
Bell's Palsy and Acyclovir
Bell's Palsy and Acyclovir
You might also like
- Laporan Praktikum Evidence Based Medicine (EBM)Document13 pagesLaporan Praktikum Evidence Based Medicine (EBM)LalaNo ratings yet
- International Conference Vote of ThanksDocument1 pageInternational Conference Vote of ThanksRini Kaithamangalam Abraham85% (13)
- Challenges of OBDocument10 pagesChallenges of OBGeetanjali Soni 1937629No ratings yet
- PDF BelpalsyDocument4 pagesPDF Belpalsygoche29No ratings yet
- Hirano 1999Document7 pagesHirano 1999LitaDwiNo ratings yet
- Comparison Between The Efficacy of Steroids and Acyclovir in The Management of Patients With Bells PalsyDocument5 pagesComparison Between The Efficacy of Steroids and Acyclovir in The Management of Patients With Bells PalsyucenucenNo ratings yet
- An Evidence-Based Approach To The First SeizureDocument8 pagesAn Evidence-Based Approach To The First SeizureheribertoNo ratings yet
- Methods: Jeremy M. Hernandez, MD, PHD Jonathan Sherbino, MD, Med Data SourcesDocument2 pagesMethods: Jeremy M. Hernandez, MD, PHD Jonathan Sherbino, MD, Med Data SourcesabbbabbbNo ratings yet
- Papel de La Estimulación Eléctrica Añadida A La Terapia Convencional en Pacientes Con Parálisis Facial (De Campana) IdiopáticaDocument7 pagesPapel de La Estimulación Eléctrica Añadida A La Terapia Convencional en Pacientes Con Parálisis Facial (De Campana) IdiopáticaandresNo ratings yet
- The Efficacy of Acupuncture in The Treatment of Bell's Palsy SequelaeDocument11 pagesThe Efficacy of Acupuncture in The Treatment of Bell's Palsy Sequelaeseptiani hasibuanNo ratings yet
- The Effect of Prednisolone On Sequelae in Bell's PalsyDocument5 pagesThe Effect of Prednisolone On Sequelae in Bell's Palsyrara fifiNo ratings yet
- Comparison of Outcomes of The Epley and Self-Epley Maneuvers inDocument5 pagesComparison of Outcomes of The Epley and Self-Epley Maneuvers inYunie ArmyatiNo ratings yet
- A Comparison of Oral Procaterol and Albuterol in Reversible Airflow ObstructionDocument6 pagesA Comparison of Oral Procaterol and Albuterol in Reversible Airflow Obstructionparris shanyNo ratings yet
- Neurology Journal WNLDocument7 pagesNeurology Journal WNLDokter KarisNo ratings yet
- PotasiumDocument11 pagesPotasiumDesy YeyenNo ratings yet
- CD001869 AbstractDocument4 pagesCD001869 AbstractMarsya Yulinesia LoppiesNo ratings yet
- Exercise Recommendations in PatientsDocument4 pagesExercise Recommendations in PatientsAleCsss123No ratings yet
- Bells PalsyDocument9 pagesBells PalsysasoyNo ratings yet
- Pulsed Radiofrequency ofDocument8 pagesPulsed Radiofrequency ofDiego Pinto PatroniNo ratings yet
- Evidence Based Medicine - CONSORT & AppraisalDocument52 pagesEvidence Based Medicine - CONSORT & AppraisalNurul Aulia AbdullahNo ratings yet
- NLR Bells PalsyDocument4 pagesNLR Bells PalsyIskandar HasanNo ratings yet
- Isopropyl Alcohol Nasal Inhalation For Nausea in The Emergency Department: A Randomized Controlled TrialDocument10 pagesIsopropyl Alcohol Nasal Inhalation For Nausea in The Emergency Department: A Randomized Controlled TrialNagib MuhammadNo ratings yet
- Anorexia 1Document4 pagesAnorexia 1Antonio Gil EscalanteNo ratings yet
- Etr80003 994 995Document2 pagesEtr80003 994 995Karen Mae PadillaNo ratings yet
- The Efficacy of Acupuncture in The Treatment of Bell's Palsy SequelaeDocument9 pagesThe Efficacy of Acupuncture in The Treatment of Bell's Palsy SequelaerezteevicNo ratings yet
- Factors Associated With Fast Recovery of Bell Palsy in ChildrenDocument6 pagesFactors Associated With Fast Recovery of Bell Palsy in ChildrenPutri GintingNo ratings yet
- Comparison of Conservative Therapy and Steroid Therapy For Bell's Palsy in ChildrenDocument6 pagesComparison of Conservative Therapy and Steroid Therapy For Bell's Palsy in ChildrenyogihermawanNo ratings yet
- Manoeuvres For The Treatment of Benign Positional Paroxysmal Vertigo A Systematic ReviewDocument9 pagesManoeuvres For The Treatment of Benign Positional Paroxysmal Vertigo A Systematic ReviewShresthaNo ratings yet
- Artikel RCTDocument8 pagesArtikel RCTSALSABILA PUTRI AULIANo ratings yet
