
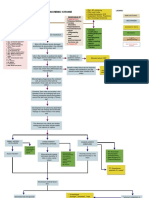
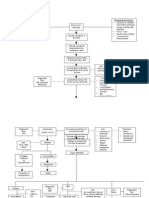
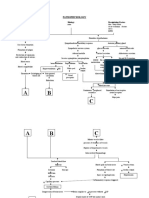
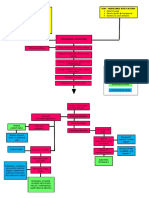
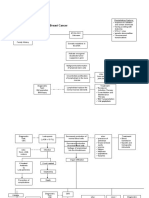
Pa Tho Physiology of Sepsis Secondary To Typhoid Ileus
Pa Tho Physiology of Sepsis Secondary To Typhoid Ileus
You might also like
- Coronary Artery Disease PathophysiologyDocument3 pagesCoronary Artery Disease Pathophysiologynursing concept maps40% (5)
- Acute Ischemic Stroke Concept MapDocument6 pagesAcute Ischemic Stroke Concept MapMoonyeen Jann Casera Balic100% (2)
- Acute Lymphoblastic Leukemia Pathophysiology: Precipitating Factors: Etiology: Predisposing FactorsDocument3 pagesAcute Lymphoblastic Leukemia Pathophysiology: Precipitating Factors: Etiology: Predisposing FactorsromelynNo ratings yet
- Pathophysiology of ALL (Diagram)Document3 pagesPathophysiology of ALL (Diagram)Joann100% (77)
- Nstemi PathoDocument2 pagesNstemi PathoSheana TmplNo ratings yet
- Congestive Heart Failure Pathophysiology Schematic DiagramDocument3 pagesCongestive Heart Failure Pathophysiology Schematic DiagramJasleen KaurNo ratings yet
- 72-HR ChickDocument16 pages72-HR Chick411452123100% (1)
- Pathophysiology of MI, COPD and BPHDocument10 pagesPathophysiology of MI, COPD and BPHSarah Lim100% (1)
- Pathophysiology of Hypertensive Cardiovascular Disease PDFDocument3 pagesPathophysiology of Hypertensive Cardiovascular Disease PDFAbdelrahman GalalNo ratings yet
- Pathophysiology of Cerebrovascular AccidentDocument3 pagesPathophysiology of Cerebrovascular AccidentByron Paz Te100% (1)
- Pathophysiology of cholangiocarcinomaJAYCERDocument3 pagesPathophysiology of cholangiocarcinomaJAYCERirish_estrellaNo ratings yet
- Pathophysiology of HypovolemiaDocument1 pagePathophysiology of HypovolemiaSheana TmplNo ratings yet
- Pathophysio of HCDDocument3 pagesPathophysio of HCDhoney requermeNo ratings yet
- O SHOCKDocument2 pagesO SHOCKkhurvy999No ratings yet
- Predisposing Factors: Precipitating Factors:: KidneysDocument1 pagePredisposing Factors: Precipitating Factors:: KidneysChe CacatianNo ratings yet
- Acute Coronary Syndrome PathophysiologyDocument3 pagesAcute Coronary Syndrome PathophysiologyJocelle Joy OrellanedaNo ratings yet
- Pathophysiolgoy Coronary Artery DiseaseDocument3 pagesPathophysiolgoy Coronary Artery DiseaseNursesLabs.comNo ratings yet
- Shanz - Clinpath Le1Document7 pagesShanz - Clinpath Le1Petrina XuNo ratings yet
- Shock and Multi OrganDocument90 pagesShock and Multi OrganElishaNo ratings yet
- NCM 106 Module 2 Lesson 1.1Document3 pagesNCM 106 Module 2 Lesson 1.1Joselyn M. LachicaNo ratings yet
- Whatsapp: +1 (402) 235-1397Document312 pagesWhatsapp: +1 (402) 235-1397Khushi RNo ratings yet
- Pa Tho PhysiologyDocument2 pagesPa Tho Physiologydavica0413No ratings yet
- Pa Tho Physiology of Cva... by Mizzy BaylonDocument3 pagesPa Tho Physiology of Cva... by Mizzy BaylonmizzybaylonNo ratings yet
- Pathophysiology: Predisposing Factors Precipitating FactorsDocument3 pagesPathophysiology: Predisposing Factors Precipitating FactorsFc ßobby HechanovaNo ratings yet
