
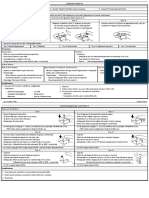
Whiplash Associated Disorders
Whiplash Associated Disorders
You might also like
- Chapter 35 Health PhysicsDocument10 pagesChapter 35 Health PhysicsMegNo ratings yet
- WhiplashDocument54 pagesWhiplashRulan AdnindyaNo ratings yet
- Flexor Tendon Repair Rehabilitation Protocols - A Systematic ReviewDocument20 pagesFlexor Tendon Repair Rehabilitation Protocols - A Systematic ReviewPatricio VásquezNo ratings yet
- Assessing Lateral Stability of The Hip and PelvisDocument7 pagesAssessing Lateral Stability of The Hip and PelvisCristian Alejandro Flores PinuerNo ratings yet
- Shark Dichotomous KeyDocument5 pagesShark Dichotomous KeyReviroda AnsayNo ratings yet
- Bad Ragaz Ring Method Gamper Lambeck Chapter 4 Comp Aq TH (2010)Document29 pagesBad Ragaz Ring Method Gamper Lambeck Chapter 4 Comp Aq TH (2010)Talia Gil Villafuerte100% (2)
- Whiplash Associated Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandWhiplash Associated Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 4 out of 5 stars4/5 (1)
- Whiplash Practice Guidelines 2003Document30 pagesWhiplash Practice Guidelines 2003silkofosNo ratings yet
- Whiplash Injury: Presenter: Dr. Md. Kamrul Islam D-Ortho Student, Department of Orthopaedic Surgery BSMMU, DhakaDocument31 pagesWhiplash Injury: Presenter: Dr. Md. Kamrul Islam D-Ortho Student, Department of Orthopaedic Surgery BSMMU, Dhakahabib757273No ratings yet
- Late Whiplash SyndromeDocument81 pagesLate Whiplash SyndromeKeith PoorbaughNo ratings yet
- Ligament Handbook 3rd EditionDocument59 pagesLigament Handbook 3rd EditionWilliam KisseNo ratings yet
- Terms: Brain Anatomy Slides Courtesy of Dr. Maria RubioDocument25 pagesTerms: Brain Anatomy Slides Courtesy of Dr. Maria RubioMatthew HylemonNo ratings yet
- Clinical Signs - NamedDocument9 pagesClinical Signs - NamedsprapurNo ratings yet
- Cervicogenic Headache Differential DiagnosisDocument10 pagesCervicogenic Headache Differential Diagnosispuchio100% (1)
- New Perspectives On Neurogenic Thoracic Outlet SyndromeDocument10 pagesNew Perspectives On Neurogenic Thoracic Outlet SyndromeMourning_WoodNo ratings yet
- Flexor Tendon Injuries SeminarDocument75 pagesFlexor Tendon Injuries SeminarAmit GoyalNo ratings yet
- Health QuestionaireDocument4 pagesHealth Questionaireapi-269450405No ratings yet
- Manual Therapy: L.A. Watson, T. Pizzari, S. BalsterDocument10 pagesManual Therapy: L.A. Watson, T. Pizzari, S. Balsterrcastello20No ratings yet
- Entrapments CadDocument3 pagesEntrapments Cadapi-467743065100% (1)
- Gluteal Tendinopathy A Review of Mechanisms, Assessmentand ManagementDocument13 pagesGluteal Tendinopathy A Review of Mechanisms, Assessmentand ManagementDaniela Villablanca100% (1)
- 2012 Scapular-Focused Treatment in Patients With ShoulderDocument13 pages2012 Scapular-Focused Treatment in Patients With ShoulderIsrael Matías Chandia Ramírez100% (1)
- The Whiplash SyndromeDocument17 pagesThe Whiplash SyndromeAbidin ZeinNo ratings yet
- The Wrist Common Injuries and ManagementDocument36 pagesThe Wrist Common Injuries and ManagementDan RollorataNo ratings yet
- Aging Spine: A Degenerative Cascade: TH STDocument4 pagesAging Spine: A Degenerative Cascade: TH STChristi EspinosaNo ratings yet
- Red Flag: MSK Services Pathway - Hip PathologyDocument16 pagesRed Flag: MSK Services Pathway - Hip PathologyMuhammed ElgasimNo ratings yet
