Download as docx, pdf, or txt
You might also like
- AOTA Exam PrepDocument2 pagesAOTA Exam PrepKenny ClayNo ratings yet
- CBTDocument238 pagesCBTHarronjardinico Jardinico88% (8)
- Opening A Private Practice in Occupational Therapy: Earn .1 Aota CeuDocument9 pagesOpening A Private Practice in Occupational Therapy: Earn .1 Aota CeuRey John MonjeNo ratings yet
- MOHOST InformationDocument1 pageMOHOST InformationRichard FullertonNo ratings yet
- 2 Introduction To TheoryDocument14 pages2 Introduction To TheoryNurul Izzah Wahidul AzamNo ratings yet
- Aota Professional Development Tool SheetDocument2 pagesAota Professional Development Tool Sheetapi-382638519No ratings yet
- AOTA Evidence-Based Practice Project CAP Worksheet Evidence Exchange Last Updated: 8/25/2016Document7 pagesAOTA Evidence-Based Practice Project CAP Worksheet Evidence Exchange Last Updated: 8/25/2016Marina ENo ratings yet
- Case Study For Hepatitis BDocument24 pagesCase Study For Hepatitis BEmma Mariz Bernas Garcia67% (6)
- Program ProposalDocument17 pagesProgram Proposalapi-582621575No ratings yet
- The Application of Assessment and Evaluation Procedure in Using Occupation Centered PracticeDocument55 pagesThe Application of Assessment and Evaluation Procedure in Using Occupation Centered PracticeAswathi100% (2)
- Functional Assessment: DR Sonali Soumyashree BPT, MPT (Neurology) Lecturer, GDGUDocument15 pagesFunctional Assessment: DR Sonali Soumyashree BPT, MPT (Neurology) Lecturer, GDGUSonali Soumyashree100% (2)
- OT Practice December 17 IssueDocument24 pagesOT Practice December 17 IssueThe American Occupational Therapy Association100% (1)
- OT10 - Principled Ot PraticeDocument20 pagesOT10 - Principled Ot PraticeAnnbe BarteNo ratings yet
- ParentingDocument29 pagesParentingaufdecken 5No ratings yet
- Barthel vs. FIMDocument5 pagesBarthel vs. FIMFrancisco CampoverdeNo ratings yet
- Occupational Therapy Case Study AssignmentDocument9 pagesOccupational Therapy Case Study Assignmentapi-395143739100% (2)
- Occupations Across The LifespanDocument6 pagesOccupations Across The LifespanMary Elizabeth JoyceNo ratings yet
- Introducing The Leadership in Enabling Occupation (LEO) ModelDocument6 pagesIntroducing The Leadership in Enabling Occupation (LEO) ModelPatricia Jara Reyes100% (1)
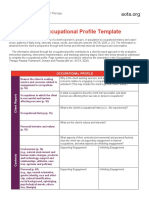
- AOTA Occupational Profile TemplateDocument2 pagesAOTA Occupational Profile TemplateYayan100% (1)
- Wee FimDocument9 pagesWee FimdeffyNo ratings yet
- Canadian Journal of Occupational TherapyDocument9 pagesCanadian Journal of Occupational TherapyFrancesca GozmanNo ratings yet
- 500 10 Ferro 10 Alto SilicioDocument90 pages500 10 Ferro 10 Alto SilicioAdams GodoyNo ratings yet
- PTFL - Ebp FinalDocument11 pagesPTFL - Ebp Finalapi-488558620No ratings yet
- Cimt and NDT Proposal-2 AltDocument10 pagesCimt and NDT Proposal-2 Altapi-487111274No ratings yet
- Placement HandbookDocument551 pagesPlacement HandbookAdonis GaleosNo ratings yet
- Implementing Occupation-Based PracticeDocument10 pagesImplementing Occupation-Based Practiceapi-392268685No ratings yet
- Physical and Occupational Therapists: Guide To Treating Osteogenesis ImperfectaDocument32 pagesPhysical and Occupational Therapists: Guide To Treating Osteogenesis ImperfectaAshari Fisio18No ratings yet