- Clinicopharmacological ConferenceDocument7 pagesClinicopharmacological ConferenceNestley TiongsonNo ratings yet
- Pre Eclampsia of Severe FeaturesDocument3 pagesPre Eclampsia of Severe FeaturesPrincess Diane S. VillegasNo ratings yet
- Pathophysiology of Acute Renal FailureDocument2 pagesPathophysiology of Acute Renal Failureminangsung minangnengNo ratings yet
- Pathophysiology of AllDocument1 pagePathophysiology of AllBGHMC PEDIAHONo ratings yet
- Pathophysio - Stemi - FinalDocument4 pagesPathophysio - Stemi - FinalPrincessDianneNo ratings yet
- Precipitating Factors:: Myocardial Cell Death (NecrosisDocument2 pagesPrecipitating Factors:: Myocardial Cell Death (NecrosisLean Ashly MacarubboNo ratings yet
- PATHOPHYDocument3 pagesPATHOPHYArlly Faena AbadNo ratings yet
- Pathophysiology (Cerebrovascular Accident Hemorrhagic Right Lobe)Document4 pagesPathophysiology (Cerebrovascular Accident Hemorrhagic Right Lobe)jhonkivenNo ratings yet
- Patho CirrhosisDocument1 pagePatho CirrhosisPearl Angeli SabalNo ratings yet
- ESRD PathophysiologyDocument2 pagesESRD Pathophysiologynursing concept mapsNo ratings yet
- All PathoDocument2 pagesAll PathoroseasNo ratings yet
- Pa Tho Physiology of PIHDocument2 pagesPa Tho Physiology of PIHCarren_Louise__8090No ratings yet
- Acute Lymphoblastic Leukemia: Predisposing Factors: Precipitating FactorsDocument3 pagesAcute Lymphoblastic Leukemia: Predisposing Factors: Precipitating FactorsKasandra Dawn Moquia BerisoNo ratings yet
- Angina PectorisDocument1 pageAngina PectorisAlissa MaghopoyNo ratings yet
- Fluid Therapy in ICU: Dr. Basuki Rahmat SP - AnDocument84 pagesFluid Therapy in ICU: Dr. Basuki Rahmat SP - AndianNo ratings yet
- Biology 1 EditedDocument336 pagesBiology 1 EditedEmperor GooseNo ratings yet
- Cva PathoDocument2 pagesCva Pathokriska_ortizNo ratings yet
- CeVD, MI, HCVD & Atrial Fibrillation PathophysiologyDocument3 pagesCeVD, MI, HCVD & Atrial Fibrillation PathophysiologyJjessmar Bolivar FamaNo ratings yet
- Modifiable Risk Factors Non - Modifiable Risk Factors: LegendDocument2 pagesModifiable Risk Factors Non - Modifiable Risk Factors: LegendWendy Escalante100% (1)
- PATHODocument2 pagesPATHOWendy EscalanteNo ratings yet
- Cholecystitis-Pathophysiology - Updated 2Document2 pagesCholecystitis-Pathophysiology - Updated 2Kylle AlimosaNo ratings yet
- General Pathophysiology of Breast Cancer: Malinda Sirue, Bsn4 MODULE 2, Activity 101Document3 pagesGeneral Pathophysiology of Breast Cancer: Malinda Sirue, Bsn4 MODULE 2, Activity 101Esmareldah Henry SirueNo ratings yet
- Sirosis HepatisDocument65 pagesSirosis HepatisIntania Fadilla100% (1)
- Acute Lymphoblastic Leukemia Pathophysiology: Predisposing Factors: Etiology: Precipitating FactorsDocument3 pagesAcute Lymphoblastic Leukemia Pathophysiology: Predisposing Factors: Etiology: Precipitating FactorsKyla ValenciaNo ratings yet
- O High Fat, High Carbohydrate o Caffeinated and Carbonated o 73 Years Old o MaleDocument4 pagesO High Fat, High Carbohydrate o Caffeinated and Carbonated o 73 Years Old o MaleJoherNo ratings yet
- Anemia Ugib PathoDocument2 pagesAnemia Ugib PathoAj GoNo ratings yet