- Extracted Pages From Cervical Spine Minimally Invasive and Open Surgery 2ED 2022Document17 pagesExtracted Pages From Cervical Spine Minimally Invasive and Open Surgery 2ED 2022Carlos Miglietti100% (1)
- Interferential Therapy Sept 08Document8 pagesInterferential Therapy Sept 08api-19753815100% (1)
- Lumbar Facet Pain ArticleDocument24 pagesLumbar Facet Pain ArticlejmccoyNo ratings yet
- Effect of Dry Needling On Lumbar Muscle Stiffness in Patients With Low Back PainDocument11 pagesEffect of Dry Needling On Lumbar Muscle Stiffness in Patients With Low Back PainValeria AlfaroNo ratings yet
- Orthosis: (Orthotic) Is A Device That Is Applied Externally To A Part ofDocument39 pagesOrthosis: (Orthotic) Is A Device That Is Applied Externally To A Part ofAbhishek KaulNo ratings yet
- O'Sullivan Posture Muscle Activity 02Document7 pagesO'Sullivan Posture Muscle Activity 02Hugo ArezNo ratings yet
- Transversus Abdominis Plane (Tap) BlockDocument6 pagesTransversus Abdominis Plane (Tap) BlockSuresh KumarNo ratings yet
- Application of AR and VR in Hand RehabilitationDocument30 pagesApplication of AR and VR in Hand RehabilitationYENY PAOLA BARBOSA CARDONANo ratings yet
- Spinal Segmental Sensitization As A Common OriginDocument8 pagesSpinal Segmental Sensitization As A Common OriginRossangel Huapaya RomeroNo ratings yet
- Lesson12 Musculoskeletal AssessmentDocument10 pagesLesson12 Musculoskeletal AssessmentDennis Nabor Muñoz, RN,RM100% (1)
- SportDocument2 pagesSportrima rizky nourliaNo ratings yet
- Neck PainDocument1 pageNeck PainHasan RahmanNo ratings yet
- Steroid Injections in Adult Patients With Joint and Soft Tissue Conditions JCG0055v3 PDFDocument18 pagesSteroid Injections in Adult Patients With Joint and Soft Tissue Conditions JCG0055v3 PDFSarath KumarNo ratings yet
- Overview of Tool and Key Points: Section A: HistoryDocument4 pagesOverview of Tool and Key Points: Section A: HistoryM Naeem ArhamNo ratings yet
- Actures of The Midfoot and ForefootDocument37 pagesActures of The Midfoot and ForefootMrHadezz LamerNo ratings yet
- Red Flag: MSK Services Pathway - Elbow PathologyDocument7 pagesRed Flag: MSK Services Pathway - Elbow PathologyMuhammed ElgasimNo ratings yet
- Erbs PalsyDocument9 pagesErbs PalsyVatsalVermaNo ratings yet
- Pathology and Management of Low Back PainDocument33 pagesPathology and Management of Low Back PainSam100% (1)
- Marshall 2015Document13 pagesMarshall 2015MalikinNadalNo ratings yet
- Spinal Disc HerniationDocument5 pagesSpinal Disc HerniationJoshua Hong100% (1)
- Low Back PainDocument8 pagesLow Back PainLev KalikaNo ratings yet
- Lateral and Medial EpicondylitisDocument40 pagesLateral and Medial EpicondylitisVijay PradeepNo ratings yet
- Effect of Positional Release Technique in Subjects With Subacute TrapezitisDocument9 pagesEffect of Positional Release Technique in Subjects With Subacute TrapezitisijphyNo ratings yet
- The Formula For Aerobic FitnessDocument1 pageThe Formula For Aerobic FitnessMelanie Saldivar CapalunganNo ratings yet
- Low BackDocument7 pagesLow BackMuhammad FahmyNo ratings yet
- CPG - Whiplash Associated DisordersDocument74 pagesCPG - Whiplash Associated DisordersGumDropNo ratings yet
- Shoulder Knee WristDocument110 pagesShoulder Knee Wriststevebravo81100% (1)
- Hip Joint: 5 December 2016 Anatomy Lecture By: DR Anita RaniDocument38 pagesHip Joint: 5 December 2016 Anatomy Lecture By: DR Anita RaniDr'Dinesh MishraNo ratings yet
