Download as pdf or txt
You might also like
- Infectious Disease Medical Behavioral Screens AmendedDocument6 pagesInfectious Disease Medical Behavioral Screens AmendedHengkyNo ratings yet
- A Study of Brainstem Evoked Response Audiometry in Children With Severe Hearing LossDocument5 pagesA Study of Brainstem Evoked Response Audiometry in Children With Severe Hearing LossFaisal YousafNo ratings yet
- Brainstem Evoked Response Audiometry (BERA) in Neonates With HyperbillirubinemiaDocument5 pagesBrainstem Evoked Response Audiometry (BERA) in Neonates With HyperbillirubinemiabidisNo ratings yet
- Slow Auditory Evoked Potentials (1 InterligneDocument8 pagesSlow Auditory Evoked Potentials (1 Interligner.boniver524No ratings yet
- BERA As A Objective Test in Cases of Inconsistent Response For Pure Tone AudiometryDocument7 pagesBERA As A Objective Test in Cases of Inconsistent Response For Pure Tone AudiometryLUZ MARINA FIGUEROA LUNANo ratings yet
- Cochlear Implantation: Is Hearing Preservation Necessary in Severe To Profound Hearing Loss?Document3 pagesCochlear Implantation: Is Hearing Preservation Necessary in Severe To Profound Hearing Loss?Lisa MallinckrodtNo ratings yet
- Brainstem Evoked Response Audiometry in Normal Hearing SubjectsDocument6 pagesBrainstem Evoked Response Audiometry in Normal Hearing SubjectsPrateek Kumar PandaNo ratings yet
- The Role of Intratympanic Dexamethasone in Sudden Sensorineural Hearing LossDocument5 pagesThe Role of Intratympanic Dexamethasone in Sudden Sensorineural Hearing LossAditya HendraNo ratings yet
- Efficiency of Stenger Test in Confirming Profound Unilateral Pseudohypacusis PDFDocument5 pagesEfficiency of Stenger Test in Confirming Profound Unilateral Pseudohypacusis PDFValentina Muñoz OyarzúnNo ratings yet
- 9 Audiometer 03 07 2023Document30 pages9 Audiometer 03 07 2023Kushagra Narang 21BML0031No ratings yet
- Does Peripheral Auditory Threshold Correlate With Brainstem Auditory Function at Term in Preterm Infants?Document5 pagesDoes Peripheral Auditory Threshold Correlate With Brainstem Auditory Function at Term in Preterm Infants?fdsudirmanNo ratings yet
- Video Head Impulse Test and Cervical Vestibular Evoked Myogenic Potentials in Patients Withmenieres DiseaseDocument7 pagesVideo Head Impulse Test and Cervical Vestibular Evoked Myogenic Potentials in Patients Withmenieres DiseaseIJAR JOURNALNo ratings yet
- Study of The Effect of Mobile Phones On HearingDocument5 pagesStudy of The Effect of Mobile Phones On HearingPranay DasNo ratings yet
- Smartphone-Based Hearing Test As An Aid in The Initial Evaluation of Unilateral Sudden Sensorineural Hearing LossDocument8 pagesSmartphone-Based Hearing Test As An Aid in The Initial Evaluation of Unilateral Sudden Sensorineural Hearing LossAnsyah EdisonNo ratings yet
- HIPOACUSIA6Document5 pagesHIPOACUSIA6cristianNo ratings yet
- PatersonDocument6 pagesPatersonCristhian Jover CastroNo ratings yet
- Round and Oval Window Reinforcement For The Treatment of HyperacusisDocument5 pagesRound and Oval Window Reinforcement For The Treatment of HyperacusistonzmanojNo ratings yet
- Congenital Middle Ear Anomalies: Anatomical and Functional Results of SurgeryDocument6 pagesCongenital Middle Ear Anomalies: Anatomical and Functional Results of SurgeryVali MocanuNo ratings yet