- Cirrhosis Hepatic: DinadewisliDocument47 pagesCirrhosis Hepatic: DinadewisliwilmaNo ratings yet
- Congestive Heart Failure Secondary To Coronary Artery Disease PathophysiologyDocument5 pagesCongestive Heart Failure Secondary To Coronary Artery Disease PathophysiologyJanica MarinasNo ratings yet
- Hepatic Enceph PathophysioDocument1 pageHepatic Enceph PathophysioJessica FabroaNo ratings yet
- Fast Facts: Leucemia: Desde la mutación genética inicial hasta el apoyo para la supervivenciaFrom EverandFast Facts: Leucemia: Desde la mutación genética inicial hasta el apoyo para la supervivenciaNo ratings yet
- Fast Facts: Leukemia: From initial gene mutation to survivorship supportFrom EverandFast Facts: Leukemia: From initial gene mutation to survivorship supportNo ratings yet
- Fast Facts: Déficit en pyruvate kinase: Sensibilisation à cette maladie génétique rareFrom EverandFast Facts: Déficit en pyruvate kinase: Sensibilisation à cette maladie génétique rareRating: 4 out of 5 stars4/5 (1)
- Skill Lab #7: Abnormal ECG Interpretation and Treatment: Aed/DDocument10 pagesSkill Lab #7: Abnormal ECG Interpretation and Treatment: Aed/Dاكرم صالحينNo ratings yet
- Acute Kidney Injury Kidney Infection: ClasificationDocument1 pageAcute Kidney Injury Kidney Infection: ClasificationSiti RuchjayaniNo ratings yet
- My CVDocument11 pagesMy CVPatrick NdunguNo ratings yet
- Cardiac Catheterization Knowledge & Skills ChecklistDocument6 pagesCardiac Catheterization Knowledge & Skills ChecklistnorthweststaffingNo ratings yet
- GREGORY - Demencia Rápidamente ProgresivaDocument47 pagesGREGORY - Demencia Rápidamente ProgresivaUgalde López ReginaNo ratings yet
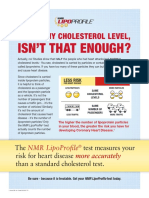
- Isn'T That Enough?: I Know My Cholesterol LevelDocument2 pagesIsn'T That Enough?: I Know My Cholesterol LevelgreatdeceivahNo ratings yet
- (JURNAL, Eng) A Retrospective Cohort Review of Prescribing in Hospitalised Patients With Heart Failure Using Beers Criteria and STOPP RecommendationsDocument7 pages(JURNAL, Eng) A Retrospective Cohort Review of Prescribing in Hospitalised Patients With Heart Failure Using Beers Criteria and STOPP RecommendationsAurellia Annisa WulandariNo ratings yet
- Med Surg Nursing Cheat Sheets 76 Cheat Sheets For Nursing Students Nodrm PDFDocument101 pagesMed Surg Nursing Cheat Sheets 76 Cheat Sheets For Nursing Students Nodrm PDFEya BaldostamonNo ratings yet
- High Risk PediatricsDocument207 pagesHigh Risk Pediatricsruby cubionaNo ratings yet
- Pemilihan Anastesi Penyakit JantungDocument10 pagesPemilihan Anastesi Penyakit JantungAndri HikmawanNo ratings yet
- LobectomyDocument3 pagesLobectomyJrosejorge TaparNo ratings yet
- Cardiovascular Risk Factors. Insights From Framingham Heart Study PDFDocument12 pagesCardiovascular Risk Factors. Insights From Framingham Heart Study PDFRafael Rivas BourdetNo ratings yet
- Ketesse Dosage & Drug Information MIMS - Com PhilippinesDocument1 pageKetesse Dosage & Drug Information MIMS - Com PhilippinesgjpaqueoNo ratings yet
- Investigation Report - (DOA) Death of PDL RICARTE, Jonathan y FloresDocument3 pagesInvestigation Report - (DOA) Death of PDL RICARTE, Jonathan y FloresLenar GamoraNo ratings yet