- Genu Recurvatum SyndromDocument7 pagesGenu Recurvatum SyndromRoxana RascaNo ratings yet
- 5 6163473997578109319 PDFDocument69 pages5 6163473997578109319 PDFGhilang MauludNo ratings yet
- Dr. A. Samy TAG Upper Limb - 1Document20 pagesDr. A. Samy TAG Upper Limb - 1DRAHMEDFAHMYORTHOCLINICNo ratings yet
- Adult Physiatric History and ExaminationDocument11 pagesAdult Physiatric History and Examinationsylschebe22gmailNo ratings yet
- The Effect of Therapeutic Ultrasound On Metallic Implants - A Study in RatsDocument5 pagesThe Effect of Therapeutic Ultrasound On Metallic Implants - A Study in RatsnatkwqNo ratings yet
- Basic KinesiologyDocument6 pagesBasic KinesiologyCarmela Beatriz SuelanNo ratings yet
- Staged Approach For Rehabilitation ClassificationDocument10 pagesStaged Approach For Rehabilitation ClassificationCambriaChicoNo ratings yet
- Red Flag: MSK Services Pathway - Hand PathologyDocument10 pagesRed Flag: MSK Services Pathway - Hand PathologyMuhammed ElgasimNo ratings yet
- Ulnar Nerve: Submitted To: Dr. Gurpreet Kaur. Submitted By: Manmeet Kaur BPT-7th Sem 16204124Document33 pagesUlnar Nerve: Submitted To: Dr. Gurpreet Kaur. Submitted By: Manmeet Kaur BPT-7th Sem 16204124Jagraj singhNo ratings yet
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Multidisciplinary Cardiac RehabilitationDocument6 pagesMultidisciplinary Cardiac RehabilitationpuchioNo ratings yet
- Thoracolumbar FracturesDocument1 pageThoracolumbar FracturespuchioNo ratings yet
- Burst FractureDocument4 pagesBurst FracturepuchioNo ratings yet
- Sacral FracturesDocument4 pagesSacral FracturespuchioNo ratings yet
- Compression FractureDocument4 pagesCompression FracturepuchioNo ratings yet
- Compression FractureDocument4 pagesCompression FracturepuchioNo ratings yet
- Thoracolumbar Fracture DislocationDocument2 pagesThoracolumbar Fracture DislocationpuchioNo ratings yet
- Spinous Process and Transverse Process FracturesDocument3 pagesSpinous Process and Transverse Process FracturespuchioNo ratings yet
- Dens FractureDocument4 pagesDens FracturepuchioNo ratings yet
- Gunshot Wound: What It IsDocument2 pagesGunshot Wound: What It IspuchioNo ratings yet
- Cauda Equina SyndromeDocument3 pagesCauda Equina SyndromepuchioNo ratings yet
- Neuroimaging of The BrainDocument20 pagesNeuroimaging of The BrainpuchioNo ratings yet
- High-Pressure Injection InjuryDocument3 pagesHigh-Pressure Injection InjurypuchioNo ratings yet
- Traumatic ArthrotomyDocument2 pagesTraumatic ArthrotomypuchioNo ratings yet
- Classification of Cerebral PalsyDocument19 pagesClassification of Cerebral PalsypuchioNo ratings yet
- Musculoskeletal Growth and Development: Steven E. KoopDocument10 pagesMusculoskeletal Growth and Development: Steven E. KooppuchioNo ratings yet
- Classification of Cerebral PalsyDocument19 pagesClassification of Cerebral PalsypuchioNo ratings yet
- Elbow Dislocation Acute and ChronicDocument16 pagesElbow Dislocation Acute and ChronicpuchioNo ratings yet
- Posterolateral Rotatory Instability of The ElbowDocument14 pagesPosterolateral Rotatory Instability of The ElbowpuchioNo ratings yet
- Physical Examination of The ElbowDocument9 pagesPhysical Examination of The ElbowpuchioNo ratings yet
- Physical Examination of The ElbowDocument9 pagesPhysical Examination of The ElbowpuchioNo ratings yet
- Skin Aging Fitz 9Document13 pagesSkin Aging Fitz 9Jhauharina RfNo ratings yet
