Download as pdf or txt
You might also like
- Anterior and Posterio Pituitary GlandDocument7 pagesAnterior and Posterio Pituitary GlandAnny AlvrzNo ratings yet
- Niveis Hormonais e TabagismoDocument9 pagesNiveis Hormonais e TabagismoDoc Nelson JuniorNo ratings yet
- Smoking and ThyroidDocument27 pagesSmoking and ThyroidEla03No ratings yet
- 5 OfficeDocument30 pages5 Officeejohn8340No ratings yet
- Chest: Systemic Effects of SmokingDocument10 pagesChest: Systemic Effects of SmokingArlen ResnawaldiNo ratings yet
- Smoking and Autoimmune Thyroid Disease: The Plot ThickensDocument4 pagesSmoking and Autoimmune Thyroid Disease: The Plot ThickensfahrulrozyNo ratings yet
- Physiological Effects On SmokingDocument6 pagesPhysiological Effects On SmokingReyki Yudho HNo ratings yet
- Oxidative Stress and LFT ReviewDocument6 pagesOxidative Stress and LFT ReviewScienceGenomeNo ratings yet
- Fumar, Cortisol y NicotinaDocument8 pagesFumar, Cortisol y NicotinaFranco LaviaNo ratings yet
- Acupuncture Treatment With ST9, LI18, and Acupressure K27 For Multi Nodular Goitre: A Case StudyDocument6 pagesAcupuncture Treatment With ST9, LI18, and Acupressure K27 For Multi Nodular Goitre: A Case StudySyam ChandrasekharanNo ratings yet
- Goitre Et Nodule ThyrogdienDocument4 pagesGoitre Et Nodule ThyrogdienKeishaNo ratings yet
- WJMH 33 143 PDFDocument18 pagesWJMH 33 143 PDFEka PriyantiNo ratings yet
- Evaluation of The Impact of Cigarette Smoking OnDocument6 pagesEvaluation of The Impact of Cigarette Smoking OnBerenice SánchezNo ratings yet
- Smoking 4Document8 pagesSmoking 4Clara CurcaNo ratings yet
- Effects of Smoking On Cardiovascular Function: The Role of Nicotine and Carbon MonoxideDocument17 pagesEffects of Smoking On Cardiovascular Function: The Role of Nicotine and Carbon Monoxide-No ratings yet
- Inbound 3275447624256708487Document4 pagesInbound 3275447624256708487dorj.hongorooNo ratings yet
- Case StudyDocument10 pagesCase StudyHomaira AlamNo ratings yet
- Smoking and Periodontal DiseaseDocument5 pagesSmoking and Periodontal Diseasegustavo.lopez.rocha1990No ratings yet
- Title: A Case Study On Iron Deficiency and Its Effects On Male/female Students Who Take Cigarette Smoke at The University of Goroka, Papua New GuineaDocument6 pagesTitle: A Case Study On Iron Deficiency and Its Effects On Male/female Students Who Take Cigarette Smoke at The University of Goroka, Papua New GuineaOtana ENOPANo ratings yet
- Hypothyroidism-Etiologies, Evaluation, and Emergency CareDocument16 pagesHypothyroidism-Etiologies, Evaluation, and Emergency CareUlises CruzNo ratings yet
- S05 108,+ (690+to+700)Document11 pagesS05 108,+ (690+to+700)Muhammad HassanNo ratings yet
- Smoking EffectsDocument9 pagesSmoking EffectsDafneSalvatierraAguilarNo ratings yet
- Top 10 Environmental and Nutrition Disorders PDFDocument87 pagesTop 10 Environmental and Nutrition Disorders PDFAdrian CaballesNo ratings yet
- Health Risks: Smoking In-DepthDocument6 pagesHealth Risks: Smoking In-DepthsirsriNo ratings yet
- Smoking Should Be Banned Permanently in The UAEDocument6 pagesSmoking Should Be Banned Permanently in The UAESameh SalahNo ratings yet