- PhysiologyWorkbook7 5Document267 pagesPhysiologyWorkbook7 5SophiaNo ratings yet
- مقارنات باطنيه عملي hpWDocument4 pagesمقارنات باطنيه عملي hpWcefolob289No ratings yet
- Case Presentation Liver CirrhosisDocument93 pagesCase Presentation Liver CirrhosismarestelbaguiocajesNo ratings yet
- Hipertensi UrgensiDocument26 pagesHipertensi UrgensidiegoNo ratings yet
- Systemic Circulation Arteries ContinuedDocument35 pagesSystemic Circulation Arteries ContinuedKristina ButeNo ratings yet
- List of Casualties Due To Typhoon YolandaDocument31 pagesList of Casualties Due To Typhoon YolandaSunStar Philippine NewsNo ratings yet
- Rheumatic Heart Disease Abx Prophylaxis For Young PatientsDocument2 pagesRheumatic Heart Disease Abx Prophylaxis For Young PatientsFathima Sheik KatherNo ratings yet
- CHF Case StudyDocument20 pagesCHF Case StudyDelia Soriano AlingayaoNo ratings yet
- Dissertation Topics in Cardiac AnaesthesiaDocument5 pagesDissertation Topics in Cardiac AnaesthesiaDoMyPapersMilwaukee100% (1)
- Presented by Yasha Ali Bangash & Pashmina Khan DPT Batch Ii Semester VDocument20 pagesPresented by Yasha Ali Bangash & Pashmina Khan DPT Batch Ii Semester VAngelic khanNo ratings yet
- Mls1 Medical Terminologies Sept 1Document5 pagesMls1 Medical Terminologies Sept 1Lian Marie ViñasNo ratings yet
- Writing Assignment PDFDocument3 pagesWriting Assignment PDFAmar EliasNo ratings yet
- Case Study 1Document9 pagesCase Study 1andry natanel tonyNo ratings yet
- DyslipidemiaDocument2 pagesDyslipidemiaapi-607717122No ratings yet
- Arrows Consele PDFDocument221 pagesArrows Consele PDFIsai Lara OsoriaNo ratings yet



















































































Download as doc, pdf, or txt
You might also like
- Coronary Artery Disease PathophysiologyDocument3 pagesCoronary Artery Disease Pathophysiologynursing concept maps40% (5)
- Acute Ischemic Stroke Concept MapDocument6 pagesAcute Ischemic Stroke Concept MapMoonyeen Jann Casera Balic100% (2)
- Acute Lymphoblastic Leukemia Pathophysiology: Precipitating Factors: Etiology: Predisposing FactorsDocument3 pagesAcute Lymphoblastic Leukemia Pathophysiology: Precipitating Factors: Etiology: Predisposing FactorsromelynNo ratings yet
- Pathophysiology of ALL (Diagram)Document3 pagesPathophysiology of ALL (Diagram)Joann100% (77)
- Nstemi PathoDocument2 pagesNstemi PathoSheana TmplNo ratings yet
- Congestive Heart Failure Pathophysiology Schematic DiagramDocument3 pagesCongestive Heart Failure Pathophysiology Schematic DiagramJasleen KaurNo ratings yet
- 72-HR ChickDocument16 pages72-HR Chick411452123100% (1)
- Pathophysiology of MI, COPD and BPHDocument10 pagesPathophysiology of MI, COPD and BPHSarah Lim100% (1)
- Pathophysiology of Hypertensive Cardiovascular Disease PDFDocument3 pagesPathophysiology of Hypertensive Cardiovascular Disease PDFAbdelrahman GalalNo ratings yet
- Pathophysiology of Cerebrovascular AccidentDocument3 pagesPathophysiology of Cerebrovascular AccidentByron Paz Te100% (1)