- Laju Respirasi Hewan With Cover Page v2Document8 pagesLaju Respirasi Hewan With Cover Page v2Rhian AlfiansyahNo ratings yet
- MLS3174 Clinical Haematology FEB 18 PDFDocument9 pagesMLS3174 Clinical Haematology FEB 18 PDFVisaNathanNo ratings yet
- RojiMolu - Effect of Growing Media On Seed Germination and Seedling Growth of Porang (Amorphophallus Muelleri Blume)Document10 pagesRojiMolu - Effect of Growing Media On Seed Germination and Seedling Growth of Porang (Amorphophallus Muelleri Blume)Hari HartantoNo ratings yet
- Types of Leukocytes and The PlateletsDocument25 pagesTypes of Leukocytes and The PlateletscarcuevajailamarieNo ratings yet
- Rafaiqa-17Mar2023-Health Che PDFDocument8 pagesRafaiqa-17Mar2023-Health Che PDFmr copy xeroxNo ratings yet
- Chanchal SirDocument38 pagesChanchal SirTouhid HossainNo ratings yet
- Understanding Nutrition 13th Edition Whitney Test Bank DownloadDocument18 pagesUnderstanding Nutrition 13th Edition Whitney Test Bank DownloadMichael Lozano100% (19)
- Histogenesis of Salivary Gland NeoplasmsDocument18 pagesHistogenesis of Salivary Gland Neoplasmsporkodi sudhaNo ratings yet
- Parameterization of The AquaCrop Model For Cowpea and Assessing The Impact of Sowing Dates Normally Used On YieldDocument14 pagesParameterization of The AquaCrop Model For Cowpea and Assessing The Impact of Sowing Dates Normally Used On YieldVandeilson Belfort MouraNo ratings yet
- Model Project Proposal (ITTO)Document22 pagesModel Project Proposal (ITTO)Bhaskar PaulNo ratings yet
- Short Takes On Three Books - American ScientistDocument6 pagesShort Takes On Three Books - American ScientistRay MondoNo ratings yet
- Lecture2 GranulopoiesisDocument9 pagesLecture2 GranulopoiesisAfifa Prima GittaNo ratings yet
- Introduction To Medical Mycology: by Prof Ashraf MOGAHEDDocument61 pagesIntroduction To Medical Mycology: by Prof Ashraf MOGAHEDlianazulak100% (2)
- Zoology Sem-III & IV (New) 2019Document30 pagesZoology Sem-III & IV (New) 2019Ajay MeghanathiNo ratings yet
- Introduction To The Study of BiochemistryDocument3 pagesIntroduction To The Study of BiochemistryMIA, Joy Beatrice R.No ratings yet
- Grafting Eggplant Techniques PDFDocument6 pagesGrafting Eggplant Techniques PDFAjaya Kumar PaniNo ratings yet
- Detection of AdulterationDocument21 pagesDetection of AdulterationDR.U.Srinivasa0% (1)
- نباتاتDocument2 pagesنباتاتhaneen refaeeNo ratings yet
- Natural Regeneration: Don Minore Robert J. LaackeDocument26 pagesNatural Regeneration: Don Minore Robert J. LaackeAngela Marie AlducenteNo ratings yet
- BIOL 351 Lab Report IDocument2 pagesBIOL 351 Lab Report IshadowlightfoxNo ratings yet
- Caplan Deron 201808 PHD CannabisDocument158 pagesCaplan Deron 201808 PHD CannabisMihai SimionNo ratings yet
- Life Process - Biology MCQDocument3 pagesLife Process - Biology MCQJASMINE VIDHYANo ratings yet
- Patogenesis Preeklampsia - Apakah Masih Merupakan Penyakit Teori PDFDocument49 pagesPatogenesis Preeklampsia - Apakah Masih Merupakan Penyakit Teori PDFFellita Ratri ANo ratings yet
- Advances in Prostaglandin, Leukotriene, and Other Bioactive Lipid ResearchDocument243 pagesAdvances in Prostaglandin, Leukotriene, and Other Bioactive Lipid ResearchCarmen PopaNo ratings yet
- Epigenetic Age Clock Test Sample ReportDocument78 pagesEpigenetic Age Clock Test Sample ReportHIMMAT SINGHNo ratings yet
- Nanotechnology Optical Tweezers ReportDocument13 pagesNanotechnology Optical Tweezers ReportDaria RomanNo ratings yet









































































































