
Elaine M.C. Chau PDF
Elaine M.C. Chau PDF
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Rosh EbookDocument825 pagesRosh EbookLeila Nabavi100% (3)
- Grossman Baims Cardiac Catheterization Angiography and Intervention 8th Edition Ebook PDFDocument62 pagesGrossman Baims Cardiac Catheterization Angiography and Intervention 8th Edition Ebook PDFjeffrey.nevarez629100% (46)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Dysrhythmias ChartDocument6 pagesDysrhythmias Chartjkrix100% (1)
- Chinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Document11 pagesChinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Reda SoNo ratings yet
- CHAPTER 27 - Heart Failure With A Preserved Ejection FractionDocument15 pagesCHAPTER 27 - Heart Failure With A Preserved Ejection FractionReda SoNo ratings yet
- Chapter 32 - Genetic Cardiac ArrythmiasDocument7 pagesChapter 32 - Genetic Cardiac ArrythmiasReda SoNo ratings yet
- Name: - Year LevelDocument6 pagesName: - Year LevelReda SoNo ratings yet
- Private Ward Admission Census 1Document6 pagesPrivate Ward Admission Census 1Reda SoNo ratings yet
- CHAPTER 11: The History and Physical Examination: An Evidence Based ApproachDocument5 pagesCHAPTER 11: The History and Physical Examination: An Evidence Based ApproachReda SoNo ratings yet
- Ward Reflection PaperDocument1 pageWard Reflection PaperReda SoNo ratings yet
- Risk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Document7 pagesRisk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Reda SoNo ratings yet
- EXAM-MITRAL VALVE DISEASE - Reda SoDocument5 pagesEXAM-MITRAL VALVE DISEASE - Reda SoReda SoNo ratings yet
- Answer Key-Mitral ValveDocument6 pagesAnswer Key-Mitral ValveReda SoNo ratings yet
- Coronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Document3 pagesCoronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Reda SoNo ratings yet
- Rapid Response Team and Cardiac Arrest/Resuscitation TeamDocument11 pagesRapid Response Team and Cardiac Arrest/Resuscitation TeamReda SoNo ratings yet
- Tilt Table Testing: Name Age/Sex APDocument1 pageTilt Table Testing: Name Age/Sex APReda SoNo ratings yet
- 2011 PadDocument19 pages2011 PadReda SoNo ratings yet
- Tilt Table Testing: Name Age/Sex APDocument1 pageTilt Table Testing: Name Age/Sex APReda SoNo ratings yet
- Team BLDG LetterDocument1 pageTeam BLDG LetterReda SoNo ratings yet
- Vascular Conference: JUNE 2018 - MARCH 2019Document2 pagesVascular Conference: JUNE 2018 - MARCH 2019Reda SoNo ratings yet
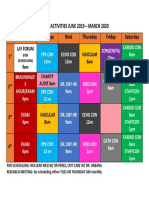
- Daily Activities 2019Document1 pageDaily Activities 2019Reda SoNo ratings yet
- ECHO CensusDocument9 pagesECHO CensusReda SoNo ratings yet
- Compu Ted Tomogra Phy: (M90Us - LiDocument1 pageCompu Ted Tomogra Phy: (M90Us - LiReda SoNo ratings yet
- Research ProtocolDocument13 pagesResearch ProtocolReda SoNo ratings yet
- Case Protocol 3Document5 pagesCase Protocol 3Reda SoNo ratings yet
- December 12Document12 pagesDecember 12Reda SoNo ratings yet
- Sept 3 2017Document7 pagesSept 3 2017Reda SoNo ratings yet
- Mckee 2012Document10 pagesMckee 2012Reda SoNo ratings yet
- 7 Overview of LipidDocument85 pages7 Overview of LipidReda SoNo ratings yet
- IungDocument8 pagesIungReda SoNo ratings yet
- Chronic Kidney DiseaseDocument16 pagesChronic Kidney DiseaseJenessel Ann P DaugNo ratings yet
- 1 SMDocument15 pages1 SMemmanuellagrace06No ratings yet
- Encyclopedia of Medical Decision MakingDocument1,266 pagesEncyclopedia of Medical Decision MakingAgam Reddy M100% (3)
- Osce - EcgDocument8 pagesOsce - EcgwNo ratings yet
- Cardio-Pulmonary Resuscitation PDFDocument21 pagesCardio-Pulmonary Resuscitation PDFMahmud DipuNo ratings yet
- Incomplete Right Bundle-Branch Block: An Electrocardiographic MisnomerDocument10 pagesIncomplete Right Bundle-Branch Block: An Electrocardiographic MisnomerxtineNo ratings yet
- Shazia Kazi ResumeDocument2 pagesShazia Kazi Resumeshazia kaziNo ratings yet
- Thu Oc Chong Loann HipDocument36 pagesThu Oc Chong Loann HipBạch MãNo ratings yet
- PacemakerDocument24 pagesPacemakerLAWKUSH KUMARNo ratings yet