- Pathophysiology of cholangiocarcinomaJAYCERDocument3 pagesPathophysiology of cholangiocarcinomaJAYCERirish_estrellaNo ratings yet
- Pathophysiology of HypovolemiaDocument1 pagePathophysiology of HypovolemiaSheana TmplNo ratings yet
- Pathophysio of HCDDocument3 pagesPathophysio of HCDhoney requermeNo ratings yet
- O SHOCKDocument2 pagesO SHOCKkhurvy999No ratings yet
- Predisposing Factors: Precipitating Factors:: KidneysDocument1 pagePredisposing Factors: Precipitating Factors:: KidneysChe CacatianNo ratings yet
- Acute Coronary Syndrome PathophysiologyDocument3 pagesAcute Coronary Syndrome PathophysiologyJocelle Joy OrellanedaNo ratings yet
- Pathophysiolgoy Coronary Artery DiseaseDocument3 pagesPathophysiolgoy Coronary Artery DiseaseNursesLabs.comNo ratings yet
- Shanz - Clinpath Le1Document7 pagesShanz - Clinpath Le1Petrina XuNo ratings yet
- Shock and Multi OrganDocument90 pagesShock and Multi OrganElishaNo ratings yet
- NCM 106 Module 2 Lesson 1.1Document3 pagesNCM 106 Module 2 Lesson 1.1Joselyn M. LachicaNo ratings yet
- Whatsapp: +1 (402) 235-1397Document312 pagesWhatsapp: +1 (402) 235-1397Khushi RNo ratings yet
- Pa Tho PhysiologyDocument2 pagesPa Tho Physiologydavica0413No ratings yet
- Pa Tho Physiology of Cva... by Mizzy BaylonDocument3 pagesPa Tho Physiology of Cva... by Mizzy BaylonmizzybaylonNo ratings yet
- Pathophysiology: Predisposing Factors Precipitating FactorsDocument3 pagesPathophysiology: Predisposing Factors Precipitating FactorsFc ßobby HechanovaNo ratings yet
- Clinicopharmacological ConferenceDocument7 pagesClinicopharmacological ConferenceNestley TiongsonNo ratings yet
- Pre Eclampsia of Severe FeaturesDocument3 pagesPre Eclampsia of Severe FeaturesPrincess Diane S. VillegasNo ratings yet
- Pathophysiology of Acute Renal FailureDocument2 pagesPathophysiology of Acute Renal Failureminangsung minangnengNo ratings yet
- Pathophysiology of AllDocument1 pagePathophysiology of AllBGHMC PEDIAHONo ratings yet
- Pathophysio - Stemi - FinalDocument4 pagesPathophysio - Stemi - FinalPrincessDianneNo ratings yet
- Precipitating Factors:: Myocardial Cell Death (NecrosisDocument2 pagesPrecipitating Factors:: Myocardial Cell Death (NecrosisLean Ashly MacarubboNo ratings yet
- PATHOPHYDocument3 pagesPATHOPHYArlly Faena AbadNo ratings yet
- Pathophysiology (Cerebrovascular Accident Hemorrhagic Right Lobe)Document4 pagesPathophysiology (Cerebrovascular Accident Hemorrhagic Right Lobe)jhonkivenNo ratings yet
- Patho CirrhosisDocument1 pagePatho CirrhosisPearl Angeli SabalNo ratings yet
- ESRD PathophysiologyDocument2 pagesESRD Pathophysiologynursing concept mapsNo ratings yet
- All PathoDocument2 pagesAll PathoroseasNo ratings yet
- Pa Tho Physiology of PIHDocument2 pagesPa Tho Physiology of PIHCarren_Louise__8090No ratings yet
- Acute Lymphoblastic Leukemia: Predisposing Factors: Precipitating FactorsDocument3 pagesAcute Lymphoblastic Leukemia: Predisposing Factors: Precipitating FactorsKasandra Dawn Moquia BerisoNo ratings yet
- Angina PectorisDocument1 pageAngina PectorisAlissa MaghopoyNo ratings yet
- Fluid Therapy in ICU: Dr. Basuki Rahmat SP - AnDocument84 pagesFluid Therapy in ICU: Dr. Basuki Rahmat SP - AndianNo ratings yet