Download as pdf or txt
You might also like
- Chapter 35 Health PhysicsDocument10 pagesChapter 35 Health PhysicsMegNo ratings yet
- WhiplashDocument54 pagesWhiplashRulan AdnindyaNo ratings yet
- Flexor Tendon Repair Rehabilitation Protocols - A Systematic ReviewDocument20 pagesFlexor Tendon Repair Rehabilitation Protocols - A Systematic ReviewPatricio VásquezNo ratings yet
- Assessing Lateral Stability of The Hip and PelvisDocument7 pagesAssessing Lateral Stability of The Hip and PelvisCristian Alejandro Flores PinuerNo ratings yet
- Shark Dichotomous KeyDocument5 pagesShark Dichotomous KeyReviroda AnsayNo ratings yet
- Bad Ragaz Ring Method Gamper Lambeck Chapter 4 Comp Aq TH (2010)Document29 pagesBad Ragaz Ring Method Gamper Lambeck Chapter 4 Comp Aq TH (2010)Talia Gil Villafuerte100% (2)
- Whiplash Associated Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandWhiplash Associated Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 4 out of 5 stars4/5 (1)
- Whiplash Practice Guidelines 2003Document30 pagesWhiplash Practice Guidelines 2003silkofosNo ratings yet
- Whiplash Injury: Presenter: Dr. Md. Kamrul Islam D-Ortho Student, Department of Orthopaedic Surgery BSMMU, DhakaDocument31 pagesWhiplash Injury: Presenter: Dr. Md. Kamrul Islam D-Ortho Student, Department of Orthopaedic Surgery BSMMU, Dhakahabib757273No ratings yet
- Late Whiplash SyndromeDocument81 pagesLate Whiplash SyndromeKeith PoorbaughNo ratings yet
- Ligament Handbook 3rd EditionDocument59 pagesLigament Handbook 3rd EditionWilliam KisseNo ratings yet
- Terms: Brain Anatomy Slides Courtesy of Dr. Maria RubioDocument25 pagesTerms: Brain Anatomy Slides Courtesy of Dr. Maria RubioMatthew HylemonNo ratings yet
- Clinical Signs - NamedDocument9 pagesClinical Signs - NamedsprapurNo ratings yet
- Cervicogenic Headache Differential DiagnosisDocument10 pagesCervicogenic Headache Differential Diagnosispuchio100% (1)
- New Perspectives On Neurogenic Thoracic Outlet SyndromeDocument10 pagesNew Perspectives On Neurogenic Thoracic Outlet SyndromeMourning_WoodNo ratings yet
- Flexor Tendon Injuries SeminarDocument75 pagesFlexor Tendon Injuries SeminarAmit GoyalNo ratings yet
- Health QuestionaireDocument4 pagesHealth Questionaireapi-269450405No ratings yet
- Manual Therapy: L.A. Watson, T. Pizzari, S. BalsterDocument10 pagesManual Therapy: L.A. Watson, T. Pizzari, S. Balsterrcastello20No ratings yet
- Entrapments CadDocument3 pagesEntrapments Cadapi-467743065100% (1)
- Gluteal Tendinopathy A Review of Mechanisms, Assessmentand ManagementDocument13 pagesGluteal Tendinopathy A Review of Mechanisms, Assessmentand ManagementDaniela Villablanca100% (1)
- 2012 Scapular-Focused Treatment in Patients With ShoulderDocument13 pages2012 Scapular-Focused Treatment in Patients With ShoulderIsrael Matías Chandia Ramírez100% (1)
- The Whiplash SyndromeDocument17 pagesThe Whiplash SyndromeAbidin ZeinNo ratings yet
- The Wrist Common Injuries and ManagementDocument36 pagesThe Wrist Common Injuries and ManagementDan RollorataNo ratings yet
- Aging Spine: A Degenerative Cascade: TH STDocument4 pagesAging Spine: A Degenerative Cascade: TH STChristi EspinosaNo ratings yet
- Red Flag: MSK Services Pathway - Hip PathologyDocument16 pagesRed Flag: MSK Services Pathway - Hip PathologyMuhammed ElgasimNo ratings yet
