Download as pdf or txt
You might also like
- Tutorial Chapter 1 - 0 ThermodynamicDocument2 pagesTutorial Chapter 1 - 0 ThermodynamicSufferedMuchNo ratings yet
- CyclophosphamideDocument7 pagesCyclophosphamideFrances Ramos33% (3)
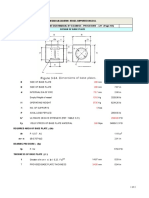
- Leg Support Calculation PDFDocument2 pagesLeg Support Calculation PDFSanjay MoreNo ratings yet
- Bronchiectasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandBronchiectasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Pleurisy, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPleurisy, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Chest Injuries: DR Rodwell Gundo Medical/Surgical Nursing DepartmentDocument47 pagesChest Injuries: DR Rodwell Gundo Medical/Surgical Nursing Departmentpaul kaundaNo ratings yet
- PneumoniaDocument12 pagesPneumoniaRola Miranda Guiang-ManaliliNo ratings yet
- Self Instructional Module On Adolescent AnemiaDocument7 pagesSelf Instructional Module On Adolescent AnemiaSagiraju SrinuNo ratings yet
- Respiratory Arrest and InsufficiencyDocument6 pagesRespiratory Arrest and InsufficiencyGetom Ngukir100% (1)
- Anju V SDocument30 pagesAnju V SJuvana LachuNo ratings yet
- PneumothoraxDocument25 pagesPneumothoraxAsma NazNo ratings yet
- Brain AbscessDocument23 pagesBrain Abscessvinnu kalyanNo ratings yet
- Lower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDocument95 pagesLower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingRI NANo ratings yet
- Respiratory Failure (Aan) PDFDocument19 pagesRespiratory Failure (Aan) PDFYudionoNo ratings yet
- Miliary TB NewDocument23 pagesMiliary TB Newzakariah kamalNo ratings yet
- Lung AbsesDocument48 pagesLung AbsesAvhindAvhindNo ratings yet
- Bronchiectasis - Ppt-Medina Presentation2Document25 pagesBronchiectasis - Ppt-Medina Presentation2chebetnaomi945No ratings yet
- Seminar Asthma PDFDocument39 pagesSeminar Asthma PDFAriff Mahdzub0% (1)
- Carpel Tunnel SyndromeDocument12 pagesCarpel Tunnel Syndromeyordin deontaNo ratings yet
- Secondary TB Eng 2015Document124 pagesSecondary TB Eng 2015humanNo ratings yet
- Neurology - : Approach To Headache DisordersDocument8 pagesNeurology - : Approach To Headache DisordersKarenNo ratings yet
- Thoracic Surgery LobectomyDocument21 pagesThoracic Surgery LobectomyJane SharpsNo ratings yet
- SepsisDocument33 pagesSepsisv_vijayakanth7656No ratings yet
- Pulmonary TBDocument13 pagesPulmonary TBAmanda ScarletNo ratings yet
- Icu PsychosisDocument23 pagesIcu PsychosisJisha JanardhanNo ratings yet
- Mitral Stenosis: Dr. Mohammed Asrafur Rahman MBBS, Bcs (H), MD Resident (Internal Medicine) (P-A) Chattogram Medical CollegeDocument16 pagesMitral Stenosis: Dr. Mohammed Asrafur Rahman MBBS, Bcs (H), MD Resident (Internal Medicine) (P-A) Chattogram Medical CollegeAsrafur RahmanNo ratings yet
- Dyspnea: Ahammed Naseem Roll No: 3 Second Year BSC Nursing Al-Mas College of NursingDocument19 pagesDyspnea: Ahammed Naseem Roll No: 3 Second Year BSC Nursing Al-Mas College of NursingNaseem Bin YoosafNo ratings yet
- Pedal EdemaDocument45 pagesPedal Edemafirdaushassan2112No ratings yet
- Pulmonary Tuberculosis: Presented By: Mis.M.K.Kaku Nursing TutorDocument16 pagesPulmonary Tuberculosis: Presented By: Mis.M.K.Kaku Nursing TutorKaku ManishaNo ratings yet
- Muscle Strength TestingDocument3 pagesMuscle Strength TestingGiselle Chloe Baluya ico100% (1)
