument2 pagesCOSHH Risk Assessment For RoundUPRonnie Murphy Knotweed Surveyor50% (2)
- Differential ProtectionDocument24 pagesDifferential ProtectionFaouzi Tlemcen100% (2)
- Production of Vitamin B12Document12 pagesProduction of Vitamin B12Sundaralingam Raj50% (2)
- In Target PDCD1 905 548/357 548/337Document2 pagesIn Target PDCD1 905 548/357 548/337Jane WongNo ratings yet
- Andritz Hydro Protection PDFDocument118 pagesAndritz Hydro Protection PDFGuntur Rizky KautsarNo ratings yet
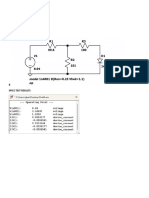
- Modelling Parallel Operation of Power Rectifiers With PspiceDocument8 pagesModelling Parallel Operation of Power Rectifiers With PspiceAl-amin AlexNo ratings yet
- Spam 150 C Motor Protection Relay: User S Manual and Technical DescriptionDocument13 pagesSpam 150 C Motor Protection Relay: User S Manual and Technical DescriptionrpshvjuNo ratings yet
- Model: REM543-CG214CAAA: Generator Protection RelayDocument7 pagesModel: REM543-CG214CAAA: Generator Protection RelaymurugananthameeeNo ratings yet
- Multispan TC-19Document4 pagesMultispan TC-19Karan SolankiNo ratings yet
- Molecular Minimal Residual Disease Detection in Acute Myeloid LeukemiaDocument42 pagesMolecular Minimal Residual Disease Detection in Acute Myeloid LeukemiaANo ratings yet
- PROTEKSIDocument24 pagesPROTEKSIchris.lutang93No ratings yet
- TitoDocument3 pagesTitoKiwii CodmNo ratings yet
- Gen First Sync Procedure - Rev01Document12 pagesGen First Sync Procedure - Rev01O P Sridharan PerumalNo ratings yet
- Test Report: Winding DF & CAP (Tan δ)Document2 pagesTest Report: Winding DF & CAP (Tan δ)JRC Testing100% (2)
- CSEProT170 - 1 DifferentialDocument9 pagesCSEProT170 - 1 Differentialtesting.rndNo ratings yet
- DT-96 / DT-72 / DT-48: Auto-Tune Pid Temperature ControllerDocument4 pagesDT-96 / DT-72 / DT-48: Auto-Tune Pid Temperature ControllerS ANo ratings yet
- MAR DS LPO MTX Report ENDocument11 pagesMAR DS LPO MTX Report ENSatriyaNo ratings yet
- Bus Bar ProtectionDocument18 pagesBus Bar ProtectionTanmayNo ratings yet
- At03 Z1paDocument64 pagesAt03 Z1paHeshan KamaljithNo ratings yet
- Airtran Southwest Question: Delay in Minutes For Two Airlines Have Been Given. Does The Average Delay For Both The Airlines Differ?Document11 pagesAirtran Southwest Question: Delay in Minutes For Two Airlines Have Been Given. Does The Average Delay For Both The Airlines Differ?Jaydeep BairagiNo ratings yet
- Megger SMRT Differential Relay Settings HelpDocument15 pagesMegger SMRT Differential Relay Settings Helpmuhammad awaisNo ratings yet
- Iwc750 TwinDocument1 pageIwc750 Twinprintstyle_designNo ratings yet
- Triatmo Budiyuwono SPJP (K), FIHA, FAPSICDocument40 pagesTriatmo Budiyuwono SPJP (K), FIHA, FAPSICganangahimsaNo ratings yet
- Poster GNB I Cong Naz Bioing 2008 Conf Effects of Intraventricular Pathologies Described by A Lumped Parameter Computer ModelDocument1 pagePoster GNB I Cong Naz Bioing 2008 Conf Effects of Intraventricular Pathologies Described by A Lumped Parameter Computer ModelFabio PiedimonteNo ratings yet
- EP0225787A2Document67 pagesEP0225787A2Buddy MyoNo ratings yet
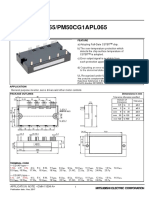
- PM50CG1AP065/PM50CG1APL065Document9 pagesPM50CG1AP065/PM50CG1APL065Omar SandreNo ratings yet
- Ame8500aeetaa24 To Ame8501ceftdf46Document12 pagesAme8500aeetaa24 To Ame8501ceftdf46gotcha75No ratings yet