- PTH 870-Occupational TherapyDocument13 pagesPTH 870-Occupational Therapyapi-551496110100% (1)
- PSI Policy Document - Guidelines For The Employment of Assistant PsychologistsDocument14 pagesPSI Policy Document - Guidelines For The Employment of Assistant Psychologistsricosadie1No ratings yet
- The Performance Quality Rating Scale (PQRS) : Reliability, Convergent Validity, and Internal Responsiveness For Two Scoring SystemsDocument8 pagesThe Performance Quality Rating Scale (PQRS) : Reliability, Convergent Validity, and Internal Responsiveness For Two Scoring SystemsCarol AlvaradoNo ratings yet
- Development of Selective Sustained Atten PDFDocument33 pagesDevelopment of Selective Sustained Atten PDFJordan Franco Zarate BalbinNo ratings yet
- Occupational Therapy Rehabilitation Paraplegic PatientDocument7 pagesOccupational Therapy Rehabilitation Paraplegic PatientAlina PasăreNo ratings yet
- The Effect of Co-Op Approach in Improving Visual Motor Integration Skills in Children With Learning DisabilityDocument7 pagesThe Effect of Co-Op Approach in Improving Visual Motor Integration Skills in Children With Learning DisabilityIJAR JOURNALNo ratings yet
- Game Design Abstract 2014Document2 pagesGame Design Abstract 2014Nambirajan VanamamalaiNo ratings yet
- Occupational AdaptationDocument5 pagesOccupational AdaptationVASH12345100% (1)
- FRIT 7232 Technology Assessment Plan: Millicent Bess-Frazier Catherine Ball Audra Youngblood Adrian GibsonDocument6 pagesFRIT 7232 Technology Assessment Plan: Millicent Bess-Frazier Catherine Ball Audra Youngblood Adrian GibsonAshley YoungbloodNo ratings yet
- AnkyloglosiaDocument18 pagesAnkyloglosiayngallo910No ratings yet
- Assistive Technology Devices To Help With Everday Living FactsheetDocument10 pagesAssistive Technology Devices To Help With Everday Living FactsheetNikos ChalkiasNo ratings yet
- Ebp PaperDocument16 pagesEbp Paperapi-583545759No ratings yet
- School BasedOccupationalTherapyduringCOVID 19Document12 pagesSchool BasedOccupationalTherapyduringCOVID 19Ligia SendreaNo ratings yet
- Integration of Medication Management Into Occupational Therapy PracticeDocument7 pagesIntegration of Medication Management Into Occupational Therapy PracticeManuel PérezNo ratings yet
- CPPFFFFFDocument4 pagesCPPFFFFFEdu Edu100% (1)
- PB NDIS Assistive Technology, Home Modifications and Consumables Code Guide 2023-24 v1.0Document35 pagesPB NDIS Assistive Technology, Home Modifications and Consumables Code Guide 2023-24 v1.0ayawe888888No ratings yet
- AprJul2017 PublicReportDocument130 pagesAprJul2017 PublicReportAgnes Claudia100% (1)
- Normalisation Process Theory A Framework For Developing, Evaluating and Implementing Complex InterventionsDocument12 pagesNormalisation Process Theory A Framework For Developing, Evaluating and Implementing Complex InterventionsTran Ngoc TienNo ratings yet
- Study ResourcesDocument3 pagesStudy Resourcesapi-405162391No ratings yet
- Hazley Jarrett Jordan-Final Cimt Systematic Review AltDocument14 pagesHazley Jarrett Jordan-Final Cimt Systematic Review Altapi-518986604No ratings yet