- Biology 1 EditedDocument336 pagesBiology 1 EditedEmperor GooseNo ratings yet
- Cva PathoDocument2 pagesCva Pathokriska_ortizNo ratings yet
- CeVD, MI, HCVD & Atrial Fibrillation PathophysiologyDocument3 pagesCeVD, MI, HCVD & Atrial Fibrillation PathophysiologyJjessmar Bolivar FamaNo ratings yet
- Modifiable Risk Factors Non - Modifiable Risk Factors: LegendDocument2 pagesModifiable Risk Factors Non - Modifiable Risk Factors: LegendWendy Escalante100% (1)
- PATHODocument2 pagesPATHOWendy EscalanteNo ratings yet
- Cholecystitis-Pathophysiology - Updated 2Document2 pagesCholecystitis-Pathophysiology - Updated 2Kylle AlimosaNo ratings yet
- General Pathophysiology of Breast Cancer: Malinda Sirue, Bsn4 MODULE 2, Activity 101Document3 pagesGeneral Pathophysiology of Breast Cancer: Malinda Sirue, Bsn4 MODULE 2, Activity 101Esmareldah Henry SirueNo ratings yet
- Sirosis HepatisDocument65 pagesSirosis HepatisIntania Fadilla100% (1)
- Acute Lymphoblastic Leukemia Pathophysiology: Predisposing Factors: Etiology: Precipitating FactorsDocument3 pagesAcute Lymphoblastic Leukemia Pathophysiology: Predisposing Factors: Etiology: Precipitating FactorsKyla ValenciaNo ratings yet
- O High Fat, High Carbohydrate o Caffeinated and Carbonated o 73 Years Old o MaleDocument4 pagesO High Fat, High Carbohydrate o Caffeinated and Carbonated o 73 Years Old o MaleJoherNo ratings yet
- Anemia Ugib PathoDocument2 pagesAnemia Ugib PathoAj GoNo ratings yet
- Cirrhosis Hepatic: DinadewisliDocument47 pagesCirrhosis Hepatic: DinadewisliwilmaNo ratings yet
- Congestive Heart Failure Secondary To Coronary Artery Disease PathophysiologyDocument5 pagesCongestive Heart Failure Secondary To Coronary Artery Disease PathophysiologyJanica MarinasNo ratings yet
- Hepatic Enceph PathophysioDocument1 pageHepatic Enceph PathophysioJessica FabroaNo ratings yet
- Fast Facts: Leucemia: Desde la mutación genética inicial hasta el apoyo para la supervivenciaFrom EverandFast Facts: Leucemia: Desde la mutación genética inicial hasta el apoyo para la supervivenciaNo ratings yet
- Fast Facts: Leukemia: From initial gene mutation to survivorship supportFrom EverandFast Facts: Leukemia: From initial gene mutation to survivorship supportNo ratings yet
- Fast Facts: Déficit en pyruvate kinase: Sensibilisation à cette maladie génétique rareFrom EverandFast Facts: Déficit en pyruvate kinase: Sensibilisation à cette maladie génétique rareRating: 4 out of 5 stars4/5 (1)
- Skill Lab #7: Abnormal ECG Interpretation and Treatment: Aed/DDocument10 pagesSkill Lab #7: Abnormal ECG Interpretation and Treatment: Aed/Dاكرم صالحينNo ratings yet
- Acute Kidney Injury Kidney Infection: ClasificationDocument1 pageAcute Kidney Injury Kidney Infection: ClasificationSiti RuchjayaniNo ratings yet
- My CVDocument11 pagesMy CVPatrick NdunguNo ratings yet
- Cardiac Catheterization Knowledge & Skills ChecklistDocument6 pagesCardiac Catheterization Knowledge & Skills ChecklistnorthweststaffingNo ratings yet
- GREGORY - Demencia Rápidamente ProgresivaDocument47 pagesGREGORY - Demencia Rápidamente ProgresivaUgalde López ReginaNo ratings yet