- Normal Ecg, Infarction & Arrhythmia SDocument98 pagesNormal Ecg, Infarction & Arrhythmia SAdinda GupitaNo ratings yet
- Blick v. Connecticut ComplaintDocument11 pagesBlick v. Connecticut ComplaintestannardNo ratings yet
- Guidelines GUCH FTDocument43 pagesGuidelines GUCH FTmiky1320No ratings yet
- Hypoplastic Left Heart SyndromeDocument26 pagesHypoplastic Left Heart SyndromeKhaled S. HarbNo ratings yet
- Congenital Cardiac Disease: A Guide To Evaluation, Treatment and Anesthetic ManagementDocument87 pagesCongenital Cardiac Disease: A Guide To Evaluation, Treatment and Anesthetic ManagementJZNo ratings yet
- Normal Sinus RhythmDocument97 pagesNormal Sinus RhythmNatasha LiberisNo ratings yet
- ARNI in Cardiovascular, Current UpdateDocument12 pagesARNI in Cardiovascular, Current Updatefazlur risyad laochiNo ratings yet
- Normal ECGDocument41 pagesNormal ECGRoscelie KhoNo ratings yet
- Basic ECG Lecture - NewDocument148 pagesBasic ECG Lecture - NewAradhanaRamchandaniNo ratings yet
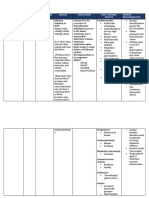
- Drug Name Brand Name Classification Dosage Indications Side/ Adverse Effects Nursing ResponsibilitiesDocument2 pagesDrug Name Brand Name Classification Dosage Indications Side/ Adverse Effects Nursing ResponsibilitiesRonald BurkeNo ratings yet
- PDF Surgery of Conotruncal Anomalies 1St Edition Francois Lacour Gayet Ebook Full ChapterDocument53 pagesPDF Surgery of Conotruncal Anomalies 1St Edition Francois Lacour Gayet Ebook Full Chapterrobert.atkinson449100% (4)
- دليل الأمراض الشائعة للأطباء-1Document148 pagesدليل الأمراض الشائعة للأطباء-1Ibrahim RamizNo ratings yet
- How To Read An ECGDocument13 pagesHow To Read An ECGNity Ganesan0% (1)
- Ecg MonitoringDocument26 pagesEcg Monitoringclaire yowsNo ratings yet
- Reading The Holter ECG ReportDocument50 pagesReading The Holter ECG ReportGreta Tanushi KukaNo ratings yet
- DYSRHYTHMIASDocument9 pagesDYSRHYTHMIASgudobenNo ratings yet
- B Modalities of RRT PDF 6542344047Document309 pagesB Modalities of RRT PDF 6542344047srihandayani1984No ratings yet
- SAB HandbookDocument81 pagesSAB HandbookDalibor CetojevicNo ratings yet































































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Rosh EbookDocument825 pagesRosh EbookLeila Nabavi100% (3)
- Grossman Baims Cardiac Catheterization Angiography and Intervention 8th Edition Ebook PDFDocument62 pagesGrossman Baims Cardiac Catheterization Angiography and Intervention 8th Edition Ebook PDFjeffrey.nevarez629100% (46)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Dysrhythmias ChartDocument6 pagesDysrhythmias Chartjkrix100% (1)
- Chinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Document11 pagesChinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Reda SoNo ratings yet
- CHAPTER 27 - Heart Failure With A Preserved Ejection FractionDocument15 pagesCHAPTER 27 - Heart Failure With A Preserved Ejection FractionReda SoNo ratings yet
- Chapter 32 - Genetic Cardiac ArrythmiasDocument7 pagesChapter 32 - Genetic Cardiac ArrythmiasReda SoNo ratings yet
- Name: - Year LevelDocument6 pagesName: - Year LevelReda SoNo ratings yet
- Private Ward Admission Census 1Document6 pagesPrivate Ward Admission Census 1Reda SoNo ratings yet
- CHAPTER 11: The History and Physical Examination: An Evidence Based ApproachDocument5 pagesCHAPTER 11: The History and Physical Examination: An Evidence Based ApproachReda SoNo ratings yet
- Ward Reflection PaperDocument1 pageWard Reflection PaperReda SoNo ratings yet
- Risk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Document7 pagesRisk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Reda SoNo ratings yet
- EXAM-MITRAL VALVE DISEASE - Reda SoDocument5 pagesEXAM-MITRAL VALVE DISEASE - Reda SoReda SoNo ratings yet
- Answer Key-Mitral ValveDocument6 pagesAnswer Key-Mitral ValveReda SoNo ratings yet
- Coronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Document3 pagesCoronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Reda SoNo ratings yet
- Rapid Response Team and Cardiac Arrest/Resuscitation TeamDocument11 pagesRapid Response Team and Cardiac Arrest/Resuscitation TeamReda SoNo ratings yet