- Tobacco Smoking On CVD PDFDocument6 pagesTobacco Smoking On CVD PDFRodriNo ratings yet
- Mutagens - BONDOCDocument2 pagesMutagens - BONDOCMilani Joy LazoNo ratings yet
- Evils of SmokingDocument4 pagesEvils of SmokingAliasgar JamaliNo ratings yet
- Hypothyroidism in The Older Population: Review Open AccessDocument10 pagesHypothyroidism in The Older Population: Review Open Accessفرح صالحNo ratings yet
- TSH Ijms 22 06521 v2Document62 pagesTSH Ijms 22 06521 v2Satish SinghNo ratings yet
- Informacion Periodontitis y FumarDocument3 pagesInformacion Periodontitis y FumarFelipe MartinezNo ratings yet
- Beneficial Effects of Nicotine and Cigarette Smoking: The Real, The Possible and The SpuriousDocument16 pagesBeneficial Effects of Nicotine and Cigarette Smoking: The Real, The Possible and The SpuriousPallat Angel JhoannaNo ratings yet
- CH 02Document22 pagesCH 02DumitruCheleNo ratings yet
- Cigarette Smoking, Pregnancy and The Development FetusDocument3 pagesCigarette Smoking, Pregnancy and The Development FetusJayanth Philip MarottipuzhaNo ratings yet
- دکتر حسینی نیاDocument109 pagesدکتر حسینی نیاMasoud DoroodgarNo ratings yet
- Research Paper About Cigarette Smoking in The PhilippinesDocument7 pagesResearch Paper About Cigarette Smoking in The PhilippinesyvunfevgfNo ratings yet
- Tobacco & CarcinogenesisDocument15 pagesTobacco & CarcinogenesisSonalee ShahNo ratings yet
- R.S.Trivedi, A.K.Anand - Jamnagar (Gujarat) : Effect of Smoking On Lipid ProfileDocument3 pagesR.S.Trivedi, A.K.Anand - Jamnagar (Gujarat) : Effect of Smoking On Lipid ProfileutarinuNo ratings yet
- Smoking and Periodontal DiseasesDocument9 pagesSmoking and Periodontal DiseasesSnowNo ratings yet
- Chapter 3Document3 pagesChapter 3Cayanong Joel Jr I.No ratings yet
- Effects of Cigarette Smoking Research PaperDocument4 pagesEffects of Cigarette Smoking Research Papergtnntxwgf100% (1)
- 52 1 58 PDFDocument16 pages52 1 58 PDFtankofdoom 4No ratings yet
- Tobacco Consumption and The Effects 2 (Autosaved) .EditedDocument10 pagesTobacco Consumption and The Effects 2 (Autosaved) .EditedMarvin CJNo ratings yet
- Cigarettes (Tobacco Smoke) Link To Oral Leukoplakia (White Sore Patches Disease) Cause From EpigeneticsDocument2 pagesCigarettes (Tobacco Smoke) Link To Oral Leukoplakia (White Sore Patches Disease) Cause From Epigeneticsapi-350797283No ratings yet
- Cigarette Smoking Literature ReviewDocument4 pagesCigarette Smoking Literature Reviewgvzrg8jy100% (1)
- Goiter - StatPearls - NCBI BookshelfDocument9 pagesGoiter - StatPearls - NCBI BookshelfnewmowneeshNo ratings yet
- Wo Week 4 (Hyperthyroidism)Document12 pagesWo Week 4 (Hyperthyroidism)Theddyon BhenlieNo ratings yet
- Merokok Dan Penyakit CVSDocument4 pagesMerokok Dan Penyakit CVSIncredibleNo ratings yet
- Artikel Ibnu Fiksani Riski - Bismillah FinishDocument5 pagesArtikel Ibnu Fiksani Riski - Bismillah FinishDidik PujiyantoNo ratings yet
- Effectofsmokingon Red Blood Cells Count Hemoglobin Concentrationand Red CellindicesDocument5 pagesEffectofsmokingon Red Blood Cells Count Hemoglobin Concentrationand Red CellindicesIvan Matthew SuperioNo ratings yet
- DiscussionDocument5 pagesDiscussioncnonsowonNo ratings yet