- Test Performed By: SWCC Witness: SWCC Engineer: Date of Test Name: Jabirali. P Rashed A.Murshed 26-DEC-2020 SignatureDocument5 pagesTest Performed By: SWCC Witness: SWCC Engineer: Date of Test Name: Jabirali. P Rashed A.Murshed 26-DEC-2020 SignatureAnonymous dH3DIEtzNo ratings yet
- DR Thomas SpreenDocument13 pagesDR Thomas SpreenLuisNo ratings yet
- Modul Untuk FisikaDocument38 pagesModul Untuk Fisikaimran,stNo ratings yet
- Xpert BCR-ABL Ultra Assay-ENGLISH PI 302-0738 Rev. C - 1Document32 pagesXpert BCR-ABL Ultra Assay-ENGLISH PI 302-0738 Rev. C - 1AndrianRakhmatsyahNo ratings yet
- 07 - S WINDECKER Biological Heart Valves MitraClip TAVIDocument44 pages07 - S WINDECKER Biological Heart Valves MitraClip TAVIA.M.B M.B.M.ENo ratings yet
- ملفDocument133 pagesملفsiso hegoNo ratings yet
- IcdDocument79 pagesIcdΔήμητρα ΠαυλοπούλουNo ratings yet
- UC2842B/3B/4B/5B UC3842B/3B/4B/5B: High Performance Current Mode PWM ControllerDocument15 pagesUC2842B/3B/4B/5B UC3842B/3B/4B/5B: High Performance Current Mode PWM ControllertoajuiceNo ratings yet
- Identification of Induction Motor ParametersDocument6 pagesIdentification of Induction Motor ParameterstrebeardNo ratings yet
- GTx108 F SubmittalDataDocument4 pagesGTx108 F SubmittalDataNic DziemianNo ratings yet
- Relay Settings - 10.0MW Jogipet SPV PlantDocument3 pagesRelay Settings - 10.0MW Jogipet SPV PlantVamsi PavuluriNo ratings yet
- 1) Negative Sequence Test: Test Report For Differential Protection Relay 7um62 PTD/7UM62Document8 pages1) Negative Sequence Test: Test Report For Differential Protection Relay 7um62 PTD/7UM62subhasish03ee6301No ratings yet
- Timer: SpecificationsDocument2 pagesTimer: SpecificationsBIOMED HCCNo ratings yet
- ANSI ProtectionDocument38 pagesANSI ProtectionAlexandru IoanNo ratings yet
- Report of UsDocument7 pagesReport of UsMd Usman KhanNo ratings yet
- BtdnangcaoDocument5 pagesBtdnangcaoTuấn Vũ VươngNo ratings yet
- Differential Protection (7UT) : Dynamic Tests, TestsDocument24 pagesDifferential Protection (7UT) : Dynamic Tests, TestsWrya SaeedNo ratings yet
- Jee Main Result PDFDocument1 pageJee Main Result PDFKrish MehtaNo ratings yet
- 26 - 4 - 7UT6 Tests - enDocument24 pages26 - 4 - 7UT6 Tests - enmohamed tinoneNo ratings yet
- PG Test-Instrument-PSWRDocument12 pagesPG Test-Instrument-PSWRyogesh pandeyNo ratings yet
- Madhucon Relay Settings - R2 - 31 03 12Document27 pagesMadhucon Relay Settings - R2 - 31 03 12Ramanjaneya ReddyNo ratings yet
- P630 Testing ProcedureDocument18 pagesP630 Testing Procedure1981todurkar100% (1)
- Complete DDR2, DDR3, DDR3L, and LPDDR3 Memory Power Solution Synchronous Buck Controller, 2-A LDO, With Buffered ReferenceDocument30 pagesComplete DDR2, DDR3, DDR3L, and LPDDR3 Memory Power Solution Synchronous Buck Controller, 2-A LDO, With Buffered Referencesalahudeen03No ratings yet
- Numerical Differential Protection of 220/132KV, 250 MVA Auto Transformer Using Siemens Make Differential Relay 7UT612Document6 pagesNumerical Differential Protection of 220/132KV, 250 MVA Auto Transformer Using Siemens Make Differential Relay 7UT612AnilNo ratings yet
- Reformer Welding Joint SummaryDocument1 pageReformer Welding Joint SummaryPraveen RANANo ratings yet
- SEL-387 - Main-2 - APM 2023Document2 pagesSEL-387 - Main-2 - APM 2023Ruel de VillaNo ratings yet
- Pruebas PTs Ritz, Transf SO 119564 - TestReport-1Document1 pagePruebas PTs Ritz, Transf SO 119564 - TestReport-1Alexander FelizNo ratings yet