- Nihms 562917Document9 pagesNihms 562917Vincent LivandyNo ratings yet
- Literature Review of Bells PalsyDocument5 pagesLiterature Review of Bells Palsyafmzxppzpvoluf100% (1)
- 658 PDFDocument6 pages658 PDFismail39 orthoNo ratings yet
- Steroids: The Clinical Problem of Bell's Palsy: Treatment Effective?Document5 pagesSteroids: The Clinical Problem of Bell's Palsy: Treatment Effective?putriseptinaNo ratings yet
- Treatments For Bronchiolitis in Children Do Not Seem Review: Commonly Used PharmacologicalDocument2 pagesTreatments For Bronchiolitis in Children Do Not Seem Review: Commonly Used Pharmacologicalapi-3711135No ratings yet
- 2008 Physical Therapy For Bell's Palsy (Idiopathic Facial Paralysis) (Review)Document24 pages2008 Physical Therapy For Bell's Palsy (Idiopathic Facial Paralysis) (Review)Francisco Antonó Castro WeithNo ratings yet
- Derry, Sheena Et Al 2014 Single Dose Dipyrone For Acute Postoperative PainDocument48 pagesDerry, Sheena Et Al 2014 Single Dose Dipyrone For Acute Postoperative PainlilingNo ratings yet
- Tecer 2004 Audiovestibular Functioning in Patients With Panic DisorderDocument6 pagesTecer 2004 Audiovestibular Functioning in Patients With Panic DisorderJuan Hernández GarcíaNo ratings yet
- [The Journal of Emergency Medicine 2011-jun vol. 40 iss. 6] Anna Engeln - Cardiopulmonary Resuscitation Outcome of Out-of-hospital Cardiac Arrest in Low-volume versus High-volume Emergency Departments_ (2011) [10.1016_j.Document1 page[The Journal of Emergency Medicine 2011-jun vol. 40 iss. 6] Anna Engeln - Cardiopulmonary Resuscitation Outcome of Out-of-hospital Cardiac Arrest in Low-volume versus High-volume Emergency Departments_ (2011) [10.1016_j.royhiranmay94No ratings yet
- IVIgG AmiloidDocument4 pagesIVIgG AmiloidyinvilllNo ratings yet
- Prednisolone or Acyclovir in Bell's Palsy: CorrespondenceDocument2 pagesPrednisolone or Acyclovir in Bell's Palsy: CorrespondenceSukhvinder Singh RanaNo ratings yet
- Art. - Qual - of Life AsthmaDocument6 pagesArt. - Qual - of Life AsthmaMaria MariaNo ratings yet
- Vit B12Document6 pagesVit B12Winda PradnyaNo ratings yet
- CorrespondenceDocument3 pagesCorrespondenceFayza RihastaraNo ratings yet
- The Natural History of Epilepsy: An Epidemiological View: ReviewDocument6 pagesThe Natural History of Epilepsy: An Epidemiological View: ReviewDiana LeonNo ratings yet
- Online Reference Notes - Nursing Research Drill AnswerDocument17 pagesOnline Reference Notes - Nursing Research Drill AnswerDairyl TagaroNo ratings yet
- The Recent History of AcupunctureDocument2 pagesThe Recent History of AcupunctureBhaskaranNo ratings yet
- 1 s2.0 S0002838X23001041Document2 pages1 s2.0 S0002838X23001041Võ Văn Phúc ToànNo ratings yet
- Summary Proceedings From The Neurology Group On Neonatal SeizuresDocument7 pagesSummary Proceedings From The Neurology Group On Neonatal SeizuresTran Trang AnhNo ratings yet
- Nested Case-Control Study of Children Presenting WDocument6 pagesNested Case-Control Study of Children Presenting Wbilal hadiNo ratings yet
- OutDocument5 pagesOutFayza RihastaraNo ratings yet
- Sieo Irizarry2021Document28 pagesSieo Irizarry2021Luluil MunirohNo ratings yet
- Rosenbloom 2013Document4 pagesRosenbloom 2013Imam SabarudinNo ratings yet
- Carbamazepine For Acute and Chronic Pain in AdultsDocument3 pagesCarbamazepine For Acute and Chronic Pain in AdultsGading AuroraNo ratings yet
- Pneumonia in The Immunocompetent Child ETDocument32 pagesPneumonia in The Immunocompetent Child ETVianney OlveraNo ratings yet
- Journal of Clinical Anesthesia: Original ContributionDocument6 pagesJournal of Clinical Anesthesia: Original ContributionzaimmuhtarNo ratings yet
- Peds 2020-0586Document16 pagesPeds 2020-0586Emilio Emmanué Escobar CruzNo ratings yet
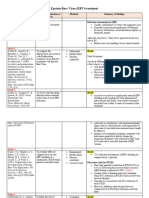
- Epstein-Barr Virus (EBV) Treatment: Study - Authors & Date Purpose of Evaluation or Research Methods Summary of FindingsDocument3 pagesEpstein-Barr Virus (EBV) Treatment: Study - Authors & Date Purpose of Evaluation or Research Methods Summary of Findingsapi-719803017No ratings yet
