Download as docx, pdf, or txt
You might also like
- Moral Reconation Therapy MRTDocument2 pagesMoral Reconation Therapy MRTapi-259241412100% (2)
- MSC Nursing QN PaperDocument9 pagesMSC Nursing QN Papersanthyakunjumon100% (1)
- Contractors Guide Seweracc16Document15 pagesContractors Guide Seweracc16Anonymous EPSHB9tXZNo ratings yet
- Rle Worksheet Nursing ProcessDocument6 pagesRle Worksheet Nursing ProcessMARVIE JOY BALUMA CABIOCNo ratings yet
- N375 Critical Thinking Activity ExampleDocument6 pagesN375 Critical Thinking Activity ExamplefaizaNo ratings yet
- Acute Otitis Media PresentationDocument76 pagesAcute Otitis Media PresentationFarah NasyitahNo ratings yet
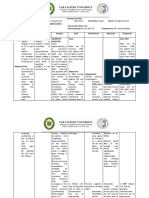
- Subjective:: Assessment Diagnosis Planning Implementation Rationale EvaluationDocument2 pagesSubjective:: Assessment Diagnosis Planning Implementation Rationale EvaluationAyra PunzalanNo ratings yet
- Acute Pain RT Surgical IncisionDocument1 pageAcute Pain RT Surgical Incisiondude06blumNo ratings yet
- Tonsilitis NCPDocument2 pagesTonsilitis NCPFATIMA MARYAMA USMANNo ratings yet
- Nursing Assessment - Pediatric Clients in The Community New 1 1Document7 pagesNursing Assessment - Pediatric Clients in The Community New 1 1Ugalde AlyssakyleNo ratings yet
- Nursing Skills Output (Nso)Document4 pagesNursing Skills Output (Nso)Julius ElciarioNo ratings yet
- HypertensionDocument3 pagesHypertensionkarl de guzmanNo ratings yet
- NCP Hip FractureDocument5 pagesNCP Hip FractureCherry Ann BalagotNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument7 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationMaria Fatima MagsinoNo ratings yet
- AnxietyDocument3 pagesAnxietyJenny Pearl Pasal50% (2)
- NCP PainDocument1 pageNCP PaindwightciderNo ratings yet
- Ineffective Coping NCPDocument4 pagesIneffective Coping NCPFrancis Alfred EscaranNo ratings yet
- Risk For Falls As Evidence by Loss of BalanceDocument4 pagesRisk For Falls As Evidence by Loss of BalanceAlexandrea MayNo ratings yet
- ماتيرنتي NcpDocument3 pagesماتيرنتي Ncpلمى الشهريNo ratings yet
- Chronic Obstructive Pulmonary Disease Bronchitis Nursing Care PlansDocument10 pagesChronic Obstructive Pulmonary Disease Bronchitis Nursing Care Planscy belNo ratings yet
- Ectopic Pregnancy NCP (Vizconde, Ehreiz Raiden C. BSN2-A)Document10 pagesEctopic Pregnancy NCP (Vizconde, Ehreiz Raiden C. BSN2-A)Raiden VizcondeNo ratings yet
- Nursing Care Plan-Hepatitis A - B (Team Lion Queen)Document9 pagesNursing Care Plan-Hepatitis A - B (Team Lion Queen)Calvo AdrianNo ratings yet
- Community Health Profile Worksheet (Worksheet C)Document10 pagesCommunity Health Profile Worksheet (Worksheet C)Jahay NielNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanCindy MariscotesNo ratings yet
- Activities of Daily Living Activities of Daily Living Refer To The Basic Skills Needed To Properly Care For Oneself and MeetDocument1 pageActivities of Daily Living Activities of Daily Living Refer To The Basic Skills Needed To Properly Care For Oneself and MeetRollon, Sherwin B.No ratings yet
- Rle Module Rle Unit Week: Bachelor of Science in Nursing: Rle NCM 105 - Psychiatric NursingDocument6 pagesRle Module Rle Unit Week: Bachelor of Science in Nursing: Rle NCM 105 - Psychiatric NursingAllisson BeckersNo ratings yet
- Nursing Care Plan DMDocument8 pagesNursing Care Plan DMnikaaraaaNo ratings yet
- Case Study NCPDocument4 pagesCase Study NCPKelly OstolNo ratings yet
- Revised NCPDocument8 pagesRevised NCPKryza Dale Bunado BaticanNo ratings yet
- Com/4-Cholecystitis - Cholelithiasis - Nursing-Care - Plans/2/ 6-OverviewDocument2 pagesCom/4-Cholecystitis - Cholelithiasis - Nursing-Care - Plans/2/ 6-OverviewCharles Belonio Dorado100% (1)