- Extracted Pages From Cervical Spine Minimally Invasive and Open Surgery 2ED 2022Document17 pagesExtracted Pages From Cervical Spine Minimally Invasive and Open Surgery 2ED 2022Carlos Miglietti100% (1)
- Interferential Therapy Sept 08Document8 pagesInterferential Therapy Sept 08api-19753815100% (1)
- Lumbar Facet Pain ArticleDocument24 pagesLumbar Facet Pain ArticlejmccoyNo ratings yet
- Effect of Dry Needling On Lumbar Muscle Stiffness in Patients With Low Back PainDocument11 pagesEffect of Dry Needling On Lumbar Muscle Stiffness in Patients With Low Back PainValeria AlfaroNo ratings yet
- Orthosis: (Orthotic) Is A Device That Is Applied Externally To A Part ofDocument39 pagesOrthosis: (Orthotic) Is A Device That Is Applied Externally To A Part ofAbhishek KaulNo ratings yet
- O'Sullivan Posture Muscle Activity 02Document7 pagesO'Sullivan Posture Muscle Activity 02Hugo ArezNo ratings yet
- Transversus Abdominis Plane (Tap) BlockDocument6 pagesTransversus Abdominis Plane (Tap) BlockSuresh KumarNo ratings yet
- Application of AR and VR in Hand RehabilitationDocument30 pagesApplication of AR and VR in Hand RehabilitationYENY PAOLA BARBOSA CARDONANo ratings yet
- Spinal Segmental Sensitization As A Common OriginDocument8 pagesSpinal Segmental Sensitization As A Common OriginRossangel Huapaya RomeroNo ratings yet
- Lesson12 Musculoskeletal AssessmentDocument10 pagesLesson12 Musculoskeletal AssessmentDennis Nabor Muñoz, RN,RM100% (1)
- SportDocument2 pagesSportrima rizky nourliaNo ratings yet
- Neck PainDocument1 pageNeck PainHasan RahmanNo ratings yet
- Steroid Injections in Adult Patients With Joint and Soft Tissue Conditions JCG0055v3 PDFDocument18 pagesSteroid Injections in Adult Patients With Joint and Soft Tissue Conditions JCG0055v3 PDFSarath KumarNo ratings yet
- Overview of Tool and Key Points: Section A: HistoryDocument4 pagesOverview of Tool and Key Points: Section A: HistoryM Naeem ArhamNo ratings yet
- Actures of The Midfoot and ForefootDocument37 pagesActures of The Midfoot and ForefootMrHadezz LamerNo ratings yet
- Red Flag: MSK Services Pathway - Elbow PathologyDocument7 pagesRed Flag: MSK Services Pathway - Elbow PathologyMuhammed ElgasimNo ratings yet
- Erbs PalsyDocument9 pagesErbs PalsyVatsalVermaNo ratings yet
- Pathology and Management of Low Back PainDocument33 pagesPathology and Management of Low Back PainSam100% (1)
- Marshall 2015Document13 pagesMarshall 2015MalikinNadalNo ratings yet
- Spinal Disc HerniationDocument5 pagesSpinal Disc HerniationJoshua Hong100% (1)
- Low Back PainDocument8 pagesLow Back PainLev KalikaNo ratings yet
- Lateral and Medial EpicondylitisDocument40 pagesLateral and Medial EpicondylitisVijay PradeepNo ratings yet
- Effect of Positional Release Technique in Subjects With Subacute TrapezitisDocument9 pagesEffect of Positional Release Technique in Subjects With Subacute TrapezitisijphyNo ratings yet
- The Formula For Aerobic FitnessDocument1 pageThe Formula For Aerobic FitnessMelanie Saldivar CapalunganNo ratings yet
- Low BackDocument7 pagesLow BackMuhammad FahmyNo ratings yet
- CPG - Whiplash Associated DisordersDocument74 pagesCPG - Whiplash Associated DisordersGumDropNo ratings yet
- Shoulder Knee WristDocument110 pagesShoulder Knee Wriststevebravo81100% (1)
- Hip Joint: 5 December 2016 Anatomy Lecture By: DR Anita RaniDocument38 pagesHip Joint: 5 December 2016 Anatomy Lecture By: DR Anita RaniDr'Dinesh MishraNo ratings yet