- Progressive Asymmetry in Occupational Noise-Induced Hearing Loss A Large Population-Based Cohort Study With A 15-Year Follow-Up PDFDocument6 pagesProgressive Asymmetry in Occupational Noise-Induced Hearing Loss A Large Population-Based Cohort Study With A 15-Year Follow-Up PDFKaty Marlen GongoraNo ratings yet
- Bjorl: Auditory Steady State Response in Pediatric AudiologyDocument6 pagesBjorl: Auditory Steady State Response in Pediatric AudiologyNur Syamsiah MNo ratings yet
- Jurnal VertigoDocument4 pagesJurnal VertigoNur Cahyani SetiawatiNo ratings yet
- Electro-Tactile Stimulation (ETS) Enhances Cochlear-Implant Mandarin Tone RecognitionDocument5 pagesElectro-Tactile Stimulation (ETS) Enhances Cochlear-Implant Mandarin Tone RecognitionAdrian ErindraNo ratings yet
- Abr BasicDocument4 pagesAbr BasicSujeet PathakNo ratings yet
- Prevalence of Dysphonia in Children With Adenotonsillar Problems....Document7 pagesPrevalence of Dysphonia in Children With Adenotonsillar Problems....Casal AmigoNo ratings yet
- Wong2019 PDFDocument7 pagesWong2019 PDFTinha 999 chancesNo ratings yet
- Measurement of Correlation Between Dizziness Handicapped Inventory and Pure Tone Audiometry For Early Diagnosis of Menieres DiseaseDocument6 pagesMeasurement of Correlation Between Dizziness Handicapped Inventory and Pure Tone Audiometry For Early Diagnosis of Menieres DiseaseIJAR JOURNALNo ratings yet
- Outcomes of TinnitusDocument6 pagesOutcomes of TinnitusmakifkilicNo ratings yet
- Hearing Status in Neonatal Hyperbilirubinemia by Auditory Brain Stem Evoked Response and Transient Evoked Otoacoustic EmissionDocument4 pagesHearing Status in Neonatal Hyperbilirubinemia by Auditory Brain Stem Evoked Response and Transient Evoked Otoacoustic EmissionGaurav MedikeriNo ratings yet
- Incidence of Developing Contralateral M Enie're's Disease in Patients Undergoing Transmastoid Labyrinthectomy For Unilateral M Enie're's DiseaseDocument4 pagesIncidence of Developing Contralateral M Enie're's Disease in Patients Undergoing Transmastoid Labyrinthectomy For Unilateral M Enie're's DiseaseNoviTrianaNo ratings yet
- MMN Reference ValuesDocument5 pagesMMN Reference ValuesLetícia Maria Martins Vasconcelos ParreiraNo ratings yet
- To Study The Incidence of Sensorineural Hearing Loss Post Meningitis in NeonatesDocument7 pagesTo Study The Incidence of Sensorineural Hearing Loss Post Meningitis in NeonatesIJAR JOURNALNo ratings yet
- A Comparison of Two Endoscopic Posterior Cordotomy Techniques: Laser Cordotomy Vs Diathermy-Assisted CordotomyDocument5 pagesA Comparison of Two Endoscopic Posterior Cordotomy Techniques: Laser Cordotomy Vs Diathermy-Assisted CordotomyGöksel TurhalNo ratings yet
- New Born Hearing ScreeningDocument26 pagesNew Born Hearing Screeningdeadly_guyNo ratings yet
- Functional Loss After Meningitis-Evaluation of Vestibular Function in Patients With Postmeningitic Hearing LossDocument10 pagesFunctional Loss After Meningitis-Evaluation of Vestibular Function in Patients With Postmeningitic Hearing LossJuan Camilo Rubiano CuellarNo ratings yet
- Neewzealand JournalDocument5 pagesNeewzealand JournalFuji Seprinur HidayatNo ratings yet
- Estado Estavel X BeraDocument17 pagesEstado Estavel X BeraCrislaine RamosNo ratings yet