- Teaching Plan PDFDocument92 pagesTeaching Plan PDFRoxanne Jane S. Graycochea100% (1)
- Unit-Iii Gordon's Functional Health PatternsDocument3 pagesUnit-Iii Gordon's Functional Health Patternsalphabennydelta4468No ratings yet
- Health History Format BlankDocument32 pagesHealth History Format BlankRich-Anne LagarasNo ratings yet
- MAHILOM NCP Risk For FallDocument2 pagesMAHILOM NCP Risk For Fallkasandra dawn BerisoNo ratings yet
- NCPDocument2 pagesNCPczeremar chanNo ratings yet
- Nursing Care Plan: Cues Objectives Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Cues Objectives Interventions Rationale EvaluationJP2001100% (1)
- Problem List Assessment Nursing Diagnosis Planning ImplementationDocument1 pageProblem List Assessment Nursing Diagnosis Planning ImplementationJai Go100% (1)
- Health Indicators: - Batch 3Document12 pagesHealth Indicators: - Batch 3Mayank JainNo ratings yet
- NCP Acute Pain WDocument1 pageNCP Acute Pain Wmiles sbNo ratings yet
- Pedia Ward NCPDocument2 pagesPedia Ward NCPChacha AllanaNo ratings yet
- Pharma Module 2 PDFDocument38 pagesPharma Module 2 PDFSheryhan Tahir BayleNo ratings yet
- Cues Nursing Diagnosis Scientific Rationale Objectives Nursing Interventions Rationale EvaluationDocument8 pagesCues Nursing Diagnosis Scientific Rationale Objectives Nursing Interventions Rationale EvaluationMa Virginia Nathalia CreerNo ratings yet
- The Ebn A. Evidence Based Nursing For Level III General QuestionDocument7 pagesThe Ebn A. Evidence Based Nursing For Level III General QuestionAvyNo ratings yet
- Teaching Plan Deviced For Teenage Mother and NewbornDocument34 pagesTeaching Plan Deviced For Teenage Mother and NewbornYzel Vasquez AdavanNo ratings yet
- NCP in PediaDocument3 pagesNCP in Pediajoister011750% (2)
- Assess The Knowledge and Attitude On Prevention of Dengue Among The Patients AttendantsDocument6 pagesAssess The Knowledge and Attitude On Prevention of Dengue Among The Patients AttendantsIJAR JOURNALNo ratings yet
- Nursing Care Plan Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationDocument2 pagesNursing Care Plan Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationValerie FischerNo ratings yet
- Circulating Nurse ScriptDocument1 pageCirculating Nurse Scriptmaga.abigail.bsnNo ratings yet
- Goal/s: After 20 Minutes of Nurse-Client Interaction, Client Will Be Knowledgeable About Newly Diagnosed Condition (Acute Appendicitis)Document3 pagesGoal/s: After 20 Minutes of Nurse-Client Interaction, Client Will Be Knowledgeable About Newly Diagnosed Condition (Acute Appendicitis)Rhn pjtNo ratings yet
- Imbalnce Nutrition Less Than Body RequirementsDocument3 pagesImbalnce Nutrition Less Than Body RequirementselheezaNo ratings yet
- NCP NDTDocument2 pagesNCP NDTMaria Celina VillarinNo ratings yet
- HTP Ineffective BreathingDocument3 pagesHTP Ineffective BreathingShyrra Edades PinderNo ratings yet
- Smoking QuestionnaireDocument5 pagesSmoking QuestionnaireAaditya Vasnik100% (1)
- Assessment of Digestive and Gi FunctionDocument3 pagesAssessment of Digestive and Gi FunctionEmi EspinoNo ratings yet
- NursingDocument11 pagesNursingNdung'u Wa Mumbi100% (1)
- Discharge Planning Incomplete AbortionDocument2 pagesDischarge Planning Incomplete AbortionNaotaka KohinataNo ratings yet
- BSN 1 H Case Application Nursing Care PlanDocument3 pagesBSN 1 H Case Application Nursing Care PlanAntonio EscotoNo ratings yet
- Learning Feedback g2Document8 pagesLearning Feedback g2Darwin DaveNo ratings yet
- NCPDocument10 pagesNCPNefre Dayap DarrocaNo ratings yet
- NCP Acute-PainDocument4 pagesNCP Acute-PainMarie CatapiaNo ratings yet
- CHAPTER 4-Atty AliboghaDocument48 pagesCHAPTER 4-Atty AliboghaPaul EspinosaNo ratings yet