- HHS Public Access: Smoking and The Risk of Type 2 DiabetesDocument11 pagesHHS Public Access: Smoking and The Risk of Type 2 DiabetesViolet MillerNo ratings yet
- 0120 2448 Amc 44 03 8Document8 pages0120 2448 Amc 44 03 8Lejla HusicNo ratings yet
- Hypothyroidism Is A Condition of Reduced Thyroid Functioning Resulting in Insufficient Amounts of Thyroid Hormones T3 and T4Document3 pagesHypothyroidism Is A Condition of Reduced Thyroid Functioning Resulting in Insufficient Amounts of Thyroid Hormones T3 and T4Meha FatimaNo ratings yet
- Health Consequences of Sustained Smoking Cessation FinalDocument5 pagesHealth Consequences of Sustained Smoking Cessation FinalAmin Mohamed Amin DemerdashNo ratings yet
- Addicted To SmokeDocument2 pagesAddicted To SmokejfafkdiutbuvzgewtaNo ratings yet
- Seminar PresentationDocument14 pagesSeminar PresentationMICHEALNo ratings yet
- Secondhand Smoke Exposure Triggered Respiratory Cardiothoracic Diseases: Secondhand Smoke Exposure Induces Harmful HealthFrom EverandSecondhand Smoke Exposure Triggered Respiratory Cardiothoracic Diseases: Secondhand Smoke Exposure Induces Harmful HealthNo ratings yet
- The Human Gut-Liver-Axis in Health and DiseaseFrom EverandThe Human Gut-Liver-Axis in Health and DiseaseAleksander KragNo ratings yet
- Orbital Apex Syndrome Secondary To Herpes Zoster OphthalmicusDocument4 pagesOrbital Apex Syndrome Secondary To Herpes Zoster OphthalmicusYosiita KartinaaNo ratings yet
- Balls Template 16x9Document5 pagesBalls Template 16x9Yosiita KartinaaNo ratings yet
- Dia Care-1996-Frati-112-8Document7 pagesDia Care-1996-Frati-112-8Yosiita KartinaaNo ratings yet
- Types of CrimeDocument2 pagesTypes of CrimeYosiita KartinaaNo ratings yet
- Clinical Evaluation of Corneal Ulcer Among Patients Attending Teaching Hospital PDFDocument4 pagesClinical Evaluation of Corneal Ulcer Among Patients Attending Teaching Hospital PDFYosiita KartinaaNo ratings yet
- Management of Corneal Ulcer PDFDocument2 pagesManagement of Corneal Ulcer PDFYosiita KartinaaNo ratings yet
- Prevalence of Contact Lens-Related Complications Among Wearers in Saudi ArabiaDocument6 pagesPrevalence of Contact Lens-Related Complications Among Wearers in Saudi ArabiaYosiita KartinaaNo ratings yet
- The Prevalence and Determinants of Pterygium in Rural Areas: SciencedirectDocument5 pagesThe Prevalence and Determinants of Pterygium in Rural Areas: SciencedirectYosiita KartinaaNo ratings yet
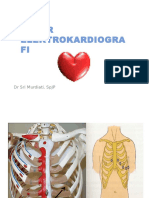
- Dasar Elektrokardiogra Fi: DR Sri Murdiati, SPJPDocument18 pagesDasar Elektrokardiogra Fi: DR Sri Murdiati, SPJPYosiita KartinaaNo ratings yet
- The Best Prescription Is KnowledgeDocument19 pagesThe Best Prescription Is KnowledgeYosiita KartinaaNo ratings yet
- CHN Answer - ReviewerDocument5 pagesCHN Answer - Reviewerdhma.gacutan.uiNo ratings yet
- AP Bio 2019Document108 pagesAP Bio 2019danielyskim1119No ratings yet
- Maternal Behavior in PigsDocument8 pagesMaternal Behavior in PigsThu Y 2007No ratings yet
- Chapter One 1.1 Background of The StudyDocument65 pagesChapter One 1.1 Background of The StudyIgbani VictoryNo ratings yet
- Content 3Document128 pagesContent 3Mohamed AbbasNo ratings yet