- Wheelchair Bowling - AnaDocument3 pagesWheelchair Bowling - Anaapi-541744798No ratings yet
- Occupational Therapy and Mental Health 1Document18 pagesOccupational Therapy and Mental Health 1Roman -No ratings yet
- Position Paper OT For People With LDDocument10 pagesPosition Paper OT For People With LDLytiana WilliamsNo ratings yet
- Mobility and Functional Assessment ToolsDocument4 pagesMobility and Functional Assessment Toolssonya63265No ratings yet
- Pool Activity Level (PAL) Instrument For Occupational ProfilingDocument35 pagesPool Activity Level (PAL) Instrument For Occupational ProfilingAngela GohNo ratings yet
- AOTA Telerehabilitation Position PaperDocument8 pagesAOTA Telerehabilitation Position PaperBill WongNo ratings yet
- Understanding Occupational Transitions in Forced Migration The Importance of Life Skills in Early Refugee ResettlementDocument11 pagesUnderstanding Occupational Transitions in Forced Migration The Importance of Life Skills in Early Refugee ResettlementAlejandroAndrésAlvarezContrerasNo ratings yet
- Client-Centered AssessmentDocument4 pagesClient-Centered AssessmentHon “Issac” KinHoNo ratings yet
- Functional Capacity Evaluation: Occupational Therapy's Role inDocument2 pagesFunctional Capacity Evaluation: Occupational Therapy's Role inramesh babu100% (1)
- Occt 526 - Child-Based PicoDocument14 pagesOcct 526 - Child-Based Picoapi-291380671No ratings yet
- Dementia Care PracticeDocument68 pagesDementia Care PracticeZekel HealthcareNo ratings yet
- Advancing Occupational Equity and Occupational Rights Action On The Social Determinants of HealthDocument23 pagesAdvancing Occupational Equity and Occupational Rights Action On The Social Determinants of Healthvalentina hernandezNo ratings yet
- Ethics Occupational TherapyDocument7 pagesEthics Occupational TherapyGeyanne GeyrosagaNo ratings yet
- Frenulum ChildDocument5 pagesFrenulum ChildPutriNo ratings yet
- Occupational Therapist Aide: Passbooks Study GuideFrom EverandOccupational Therapist Aide: Passbooks Study GuideNo ratings yet
- ManDocument6 pagesManNeko NekoNo ratings yet
- CBT MOCK TEST 1-2 and Answer Key PDFDocument55 pagesCBT MOCK TEST 1-2 and Answer Key PDFNeko Neko100% (1)
- Nclex Random Fact To StudyDocument431 pagesNclex Random Fact To StudyNeko Neko100% (1)
- Health Care MGTDocument9 pagesHealth Care MGTNeko NekoNo ratings yet
- Comparison of Nursing and Medical DiagnosesDocument14 pagesComparison of Nursing and Medical DiagnosesNeko NekoNo ratings yet
- College of Engineering and Architecture: University of La Salette, IncDocument1 pageCollege of Engineering and Architecture: University of La Salette, IncNeko NekoNo ratings yet
- DiscussionDocument6 pagesDiscussionNeko NekoNo ratings yet
- DrugDocument1 pageDrugNeko NekoNo ratings yet
- Artifacts in HistopathologyDocument8 pagesArtifacts in Histopathologysyed ahmedNo ratings yet
- CANULATION2Document4 pagesCANULATION2profarmahNo ratings yet
- Modified Technique For Esthetic Crown Lengthening in The Natural Dentition - Case SeriesDocument15 pagesModified Technique For Esthetic Crown Lengthening in The Natural Dentition - Case SeriesCentro Dental IntegralNo ratings yet
- Ep TrainingDocument35 pagesEp TrainingVatsal SinghNo ratings yet