- Genu Recurvatum SyndromDocument7 pagesGenu Recurvatum SyndromRoxana RascaNo ratings yet
- 5 6163473997578109319 PDFDocument69 pages5 6163473997578109319 PDFGhilang MauludNo ratings yet
- Dr. A. Samy TAG Upper Limb - 1Document20 pagesDr. A. Samy TAG Upper Limb - 1DRAHMEDFAHMYORTHOCLINICNo ratings yet
- Adult Physiatric History and ExaminationDocument11 pagesAdult Physiatric History and Examinationsylschebe22gmailNo ratings yet
- The Effect of Therapeutic Ultrasound On Metallic Implants - A Study in RatsDocument5 pagesThe Effect of Therapeutic Ultrasound On Metallic Implants - A Study in RatsnatkwqNo ratings yet
- Basic KinesiologyDocument6 pagesBasic KinesiologyCarmela Beatriz SuelanNo ratings yet
- Staged Approach For Rehabilitation ClassificationDocument10 pagesStaged Approach For Rehabilitation ClassificationCambriaChicoNo ratings yet
- Red Flag: MSK Services Pathway - Hand PathologyDocument10 pagesRed Flag: MSK Services Pathway - Hand PathologyMuhammed ElgasimNo ratings yet
- Ulnar Nerve: Submitted To: Dr. Gurpreet Kaur. Submitted By: Manmeet Kaur BPT-7th Sem 16204124Document33 pagesUlnar Nerve: Submitted To: Dr. Gurpreet Kaur. Submitted By: Manmeet Kaur BPT-7th Sem 16204124Jagraj singhNo ratings yet
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Multidisciplinary Cardiac RehabilitationDocument6 pagesMultidisciplinary Cardiac RehabilitationpuchioNo ratings yet
- Thoracolumbar FracturesDocument1 pageThoracolumbar FracturespuchioNo ratings yet
- Burst FractureDocument4 pagesBurst FracturepuchioNo ratings yet
- Sacral FracturesDocument4 pagesSacral FracturespuchioNo ratings yet
- Compression FractureDocument4 pagesCompression FracturepuchioNo ratings yet
- Compression FractureDocument4 pagesCompression FracturepuchioNo ratings yet
- Thoracolumbar Fracture DislocationDocument2 pagesThoracolumbar Fracture DislocationpuchioNo ratings yet
- Spinous Process and Transverse Process FracturesDocument3 pagesSpinous Process and Transverse Process FracturespuchioNo ratings yet
- Dens FractureDocument4 pagesDens FracturepuchioNo ratings yet
- Gunshot Wound: What It IsDocument2 pagesGunshot Wound: What It IspuchioNo ratings yet
- Cauda Equina SyndromeDocument3 pagesCauda Equina SyndromepuchioNo ratings yet
- Neuroimaging of The BrainDocument20 pagesNeuroimaging of The BrainpuchioNo ratings yet
- High-Pressure Injection InjuryDocument3 pagesHigh-Pressure Injection InjurypuchioNo ratings yet
- Traumatic ArthrotomyDocument2 pagesTraumatic ArthrotomypuchioNo ratings yet
- Classification of Cerebral PalsyDocument19 pagesClassification of Cerebral PalsypuchioNo ratings yet
- Musculoskeletal Growth and Development: Steven E. KoopDocument10 pagesMusculoskeletal Growth and Development: Steven E. KooppuchioNo ratings yet
- Classification of Cerebral PalsyDocument19 pagesClassification of Cerebral PalsypuchioNo ratings yet
- Elbow Dislocation Acute and ChronicDocument16 pagesElbow Dislocation Acute and ChronicpuchioNo ratings yet
- Posterolateral Rotatory Instability of The ElbowDocument14 pagesPosterolateral Rotatory Instability of The ElbowpuchioNo ratings yet
- Physical Examination of The ElbowDocument9 pagesPhysical Examination of The ElbowpuchioNo ratings yet
- Physical Examination of The ElbowDocument9 pagesPhysical Examination of The ElbowpuchioNo ratings yet
- Skin Aging Fitz 9Document13 pagesSkin Aging Fitz 9Jhauharina RfNo ratings yet