- Isn'T That Enough?: I Know My Cholesterol LevelDocument2 pagesIsn'T That Enough?: I Know My Cholesterol LevelgreatdeceivahNo ratings yet
- (JURNAL, Eng) A Retrospective Cohort Review of Prescribing in Hospitalised Patients With Heart Failure Using Beers Criteria and STOPP RecommendationsDocument7 pages(JURNAL, Eng) A Retrospective Cohort Review of Prescribing in Hospitalised Patients With Heart Failure Using Beers Criteria and STOPP RecommendationsAurellia Annisa WulandariNo ratings yet
- Med Surg Nursing Cheat Sheets 76 Cheat Sheets For Nursing Students Nodrm PDFDocument101 pagesMed Surg Nursing Cheat Sheets 76 Cheat Sheets For Nursing Students Nodrm PDFEya BaldostamonNo ratings yet
- High Risk PediatricsDocument207 pagesHigh Risk Pediatricsruby cubionaNo ratings yet
- Pemilihan Anastesi Penyakit JantungDocument10 pagesPemilihan Anastesi Penyakit JantungAndri HikmawanNo ratings yet
- LobectomyDocument3 pagesLobectomyJrosejorge TaparNo ratings yet
- Cardiovascular Risk Factors. Insights From Framingham Heart Study PDFDocument12 pagesCardiovascular Risk Factors. Insights From Framingham Heart Study PDFRafael Rivas BourdetNo ratings yet
- Ketesse Dosage & Drug Information MIMS - Com PhilippinesDocument1 pageKetesse Dosage & Drug Information MIMS - Com PhilippinesgjpaqueoNo ratings yet
- Investigation Report - (DOA) Death of PDL RICARTE, Jonathan y FloresDocument3 pagesInvestigation Report - (DOA) Death of PDL RICARTE, Jonathan y FloresLenar GamoraNo ratings yet
- PhysiologyWorkbook7 5Document267 pagesPhysiologyWorkbook7 5SophiaNo ratings yet
- مقارنات باطنيه عملي hpWDocument4 pagesمقارنات باطنيه عملي hpWcefolob289No ratings yet
- Case Presentation Liver CirrhosisDocument93 pagesCase Presentation Liver CirrhosismarestelbaguiocajesNo ratings yet
- Hipertensi UrgensiDocument26 pagesHipertensi UrgensidiegoNo ratings yet
- Systemic Circulation Arteries ContinuedDocument35 pagesSystemic Circulation Arteries ContinuedKristina ButeNo ratings yet
- List of Casualties Due To Typhoon YolandaDocument31 pagesList of Casualties Due To Typhoon YolandaSunStar Philippine NewsNo ratings yet
- Rheumatic Heart Disease Abx Prophylaxis For Young PatientsDocument2 pagesRheumatic Heart Disease Abx Prophylaxis For Young PatientsFathima Sheik KatherNo ratings yet
- CHF Case StudyDocument20 pagesCHF Case StudyDelia Soriano AlingayaoNo ratings yet
- Dissertation Topics in Cardiac AnaesthesiaDocument5 pagesDissertation Topics in Cardiac AnaesthesiaDoMyPapersMilwaukee100% (1)
- Presented by Yasha Ali Bangash & Pashmina Khan DPT Batch Ii Semester VDocument20 pagesPresented by Yasha Ali Bangash & Pashmina Khan DPT Batch Ii Semester VAngelic khanNo ratings yet
- Mls1 Medical Terminologies Sept 1Document5 pagesMls1 Medical Terminologies Sept 1Lian Marie ViñasNo ratings yet
- Writing Assignment PDFDocument3 pagesWriting Assignment PDFAmar EliasNo ratings yet
- Case Study 1Document9 pagesCase Study 1andry natanel tonyNo ratings yet
- DyslipidemiaDocument2 pagesDyslipidemiaapi-607717122No ratings yet
- Arrows Consele PDFDocument221 pagesArrows Consele PDFIsai Lara OsoriaNo ratings yet