- Assessment of The AbdomenDocument93 pagesAssessment of The AbdomenAbdurehman AyeleNo ratings yet
- Dr. Shaf Keshavjee, Lung Transplant GuruDocument5 pagesDr. Shaf Keshavjee, Lung Transplant GuruDarren GluckmanNo ratings yet
- Refrat Semester 2. MREDocument10 pagesRefrat Semester 2. MREBambang AdityaNo ratings yet
- Brachial Plexus InjuryDocument39 pagesBrachial Plexus InjurymariaNo ratings yet
- Cell Injury Patho LabDocument17 pagesCell Injury Patho LabRUTUJA DILIP GADENo ratings yet
- Reti No MetriDocument4 pagesReti No MetriEstmar ValentinoNo ratings yet
- ER Nurse/Offshore Oil Rig Medic: at Dar Afia Medical Company/Seadrill/International SOS/ Rowan Drilling CompanyDocument6 pagesER Nurse/Offshore Oil Rig Medic: at Dar Afia Medical Company/Seadrill/International SOS/ Rowan Drilling CompanyVictoria GomezNo ratings yet
- Scleral-Fixated Intraocular Lens Implants-Evolution of Surgical Techniques and Future DevelopmentsDocument32 pagesScleral-Fixated Intraocular Lens Implants-Evolution of Surgical Techniques and Future DevelopmentsHariom ShuklaNo ratings yet
- Grudziak SymposiumPresentationDocument23 pagesGrudziak SymposiumPresentationرعد النميريNo ratings yet
- AraknoiditisDocument2 pagesAraknoiditissyafiqNo ratings yet
- Aortic Valve ReplacementDocument17 pagesAortic Valve Replacementm_alodat6144No ratings yet
- Inguinal Hernia Surgery OverviewDocument15 pagesInguinal Hernia Surgery OverviewWarda BajwaNo ratings yet
- Surface Anatomy: David Ebenezer Department of Anatomy Velammal Medical CollegeDocument101 pagesSurface Anatomy: David Ebenezer Department of Anatomy Velammal Medical CollegeKarishma RameshNo ratings yet
- WFA Competency LevelsDocument5 pagesWFA Competency LevelsTroy Lyons DunowNo ratings yet
- Combination Therapy ScarsDocument6 pagesCombination Therapy Scarsxj112358No ratings yet
- Angioplasty and Stenting For Peripheral Arterial Disease of The Lower LimbsDocument13 pagesAngioplasty and Stenting For Peripheral Arterial Disease of The Lower Limbsnadia shabriNo ratings yet
- Citrasate 2Document2 pagesCitrasate 2توفيق باعبادNo ratings yet
- Doppler Sonography of Both Lower Limb Venous System Deep Venous SystemDocument2 pagesDoppler Sonography of Both Lower Limb Venous System Deep Venous SystemMukesh GuptaNo ratings yet
- Extraction of Wisdom Teeth Under General Anesthesia-A StudyDocument5 pagesExtraction of Wisdom Teeth Under General Anesthesia-A StudyCiutac ŞtefanNo ratings yet
- Chemotherapy and Nursing ManagementDocument84 pagesChemotherapy and Nursing ManagementAbdallah AlasalNo ratings yet
- Head (Skull, Scalp, Hair) : Head-To-Toe Assessment (C. Eyebrows, Eyes and Eyelashes)Document15 pagesHead (Skull, Scalp, Hair) : Head-To-Toe Assessment (C. Eyebrows, Eyes and Eyelashes)anne002No ratings yet
- Bone FractureDocument6 pagesBone FractureNetz ProtomartirNo ratings yet
- Cardiovascular System AnatomyDocument54 pagesCardiovascular System AnatomyAyen LatosaNo ratings yet
- Manual For Esu V Sse2lDocument132 pagesManual For Esu V Sse2lGregorio NavarreteNo ratings yet
- Anatomy of The Scalp!Document5 pagesAnatomy of The Scalp!GE EKNo ratings yet
- Alvin B. Vibar, M.D.Document49 pagesAlvin B. Vibar, M.D.Ditas ChuNo ratings yet