- Tilt Table Testing: Name Age/Sex APDocument1 pageTilt Table Testing: Name Age/Sex APReda SoNo ratings yet
- 2011 PadDocument19 pages2011 PadReda SoNo ratings yet
- Tilt Table Testing: Name Age/Sex APDocument1 pageTilt Table Testing: Name Age/Sex APReda SoNo ratings yet
- Team BLDG LetterDocument1 pageTeam BLDG LetterReda SoNo ratings yet
- Vascular Conference: JUNE 2018 - MARCH 2019Document2 pagesVascular Conference: JUNE 2018 - MARCH 2019Reda SoNo ratings yet
- Daily Activities 2019Document1 pageDaily Activities 2019Reda SoNo ratings yet
- ECHO CensusDocument9 pagesECHO CensusReda SoNo ratings yet
- Compu Ted Tomogra Phy: (M90Us - LiDocument1 pageCompu Ted Tomogra Phy: (M90Us - LiReda SoNo ratings yet
- Research ProtocolDocument13 pagesResearch ProtocolReda SoNo ratings yet
- Case Protocol 3Document5 pagesCase Protocol 3Reda SoNo ratings yet
- December 12Document12 pagesDecember 12Reda SoNo ratings yet
- Sept 3 2017Document7 pagesSept 3 2017Reda SoNo ratings yet
- Mckee 2012Document10 pagesMckee 2012Reda SoNo ratings yet
- 7 Overview of LipidDocument85 pages7 Overview of LipidReda SoNo ratings yet
- IungDocument8 pagesIungReda SoNo ratings yet
- Chronic Kidney DiseaseDocument16 pagesChronic Kidney DiseaseJenessel Ann P DaugNo ratings yet
- 1 SMDocument15 pages1 SMemmanuellagrace06No ratings yet
- Encyclopedia of Medical Decision MakingDocument1,266 pagesEncyclopedia of Medical Decision MakingAgam Reddy M100% (3)
- Osce - EcgDocument8 pagesOsce - EcgwNo ratings yet
- Cardio-Pulmonary Resuscitation PDFDocument21 pagesCardio-Pulmonary Resuscitation PDFMahmud DipuNo ratings yet
- Incomplete Right Bundle-Branch Block: An Electrocardiographic MisnomerDocument10 pagesIncomplete Right Bundle-Branch Block: An Electrocardiographic MisnomerxtineNo ratings yet
- Shazia Kazi ResumeDocument2 pagesShazia Kazi Resumeshazia kaziNo ratings yet
- Thu Oc Chong Loann HipDocument36 pagesThu Oc Chong Loann HipBạch MãNo ratings yet
- PacemakerDocument24 pagesPacemakerLAWKUSH KUMARNo ratings yet
- Normal Ecg, Infarction & Arrhythmia SDocument98 pagesNormal Ecg, Infarction & Arrhythmia SAdinda GupitaNo ratings yet
- Blick v. Connecticut ComplaintDocument11 pagesBlick v. Connecticut ComplaintestannardNo ratings yet
- Guidelines GUCH FTDocument43 pagesGuidelines GUCH FTmiky1320No ratings yet
- Hypoplastic Left Heart SyndromeDocument26 pagesHypoplastic Left Heart SyndromeKhaled S. HarbNo ratings yet
- Congenital Cardiac Disease: A Guide To Evaluation, Treatment and Anesthetic ManagementDocument87 pagesCongenital Cardiac Disease: A Guide To Evaluation, Treatment and Anesthetic ManagementJZNo ratings yet
- Normal Sinus RhythmDocument97 pagesNormal Sinus RhythmNatasha LiberisNo ratings yet
- ARNI in Cardiovascular, Current UpdateDocument12 pagesARNI in Cardiovascular, Current Updatefazlur risyad laochiNo ratings yet
- Normal ECGDocument41 pagesNormal ECGRoscelie KhoNo ratings yet
- Basic ECG Lecture - NewDocument148 pagesBasic ECG Lecture - NewAradhanaRamchandaniNo ratings yet
- Drug Name Brand Name Classification Dosage Indications Side/ Adverse Effects Nursing ResponsibilitiesDocument2 pagesDrug Name Brand Name Classification Dosage Indications Side/ Adverse Effects Nursing ResponsibilitiesRonald BurkeNo ratings yet
- PDF Surgery of Conotruncal Anomalies 1St Edition Francois Lacour Gayet Ebook Full ChapterDocument53 pagesPDF Surgery of Conotruncal Anomalies 1St Edition Francois Lacour Gayet Ebook Full Chapterrobert.atkinson449100% (4)
- دليل الأمراض الشائعة للأطباء-1Document148 pagesدليل الأمراض الشائعة للأطباء-1Ibrahim RamizNo ratings yet
- How To Read An ECGDocument13 pagesHow To Read An ECGNity Ganesan0% (1)
- Ecg MonitoringDocument26 pagesEcg Monitoringclaire yowsNo ratings yet
- Reading The Holter ECG ReportDocument50 pagesReading The Holter ECG ReportGreta Tanushi KukaNo ratings yet
- DYSRHYTHMIASDocument9 pagesDYSRHYTHMIASgudobenNo ratings yet
- B Modalities of RRT PDF 6542344047Document309 pagesB Modalities of RRT PDF 6542344047srihandayani1984No ratings yet
- SAB HandbookDocument81 pagesSAB HandbookDalibor CetojevicNo ratings yet