- EsophagomyotomyDocument3 pagesEsophagomyotomySamVelascoNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Heart Clinic: Alternative Learning System Related Learning ExperienceDocument8 pagesHeart Clinic: Alternative Learning System Related Learning ExperienceEdson John DemayoNo ratings yet
- PULSEDocument11 pagesPULSEHilma NadzifaNo ratings yet
- Professional Development PowerpointDocument10 pagesProfessional Development Powerpointapi-549073507No ratings yet
- Brewin, C. (2014) - Cognitive Foundations of Clinical Psychology PDFDocument229 pagesBrewin, C. (2014) - Cognitive Foundations of Clinical Psychology PDFMarcela Fernanda Guzmán SánchezNo ratings yet
- Fee Regulation in Private Schooling: The Case of GujaratDocument2 pagesFee Regulation in Private Schooling: The Case of GujaratATHENA CHOWDHURYNo ratings yet
- MCU Based Drying System For Golden Rice Grains With Temperature and Humidity ModificationDocument4 pagesMCU Based Drying System For Golden Rice Grains With Temperature and Humidity ModificationJake Lester GatchalianNo ratings yet
- Las - Mapeh QuizDocument3 pagesLas - Mapeh QuizMa. Luiggie Teresita PerezNo ratings yet
- GastroparesisDocument31 pagesGastroparesisGaby ZuritaNo ratings yet
- O Recruitment Retention of HFM Program Staff PolicyDocument10 pagesO Recruitment Retention of HFM Program Staff PolicyRick ThomaNo ratings yet
- Determination of Ascorbic Acid: Analytical Chemistry IVDocument9 pagesDetermination of Ascorbic Acid: Analytical Chemistry IVashNo ratings yet
- Occupational Safety and Health STDDocument65 pagesOccupational Safety and Health STDKirk Corales100% (4)
- Brain Sync CatalogDocument17 pagesBrain Sync CatalogknonieNo ratings yet
- University of Kathmandu InternationalDocument24 pagesUniversity of Kathmandu InternationalDr.Ukihana SamuraiNo ratings yet
- Anna Nicole Smith Drug Procurement ChartDocument4 pagesAnna Nicole Smith Drug Procurement ChartQV'sNo ratings yet
- Conduct A Hazard Analysis What Does This Mean?Document5 pagesConduct A Hazard Analysis What Does This Mean?jujuNo ratings yet
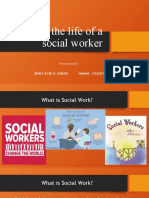
- A Day in The Life of A Social WORKER JENNY ROSE SINDONDocument13 pagesA Day in The Life of A Social WORKER JENNY ROSE SINDONma.cristina ginesNo ratings yet
- SF8 (Nutritional Status Galupo) AutomatedDocument5 pagesSF8 (Nutritional Status Galupo) AutomatedShen-Chen Cabuyao Dela PuertaNo ratings yet
- Breast Imaging Review - A Quick Guide To Essential Diagnoses (2nd Edition) PDFDocument264 pagesBreast Imaging Review - A Quick Guide To Essential Diagnoses (2nd Edition) PDFGregorio Parra100% (3)
- Gdi and GemDocument32 pagesGdi and GemDaVid Silence KawlniNo ratings yet
- Scratch AssayDocument2 pagesScratch AssayElsya Veranza100% (1)
- Philippine Association of Water Districts, Inc.: Lingkod NG Bayan Sa Buong KapuluanDocument3 pagesPhilippine Association of Water Districts, Inc.: Lingkod NG Bayan Sa Buong Kapuluanjoana marie garridoNo ratings yet
- Book Review Why Nations FailDocument11 pagesBook Review Why Nations FailCarloSangronesNo ratings yet
- Ismenore: You Should Also DoDocument2 pagesIsmenore: You Should Also DoNurul Ilmi UtamiNo ratings yet
- A Randomized, Double-Blind, Controlled Trial Comparing Rifaximin Plus Lactulose With Lactulose Alone in Treatment of Overt Hepatic EncephalopathyDocument3 pagesA Randomized, Double-Blind, Controlled Trial Comparing Rifaximin Plus Lactulose With Lactulose Alone in Treatment of Overt Hepatic EncephalopathyYunita DNo ratings yet
- PgsgaDocument2 pagesPgsgaArsela Rindang AzhariNo ratings yet
- Responsible Parenthood 2Document20 pagesResponsible Parenthood 2jessicadimailigNo ratings yet
- Solution Focused TechniquesDocument5 pagesSolution Focused TechniquesNazario Israel Narvaez ArzateNo ratings yet