- Attitude 0F Nursing Mothers Towards Exclusive Breast Feeding Among Maried Women Aged 18-45 YearsDocument47 pagesAttitude 0F Nursing Mothers Towards Exclusive Breast Feeding Among Maried Women Aged 18-45 YearsUsman Ahmad TijjaniNo ratings yet
- Post PartumDocument22 pagesPost PartumShaira Mae Yante RomeroNo ratings yet
- Chapter 10 ANATOMY AND PHYSIOLOGYDocument5 pagesChapter 10 ANATOMY AND PHYSIOLOGYAngela Mae MeriñoNo ratings yet
- Endocrine Passmedicine & Onexamination Notes 2016 PDFDocument96 pagesEndocrine Passmedicine & Onexamination Notes 2016 PDFsepan abdullahNo ratings yet
- Clinical Characterization of Patients WithDocument4 pagesClinical Characterization of Patients WithPaulo Eduardo CampanaNo ratings yet
- ABS Endocrinology PDFDocument59 pagesABS Endocrinology PDFMichael Olivier WNo ratings yet
- Materi 5 Endokrinologi Selama Siklus EstrusDocument42 pagesMateri 5 Endokrinologi Selama Siklus EstrusSaparuddin UINAMNo ratings yet
- Endocrine SystemDocument27 pagesEndocrine Systemcardos cherry100% (1)
- MCQS On PHYSIOLOGY OF LACTATIONDocument6 pagesMCQS On PHYSIOLOGY OF LACTATIONnighatkhanNo ratings yet
- Bioassay of OxytocinDocument13 pagesBioassay of OxytocinGoogle IndiaNo ratings yet
- Gyn Infertility PresentationDocument30 pagesGyn Infertility Presentationapi-507364479No ratings yet
- Fcps Past Papers PartDocument25 pagesFcps Past Papers PartBeena Muhammad Fahad100% (1)
- LactationDocument8 pagesLactationDevuchandana RNo ratings yet
- DR Yog TT Notes Rishikesh Training - Docx 2023Document21 pagesDR Yog TT Notes Rishikesh Training - Docx 2023mechevegadiazNo ratings yet
- Structure of The Lactating Breast: Lactation Is The Process by Which Milk Is Synthesized and Secreted From The MammaryDocument5 pagesStructure of The Lactating Breast: Lactation Is The Process by Which Milk Is Synthesized and Secreted From The Mammaryratna putriNo ratings yet
- Immune Response (Hormones) : Hawler Medical University College of Medicine Department: MicrobiologyDocument25 pagesImmune Response (Hormones) : Hawler Medical University College of Medicine Department: Microbiologyla.instagramawaNo ratings yet
- From PMS To MenopauseDocument196 pagesFrom PMS To MenopauseWeemizo تNo ratings yet
- Gynecology StudyguideDocument39 pagesGynecology StudyguideGameron777No ratings yet
- Unit 12Document14 pagesUnit 12KumareshNo ratings yet
- (Gyne) 2.1 PCOS, Hyperandrogenism & Hyperprolactenemia (OnaCruz) - WiniDocument10 pages(Gyne) 2.1 PCOS, Hyperandrogenism & Hyperprolactenemia (OnaCruz) - WiniDexter IanNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka: Confirmation For Registration of Subjects For DissertationDocument19 pagesRajiv Gandhi University of Health Sciences, Karnataka: Confirmation For Registration of Subjects For DissertationRIYANo ratings yet
- Endocrine 1 PageDocument3 pagesEndocrine 1 PagetimbitNo ratings yet
- Adapting For MotherhoodDocument15 pagesAdapting For MotherhoodfilipCARbovaNo ratings yet
- Physiological Changes During Pregnancy: Presented By: Ms. Vruti PatelDocument44 pagesPhysiological Changes During Pregnancy: Presented By: Ms. Vruti PatelSANJEEV KUMARNo ratings yet