- Prediction of Permanent Hearing Loss in High-Risk Preterm Infants at Term AgeDocument7 pagesPrediction of Permanent Hearing Loss in High-Risk Preterm Infants at Term AgefdsudirmanNo ratings yet
- An Update On The New Investigations in Our ClinicDocument17 pagesAn Update On The New Investigations in Our ClinickhanasifalamNo ratings yet
- Presented by Dr. Pankaj YadavDocument20 pagesPresented by Dr. Pankaj Yadavavinash mishraNo ratings yet
- Inner Ear Malformations in Cochlear Implantation Candidates at Mother and Child Hospital of Bingerville (Cote D'ivoire)Document5 pagesInner Ear Malformations in Cochlear Implantation Candidates at Mother and Child Hospital of Bingerville (Cote D'ivoire)Phong HoàngNo ratings yet
- Jurnal IacDocument11 pagesJurnal IacAinul LuthfiNo ratings yet
- Schulman Galambos1979Document5 pagesSchulman Galambos1979Feisal MoulanaNo ratings yet
- Management of Congenital Aural AtresiaDocument22 pagesManagement of Congenital Aural AtresiamelaniNo ratings yet
- Vertigo MeniereDocument5 pagesVertigo MeniereHamba AllahNo ratings yet
- Ref 7Document6 pagesRef 7NEHA BHATINo ratings yet
- HA & BrainDocument100 pagesHA & BrainGhada WageihNo ratings yet
- Liu Et Al. (2019)Document6 pagesLiu Et Al. (2019)viniciuskiss99No ratings yet
- Vestibular Evoked Myogenic Potentials in ChildrenDocument5 pagesVestibular Evoked Myogenic Potentials in ChildrenCanto XChileNo ratings yet
- Ijcpd 10 369Document4 pagesIjcpd 10 369Dr Abhigyan ShankarNo ratings yet
- Sevil 2015Document8 pagesSevil 2015neuro a2021No ratings yet
- Comparison of Tympanometry Results For Probe Tones of 226 HZ and 1000 HZ in NewbornsDocument40 pagesComparison of Tympanometry Results For Probe Tones of 226 HZ and 1000 HZ in NewbornsEkky Rizky MaulanaNo ratings yet
- Acta Otolaryngol 2021 141 12 1055-1062Document9 pagesActa Otolaryngol 2021 141 12 1055-1062BALTAZAR OTTONELLONo ratings yet
- Cochlear Implantation Under Local Anesthesia and Conscious Sedation: An Italian ExperienceDocument6 pagesCochlear Implantation Under Local Anesthesia and Conscious Sedation: An Italian ExperiencePritam PanigrahiNo ratings yet
- Management of Children With Auditory Neuropathy SPDocument8 pagesManagement of Children With Auditory Neuropathy SPmedicalcallNo ratings yet
- Crying Abnormalities in Congenital Hypothyroidism - Preliminary Spectrographic StudyDocument6 pagesCrying Abnormalities in Congenital Hypothyroidism - Preliminary Spectrographic StudyVanessa Alejandra Quilempan VivancoNo ratings yet
- Jurding Cochlea ImplantasiDocument53 pagesJurding Cochlea ImplantasipuspitaNo ratings yet
- Ef Tek Harian 2015Document6 pagesEf Tek Harian 2015neuro a2021No ratings yet
- Admin, 029 - 1046 - Ni Made Ary Wisma Dewi - GalleyDocument5 pagesAdmin, 029 - 1046 - Ni Made Ary Wisma Dewi - GalleyDika PrasetyoNo ratings yet
- International Journal of Pediatric OtorhinolaryngologyDocument9 pagesInternational Journal of Pediatric OtorhinolaryngologyAcoet MiezarNo ratings yet
- Journal of Clinical Anesthesia: Original ContributionDocument6 pagesJournal of Clinical Anesthesia: Original ContributionzaimmuhtarNo ratings yet
- MSU-Iligan Institute of Technology: Nursing Health Assessment IDocument1 pageMSU-Iligan Institute of Technology: Nursing Health Assessment IJhon Jade PalagtiwNo ratings yet