- L90 BlankDocument3 pagesL90 Blankhikaru20No ratings yet
- Design Qualification Test ReportDocument38 pagesDesign Qualification Test ReportHareth MRAIDINo ratings yet
- CL Analyzer: Coagulometric, Chromogenic and Immunological AssaysDocument2 pagesCL Analyzer: Coagulometric, Chromogenic and Immunological AssaysEdwinNo ratings yet
- '"ljirdep: .. Intra Ofrice NoteDocument1 page'"ljirdep: .. Intra Ofrice NotevemncnsNo ratings yet
- A L702 Service G Uid E: RviceDocument26 pagesA L702 Service G Uid E: RvicePIOTR VALENTINENo ratings yet
- TMP 592 BDocument4 pagesTMP 592 BFrontiersNo ratings yet
- The Fourth Terminal: Benefits of Body-Biasing Techniques for FDSOI Circuits and SystemsFrom EverandThe Fourth Terminal: Benefits of Body-Biasing Techniques for FDSOI Circuits and SystemsSylvain ClercNo ratings yet
- Emergency Meds (Shock, Cardiac Arrest, Anaphylaxis)Document1 pageEmergency Meds (Shock, Cardiac Arrest, Anaphylaxis)aymenNo ratings yet
- Chronic Myelomonocytic LeukemiaDocument17 pagesChronic Myelomonocytic LeukemiaaymenNo ratings yet
- Cerebrovascular AccidentDocument5 pagesCerebrovascular AccidentaymenNo ratings yet
- Tear Cytokines As Biomarkers For Chronic GVHDDocument7 pagesTear Cytokines As Biomarkers For Chronic GVHDaymenNo ratings yet
- Future Outlook of Checkpoint Receptor InhibitorsDocument3 pagesFuture Outlook of Checkpoint Receptor InhibitorsaymenNo ratings yet
- Transfusion Related Immunomodulation (Trim)Document14 pagesTransfusion Related Immunomodulation (Trim)aymenNo ratings yet
- General Transfusion Practice Quiz For Rotating Medical StaffDocument3 pagesGeneral Transfusion Practice Quiz For Rotating Medical StaffaymenNo ratings yet
- A-Gvhd M.saeedDocument20 pagesA-Gvhd M.saeedaymenNo ratings yet
- Transfusion Related Immunomodulation (Trim) : By/ Aymen OmerDocument14 pagesTransfusion Related Immunomodulation (Trim) : By/ Aymen OmeraymenNo ratings yet
- Thrombolytics - Hematology - Medbullets Step 1Document5 pagesThrombolytics - Hematology - Medbullets Step 1aymen100% (1)
- Arterial Blood Gases (ABG) : Shaza AlyDocument56 pagesArterial Blood Gases (ABG) : Shaza AlyaymenNo ratings yet
- Acute Lymphoblastic Leukemia Prof.S.Tito'S Unit M5 Dr.M.ArivumaniDocument47 pagesAcute Lymphoblastic Leukemia Prof.S.Tito'S Unit M5 Dr.M.ArivumaniaymenNo ratings yet
- Hematological Manifestations of Connective Tissue Disorders: Aymen OmerDocument69 pagesHematological Manifestations of Connective Tissue Disorders: Aymen OmeraymenNo ratings yet
- Lecture Hemophilia and Thrombocytopenic PurpuraDocument55 pagesLecture Hemophilia and Thrombocytopenic PurpuraaymenNo ratings yet
- 39notes Clinical PathologyDocument9 pages39notes Clinical PathologyaymenNo ratings yet
- Prof. M. Rushdi: PolycythemiaDocument6 pagesProf. M. Rushdi: PolycythemiaaymenNo ratings yet
- Type of MutationDocument16 pagesType of Mutationaymen100% (1)
- Location Gold Standard Current Practice: Thrombophilia Teaching Points10/19/2005 (JGP)Document2 pagesLocation Gold Standard Current Practice: Thrombophilia Teaching Points10/19/2005 (JGP)aymenNo ratings yet
- ECG Interpretations GoodDocument104 pagesECG Interpretations GoodaymenNo ratings yet
- Anticoagulation PharmacologyDocument36 pagesAnticoagulation PharmacologyaymenNo ratings yet