- Laju Respirasi Hewan With Cover Page v2Document8 pagesLaju Respirasi Hewan With Cover Page v2Rhian AlfiansyahNo ratings yet
- MLS3174 Clinical Haematology FEB 18 PDFDocument9 pagesMLS3174 Clinical Haematology FEB 18 PDFVisaNathanNo ratings yet
- RojiMolu - Effect of Growing Media On Seed Germination and Seedling Growth of Porang (Amorphophallus Muelleri Blume)Document10 pagesRojiMolu - Effect of Growing Media On Seed Germination and Seedling Growth of Porang (Amorphophallus Muelleri Blume)Hari HartantoNo ratings yet
- Types of Leukocytes and The PlateletsDocument25 pagesTypes of Leukocytes and The PlateletscarcuevajailamarieNo ratings yet
- Rafaiqa-17Mar2023-Health Che PDFDocument8 pagesRafaiqa-17Mar2023-Health Che PDFmr copy xeroxNo ratings yet
- Chanchal SirDocument38 pagesChanchal SirTouhid HossainNo ratings yet
- Understanding Nutrition 13th Edition Whitney Test Bank DownloadDocument18 pagesUnderstanding Nutrition 13th Edition Whitney Test Bank DownloadMichael Lozano100% (19)
- Histogenesis of Salivary Gland NeoplasmsDocument18 pagesHistogenesis of Salivary Gland Neoplasmsporkodi sudhaNo ratings yet
- Parameterization of The AquaCrop Model For Cowpea and Assessing The Impact of Sowing Dates Normally Used On YieldDocument14 pagesParameterization of The AquaCrop Model For Cowpea and Assessing The Impact of Sowing Dates Normally Used On YieldVandeilson Belfort MouraNo ratings yet
- Model Project Proposal (ITTO)Document22 pagesModel Project Proposal (ITTO)Bhaskar PaulNo ratings yet
- Short Takes On Three Books - American ScientistDocument6 pagesShort Takes On Three Books - American ScientistRay MondoNo ratings yet
- Lecture2 GranulopoiesisDocument9 pagesLecture2 GranulopoiesisAfifa Prima GittaNo ratings yet
- Introduction To Medical Mycology: by Prof Ashraf MOGAHEDDocument61 pagesIntroduction To Medical Mycology: by Prof Ashraf MOGAHEDlianazulak100% (2)
- Zoology Sem-III & IV (New) 2019Document30 pagesZoology Sem-III & IV (New) 2019Ajay MeghanathiNo ratings yet
- Introduction To The Study of BiochemistryDocument3 pagesIntroduction To The Study of BiochemistryMIA, Joy Beatrice R.No ratings yet
- Grafting Eggplant Techniques PDFDocument6 pagesGrafting Eggplant Techniques PDFAjaya Kumar PaniNo ratings yet
- Detection of AdulterationDocument21 pagesDetection of AdulterationDR.U.Srinivasa0% (1)
- نباتاتDocument2 pagesنباتاتhaneen refaeeNo ratings yet
- Natural Regeneration: Don Minore Robert J. LaackeDocument26 pagesNatural Regeneration: Don Minore Robert J. LaackeAngela Marie AlducenteNo ratings yet
- BIOL 351 Lab Report IDocument2 pagesBIOL 351 Lab Report IshadowlightfoxNo ratings yet
- Caplan Deron 201808 PHD CannabisDocument158 pagesCaplan Deron 201808 PHD CannabisMihai SimionNo ratings yet
- Life Process - Biology MCQDocument3 pagesLife Process - Biology MCQJASMINE VIDHYANo ratings yet
- Patogenesis Preeklampsia - Apakah Masih Merupakan Penyakit Teori PDFDocument49 pagesPatogenesis Preeklampsia - Apakah Masih Merupakan Penyakit Teori PDFFellita Ratri ANo ratings yet
- Advances in Prostaglandin, Leukotriene, and Other Bioactive Lipid ResearchDocument243 pagesAdvances in Prostaglandin, Leukotriene, and Other Bioactive Lipid ResearchCarmen PopaNo ratings yet
- Epigenetic Age Clock Test Sample ReportDocument78 pagesEpigenetic Age Clock Test Sample ReportHIMMAT SINGHNo ratings yet
- Nanotechnology Optical Tweezers ReportDocument13 pagesNanotechnology Optical Tweezers ReportDaria RomanNo ratings yet