Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Drug StudyDocument7 pagesDrug StudyJohn Paulo MataNo ratings yet
- Vitamin and Mineral Deficiency ChecklistDocument5 pagesVitamin and Mineral Deficiency ChecklistKrishna DasNo ratings yet
- Molar PregnancyDocument5 pagesMolar Pregnancycwqdtgtf6hNo ratings yet
- Effective Hemodynamic Monitoring 2Document10 pagesEffective Hemodynamic Monitoring 2Shirley castañedaNo ratings yet
- NB Access Point ApplicationDocument18 pagesNB Access Point Applicationnarmatha.vannarajahNo ratings yet
- Rapid Plasma Reagin 2020Document6 pagesRapid Plasma Reagin 2020REMAN ALINGASANo ratings yet
- Appendix 4: Week 5 Pre-ReadingDocument4 pagesAppendix 4: Week 5 Pre-ReadinggamzeNo ratings yet
- Shapiro 1997Document6 pagesShapiro 1997JohnnyNo ratings yet
- NCLEX RN Practice Test 5Document6 pagesNCLEX RN Practice Test 5Xiao Wei Ka HardiansyahNo ratings yet
- Local Drug Delivery in PeriodonticsDocument56 pagesLocal Drug Delivery in PeriodonticsAnuj Singh PariharNo ratings yet
- Cyclo ThermDocument18 pagesCyclo ThermSmitha V Gowda100% (1)
- Dinesh RamDocument1 pageDinesh RamchandanNo ratings yet
- Cardiology 1Document60 pagesCardiology 1ChibuNo ratings yet
- EEG Lecture Introduction To EEGDocument62 pagesEEG Lecture Introduction To EEGSada Twins100% (2)
- Diabetic Foot UlcersDocument13 pagesDiabetic Foot UlcersShanmuga SundaramNo ratings yet
- Ospe 2022Document25 pagesOspe 2022jtyqpjptqr100% (1)
- PoliomyelitisDocument4 pagesPoliomyelitisJohn Paul NavaltaNo ratings yet
- Kanski'S: Clinical OphthalmologyDocument504 pagesKanski'S: Clinical OphthalmologyMohin hossain100% (1)
- Case Scenario - PulmonaryDocument2 pagesCase Scenario - PulmonaryCHRISTINE JULIANENo ratings yet
- Inflammatory Lesions of The JawsDocument54 pagesInflammatory Lesions of The JawsAi Rafikah Nurpratiwi100% (1)
- TakebackyourlifebookDocument94 pagesTakebackyourlifebookAnthony Lavado100% (1)
- Anaesthetic Management of Obese PatientDocument53 pagesAnaesthetic Management of Obese PatientpriyadikkalaNo ratings yet
- Cerebral Localization Parietal Lobe SignsDocument34 pagesCerebral Localization Parietal Lobe SignsManice BastinenNo ratings yet
- Module 2Document3 pagesModule 2Esmareldah Henry SirueNo ratings yet
- TUBERCLUOSIS MCQS, ZSMU, UkraineDocument26 pagesTUBERCLUOSIS MCQS, ZSMU, UkraineDrRaghavender Reddy100% (1)
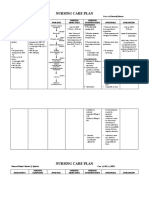
- Nursing Care Plan-Mam LazoDocument7 pagesNursing Care Plan-Mam LazoGayLah MomblancoNo ratings yet
- Physical Examination Related NutritionDocument40 pagesPhysical Examination Related NutritionYohan SamudraNo ratings yet
- Cefuroxime Drug StudyDocument2 pagesCefuroxime Drug StudyDanica Kate Galleon100% (1)
- Ismail's Undergraduate ThesisDocument82 pagesIsmail's Undergraduate ThesisAbiola IbrahimNo ratings yet
- COLLEGE OF ST. JOHN - ROXAS Member: Association ofDocument5 pagesCOLLEGE OF ST. JOHN - ROXAS Member: Association ofCrisha Ann Billones Bacuta0% (1)