- Updates For Haploidentical Hematopoietic Transplantation OutcomesDocument46 pagesUpdates For Haploidentical Hematopoietic Transplantation OutcomesaymenNo ratings yet
- Ebook V1 MullenaxDocument38 pagesEbook V1 MullenaxRob Hammer100% (1)
- Cleansing Enema: By: Tanti A.BDocument18 pagesCleansing Enema: By: Tanti A.BWidya PutriNo ratings yet
- A Review On The Ksheerdhooma - A Unique Modality of PanchakarmaDocument7 pagesA Review On The Ksheerdhooma - A Unique Modality of PanchakarmaIJRASETPublicationsNo ratings yet
- GDPDocument13 pagesGDPQF Felipe González100% (1)
- Kimera Exosomes, Kimera Labs, Inc. - 649343 - 09:01:2023 - FDADocument1 pageKimera Exosomes, Kimera Labs, Inc. - 649343 - 09:01:2023 - FDAseenfgNo ratings yet
- 3d Swot AnalysisDocument1 page3d Swot Analysisapi-491306234No ratings yet
- Food Safety BrazilDocument10 pagesFood Safety BrazilAdil KaukabNo ratings yet
- 〈1382〉 Assessment of Elastomeric Component Functional Suitability in Parenteral Product Packaging Delivery SystemsDocument8 pages〈1382〉 Assessment of Elastomeric Component Functional Suitability in Parenteral Product Packaging Delivery SystemsMehran ImaniNo ratings yet
- A2 Journal Front PageDocument1 pageA2 Journal Front PageMichelle RogersNo ratings yet
- December 2023 Final Upload Lyst2146Document190 pagesDecember 2023 Final Upload Lyst2146anshuman kumarNo ratings yet
- AIIMS Jodhpur Juniour Residents NoticeDocument4 pagesAIIMS Jodhpur Juniour Residents NoticeVijaya sharmaNo ratings yet
- Hyperkalemia Approach AND Management: Dr. Renuka RayanaDocument38 pagesHyperkalemia Approach AND Management: Dr. Renuka RayanaSap Modules100% (1)
- Thyroid CytologyDocument36 pagesThyroid CytologyNaglaa RamadanNo ratings yet
- Meg Acet in AnorexiaDocument45 pagesMeg Acet in AnorexiaRaina MohakNo ratings yet
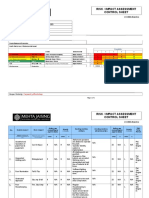
- Risk / Impact Assessment Control Sheet: CC/EHS/RA/014 ContractDocument4 pagesRisk / Impact Assessment Control Sheet: CC/EHS/RA/014 Contractsaurabh juwatkarNo ratings yet
- Avatar Identification and Problematic GamingDocument7 pagesAvatar Identification and Problematic GamingAndreaNo ratings yet
- Studi Performa Umum Tubuh Dan Status Fisiologis Kuda SumbaDocument7 pagesStudi Performa Umum Tubuh Dan Status Fisiologis Kuda SumbaMitha AristaNo ratings yet
- ICoC Signatory Companies - October 2011Document78 pagesICoC Signatory Companies - October 2011Feral JundiNo ratings yet
- p450 Table Oct 11 2009Document2 pagesp450 Table Oct 11 2009Naresh BabuNo ratings yet
- Ipo 21 1 034Document3 pagesIpo 21 1 034Y.rajuNo ratings yet
- Outline of Dissertation On ObesityDocument16 pagesOutline of Dissertation On ObesityLavarn PillaiNo ratings yet
- Healthy Body Systems PowerPointDocument42 pagesHealthy Body Systems PowerPointJianming WangNo ratings yet
- Mucolytics, Expectorants, and Mucokinetic MedicationsDocument7 pagesMucolytics, Expectorants, and Mucokinetic MedicationsDhayu Mart Hindrasyah PandiaNo ratings yet
- Roleplay JonglishDocument2 pagesRoleplay JonglishNeeyach HandayaniNo ratings yet
- CABONGA AN NHS GJHSPv2018.10.24Document40 pagesCABONGA AN NHS GJHSPv2018.10.24Halem Laroya LucernasNo ratings yet
- Injury Statistics SheetDocument4 pagesInjury Statistics SheetEslam IsmaeelNo ratings yet
- Enjoy Your Freebie!: What'S in This PDF?Document9 pagesEnjoy Your Freebie!: What'S in This PDF?Pramudita DinantiNo ratings yet
- Vaporisors PDFDocument8 pagesVaporisors PDFaksinuNo ratings yet