- Agencies of The UnDocument2 pagesAgencies of The Unrishit allamNo ratings yet
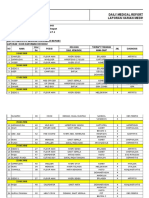
- Daily Medical Report Laporan Harian MedikDocument18 pagesDaily Medical Report Laporan Harian MedikLehman ManNo ratings yet
- TB Screening FormDocument1 pageTB Screening FormBrianKoNo ratings yet
- QUCHI L.I.-11: Pool at The CrookDocument3 pagesQUCHI L.I.-11: Pool at The Crookray72roNo ratings yet
- Shock Leadership - Pandemic ManagementDocument24 pagesShock Leadership - Pandemic Managementodin1710No ratings yet
- Infectious Disease Epidemiology Quiz 3Document1 pageInfectious Disease Epidemiology Quiz 3syifafillahNo ratings yet
- Reproductive and Child Health ProgrammeDocument2 pagesReproductive and Child Health ProgrammeAnnapurna DangetiNo ratings yet
- City of Columbus Lawsuit Against Drug CompaniesDocument123 pagesCity of Columbus Lawsuit Against Drug CompaniesAnonymous AJEonl3yxjNo ratings yet
- Bonus Task On Politics and GovernanceDocument3 pagesBonus Task On Politics and GovernanceVictorBaguilatNo ratings yet
- EpidemiologyDocument31 pagesEpidemiologyFaizan AliNo ratings yet
- PFCRT Gene in Plasmodium Falciparum Field Isolates From Muzaffargarh, PakistanDocument12 pagesPFCRT Gene in Plasmodium Falciparum Field Isolates From Muzaffargarh, PakistanvivaNo ratings yet
- A Guide To Introducing: Inactivated Polio VaccineDocument48 pagesA Guide To Introducing: Inactivated Polio VaccineJjNoznaugNo ratings yet
- Essential Biology 5.3 WORDDocument4 pagesEssential Biology 5.3 WORDCaitlin BarrettNo ratings yet
- Diosana, Jezelle B. PSY 1Y2-5Document3 pagesDiosana, Jezelle B. PSY 1Y2-5JoshuaNo ratings yet
- Medical CertificateDocument2 pagesMedical CertificatelekacaNo ratings yet
- Pyogenic Liver AbscessDocument5 pagesPyogenic Liver AbscessPatcharaporn Fern KlongklaewNo ratings yet
- Special Spot Round Process and Schedule RevisedDocument3 pagesSpecial Spot Round Process and Schedule RevisedRahul SinghNo ratings yet
- Environmental Swabbing PDFDocument10 pagesEnvironmental Swabbing PDFnilebhalNo ratings yet
- Time & Temp Paperless Office Edition 10-01-17Document67 pagesTime & Temp Paperless Office Edition 10-01-17Carlos VieiraNo ratings yet
- VertigoDocument3 pagesVertigoAacg MeryendNo ratings yet
- JCelin438 447Document10 pagesJCelin438 447MogleNo ratings yet
- What Are Chemtrails?Document7 pagesWhat Are Chemtrails?Mamello Meme BolofoNo ratings yet
- Covid 19Document9 pagesCovid 19Venus BoacNo ratings yet
- Clinical Classification of The Status of The Pulp and Dental HealthDocument15 pagesClinical Classification of The Status of The Pulp and Dental HealthrahaazadNo ratings yet
- Homeless Deaths ReportDocument102 pagesHomeless Deaths ReportCapital Public RadioNo ratings yet
- Your Friend in Singapore Has Written To You To Inform You That His Cousin in Penang Was Down With Dengue FeverDocument2 pagesYour Friend in Singapore Has Written To You To Inform You That His Cousin in Penang Was Down With Dengue FeverLee Shi HuanNo ratings yet
- LIFE SKETCH OF DR Christian Friedrich Samuel Hahnemann PDFDocument3 pagesLIFE SKETCH OF DR Christian Friedrich Samuel Hahnemann PDFkrsnaprakash8346100% (1)
- 1 s2.0 S0140673684918166 MainDocument5 pages1 s2.0 S0140673684918166 MainjimbojandersonNo ratings yet