- AppendicitisDocument36 pagesAppendicitisPetro MyronovNo ratings yet
- BurnsDocument106 pagesBurnsShahini PrajapatiNo ratings yet
- Cardiovascular System Diseases Part 1Document22 pagesCardiovascular System Diseases Part 1Prince Rener Velasco PeraNo ratings yet
- Asthma and CopdDocument44 pagesAsthma and CopdBeer Dilacshe100% (1)
- Cardiovascular SystemDocument4 pagesCardiovascular SystemMuhammad ZahidNo ratings yet
- Nephrotic and Nephritic SyndromesDocument27 pagesNephrotic and Nephritic SyndromesJoshua Smith100% (1)
- PLAGUEDocument5 pagesPLAGUEHpu JogindernagerNo ratings yet
- SR NO Time Specific Objective Content Teacher Activities Student Activities A.V Aids EvaluationDocument16 pagesSR NO Time Specific Objective Content Teacher Activities Student Activities A.V Aids EvaluationJuhi Johnson JadhavNo ratings yet
- 22 Manuscript Intestinal ObstructionDocument8 pages22 Manuscript Intestinal Obstructionkint manlangitNo ratings yet
- Isabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderDocument15 pagesIsabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderCharlz ZipaganNo ratings yet
- Heart BlockDocument20 pagesHeart BlockSumathi GopinathNo ratings yet
- Woman With PneumoniaDocument9 pagesWoman With PneumoniaNohaira SADANGNo ratings yet
- Pulmonary TuberculosisDocument6 pagesPulmonary TuberculosisZachary CohenNo ratings yet
- LEUKEMIADocument20 pagesLEUKEMIAHafsaNo ratings yet
- Renal TransplantationDocument50 pagesRenal Transplantationregie cuaresmaNo ratings yet
- Chest InjuriesDocument19 pagesChest InjuriesAbdi Kumala100% (1)
- Miconium Aspiration SyndromeDocument19 pagesMiconium Aspiration SyndromeEnna PaulaNo ratings yet
- Cough, Dyspnea and HemoptysisDocument34 pagesCough, Dyspnea and HemoptysisPooja ShashidharanNo ratings yet
- Acute Rheumatic FeverDocument50 pagesAcute Rheumatic Feversunaryo lNo ratings yet
- Diagnosis & Treament: ShockDocument52 pagesDiagnosis & Treament: ShockasepNo ratings yet
- Lung AbscessDocument25 pagesLung AbscessIskandar HasanNo ratings yet
- Pulmonary Function TestDocument57 pagesPulmonary Function TestDeepika PatelNo ratings yet
- TB SpineDocument15 pagesTB SpineChe AinNo ratings yet
- Unconsciousness: Anil PatidarDocument29 pagesUnconsciousness: Anil Patidarjinal sutharNo ratings yet
- Tuberculosis: Dr.V. Gangadharan Professor & Hod Department of Respiratory Medicine Saveetha Medical College HospitalDocument58 pagesTuberculosis: Dr.V. Gangadharan Professor & Hod Department of Respiratory Medicine Saveetha Medical College HospitalJoanna RachelNo ratings yet
- Pneumonia: DefinitionDocument5 pagesPneumonia: DefinitionhemaanandhyNo ratings yet
- 3rd Year Internal Assessment Child Health NursingDocument20 pages3rd Year Internal Assessment Child Health NursingRajesh Kumar SahNo ratings yet
- Guiilan Barre SyndromeDocument19 pagesGuiilan Barre SyndromeDhayaneeDruAinsleyIINo ratings yet
- Urinary Tract Infection (UTI)Document39 pagesUrinary Tract Infection (UTI)Sabita TripathiNo ratings yet
- Bronchial AsthmaDocument71 pagesBronchial AsthmaHero MondaresNo ratings yet
- Mechanical Ventilation: Reported By: Sembrana Ii, Gloria TRINIDAD, Anna PatriciaDocument55 pagesMechanical Ventilation: Reported By: Sembrana Ii, Gloria TRINIDAD, Anna PatriciaElaine IsalosNo ratings yet
- ASTHMADocument16 pagesASTHMAAyesigwa Gerald96100% (1)
- Restrictive Lung DiseaseDocument32 pagesRestrictive Lung DiseaseSalman Khan100% (1)
- AM1000 Modbus Protocol en VA0Document4 pagesAM1000 Modbus Protocol en VA0Pedro José Arjona GonzálezNo ratings yet
- ToR For Fiberglass Biogas Plants Installation - EOI PDFDocument4 pagesToR For Fiberglass Biogas Plants Installation - EOI PDFmy09No ratings yet
- Ultimate GuideDocument11 pagesUltimate GuideIgor SucevicNo ratings yet
- Psychoanalythic TheoryDocument1 pagePsychoanalythic TheorySilver BroochNo ratings yet
- Free Download All Aeronautical Engg Books: AERO 3-1 BOOKSDocument11 pagesFree Download All Aeronautical Engg Books: AERO 3-1 BOOKSMacen SnoodleNo ratings yet
- Water Content in SoilDocument4 pagesWater Content in SoilJohn Paul CristobalNo ratings yet
- Kore Network Device ConfigurationDocument61 pagesKore Network Device ConfigurationEllaziaNo ratings yet
- Unit I-Cloud ComputingDocument29 pagesUnit I-Cloud ComputingAR OFFICIALNo ratings yet
- T2T 32T BTC Master Manual enDocument10 pagesT2T 32T BTC Master Manual enRAMON RUIZNo ratings yet
- Problem: Determine The Total Volume of Earth To Be Excavated Up To Elevation 0Document17 pagesProblem: Determine The Total Volume of Earth To Be Excavated Up To Elevation 0gtech00100% (1)
- Make List SLTD-J-1401-L-6-00003-02Document4 pagesMake List SLTD-J-1401-L-6-00003-02tribhuvan ShankarNo ratings yet
- Transport Phenomena: τ =μ dv dyDocument2 pagesTransport Phenomena: τ =μ dv dySYED ASGHAR ALI SULTANNo ratings yet
- CD Dye RD0005Document7 pagesCD Dye RD0005Juan CarlosNo ratings yet
- Chapter 20 Practice TestDocument19 pagesChapter 20 Practice TestCorei'Ana Conrad0% (1)
- MATH 4 PPT Q3 W4 - Lesson 52 - Quadrilateral 1Document17 pagesMATH 4 PPT Q3 W4 - Lesson 52 - Quadrilateral 1Erika Mae TupagNo ratings yet
- Rakit Lampu LedDocument11 pagesRakit Lampu LedIbnusyam UtihNo ratings yet
- The Evolution of Video Streaming and Digital Content DeliveryDocument8 pagesThe Evolution of Video Streaming and Digital Content DeliveryBrookings InstitutionNo ratings yet
- 12 2f17 Vegetarian Argumentative EssayDocument7 pages12 2f17 Vegetarian Argumentative Essayapi-413258549No ratings yet
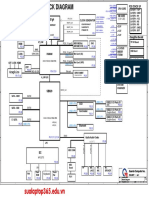
- Da0bl7mb6d0 Rev DDocument44 pagesDa0bl7mb6d0 Rev DFerreira da CunhaNo ratings yet
- Data Transformation by Andy FieldDocument1 pageData Transformation by Andy FieldGon MartNo ratings yet
- Quatre Agro Enterprise Private LimitedDocument25 pagesQuatre Agro Enterprise Private Limitedp23pallavNo ratings yet
- Tax System SriLankaDocument44 pagesTax System SriLankamandarak7146No ratings yet
- Peniel Integrated Christian Academy of Rizal, Inc. Science Weblinks GRADE 4 S.Y. 2020-2021Document3 pagesPeniel Integrated Christian Academy of Rizal, Inc. Science Weblinks GRADE 4 S.Y. 2020-2021Jhocen Grace GanironNo ratings yet
- 9 Exercise Physiology Handout 2011Document20 pages9 Exercise Physiology Handout 2011maraj687No ratings yet
- HT Billing System - May'2022Document2 pagesHT Billing System - May'2022V.Sampath RaoNo ratings yet
- Solution Manual For Fundamentals of Semiconductor Fabrication Gary S May Simon M Sze Isbn 0471232793 Isbn 978-0-471 23279 7 Isbn 9780471232797Document16 pagesSolution Manual For Fundamentals of Semiconductor Fabrication Gary S May Simon M Sze Isbn 0471232793 Isbn 978-0-471 23279 7 Isbn 9780471232797warepneumomxkhf100% (17)
- X PPT CH 12 ElectricityDocument12 pagesX PPT CH 12 ElectricityAakriti100% (1)