- Spinal Anaesthesia For Ambulatory Arthroscopic Surgery of The KneeDocument6 pagesSpinal Anaesthesia For Ambulatory Arthroscopic Surgery of The KneeGustavo MosqueraNo ratings yet
- Original Article: Banu HB, Rahman S, Hossain S, Nessa J, Khan EH, Mahmood K, Rahman DML, Ahmed MDocument6 pagesOriginal Article: Banu HB, Rahman S, Hossain S, Nessa J, Khan EH, Mahmood K, Rahman DML, Ahmed MDicky HaryantoNo ratings yet
- Comparison of The Efficacy of Combination Therapy of Prednisolone - Acyclovir With Prednisolone Alone in Bell's PalsyDocument30 pagesComparison of The Efficacy of Combination Therapy of Prednisolone - Acyclovir With Prednisolone Alone in Bell's PalsyAvindhaNo ratings yet
- E46 FullDocument9 pagesE46 Fulljames.armstrong35No ratings yet
- 21ST Lit WorksheetsDocument21 pages21ST Lit WorksheetsRea BartolomeNo ratings yet
- DISTRIBUTION STATEMENT A: Approved For Public Release Distribution Is UnlimitedDocument189 pagesDISTRIBUTION STATEMENT A: Approved For Public Release Distribution Is UnlimitedStein Hjalmar Hansen100% (1)
- Hospital Management & Information System: S SkiesDocument2 pagesHospital Management & Information System: S SkiesHandi FerryandiNo ratings yet
- DocumentDocument9 pagesDocumentpuskesmas ciapusNo ratings yet
- Mosaic TRD1 U2 VideoDocument1 pageMosaic TRD1 U2 VideomariaNo ratings yet
- Digital Principles UNIT 1 FinalDocument86 pagesDigital Principles UNIT 1 FinalSathish Kumar0% (1)
- Table of Contents - FinalDocument9 pagesTable of Contents - FinalkathleenNo ratings yet
- Lesson 11: Stakeholder Theory: A Comprehensive Approach To Corporate Social ResponsibilityDocument17 pagesLesson 11: Stakeholder Theory: A Comprehensive Approach To Corporate Social ResponsibilityMerlanie MaganaNo ratings yet
- Woldia University - 3 Year Cs Section 1 Group 5Document85 pagesWoldia University - 3 Year Cs Section 1 Group 5Yitayal GebruNo ratings yet
- Lines and AnglesDocument2 pagesLines and AnglesKaonashiNo ratings yet
- Adultery On The Part of The Wife - Desertion On The Part of The Husband - Loss of Affection - Cruelty - Insanity - ChildlessnessDocument2 pagesAdultery On The Part of The Wife - Desertion On The Part of The Husband - Loss of Affection - Cruelty - Insanity - ChildlessnesschiaocoNo ratings yet
- Abstinence in ReligionDocument3 pagesAbstinence in ReligionnieotyagiNo ratings yet
- Medical Terminology A Short Course 7th Edition Chabner Test BankDocument25 pagesMedical Terminology A Short Course 7th Edition Chabner Test BankKatherineMooretfqm100% (58)
- Hsse Department: (Solar Alert SDN BHD)Document2 pagesHsse Department: (Solar Alert SDN BHD)syafiq firdausNo ratings yet
- Art App HandoutDocument14 pagesArt App HandoutMarphil Rey TardioNo ratings yet
- Delhi Domestic Working Womens Forum Vs Union of Ins950517COM455916Document6 pagesDelhi Domestic Working Womens Forum Vs Union of Ins950517COM455916Bleach Body BoiNo ratings yet
- Synthesis of Tert-Butyl ChlorideDocument4 pagesSynthesis of Tert-Butyl ChlorideJoel AtienzaNo ratings yet
- (17 December 2014) Revised SC Draft Resolution-For CirculationDocument4 pages(17 December 2014) Revised SC Draft Resolution-For CirculationColum LynchNo ratings yet
- Periodic Assignment 1 Fall 21 201 B-1Document1 pagePeriodic Assignment 1 Fall 21 201 B-1Patrick MillerNo ratings yet
- Passivation On Chemical TankerDocument15 pagesPassivation On Chemical TankerRonald MesinaNo ratings yet
- Lutheran Social Service of MN - Chief Development OfficerDocument7 pagesLutheran Social Service of MN - Chief Development OfficerLars LeafbladNo ratings yet
- Hrdp-Shehla Zia & Ors V WAPDA (1994)Document6 pagesHrdp-Shehla Zia & Ors V WAPDA (1994)Robert WalusimbiNo ratings yet
- S01 Management and OrganizationDocument4 pagesS01 Management and OrganizationmijacajoNo ratings yet
- Rosa Interview Acta SociologicaDocument21 pagesRosa Interview Acta SociologicaDanielNo ratings yet
- United States v. Donald Eugene Johnson, 966 F.2d 1445, 4th Cir. (1992)Document6 pagesUnited States v. Donald Eugene Johnson, 966 F.2d 1445, 4th Cir. (1992)Scribd Government DocsNo ratings yet
- CASE DIGEST: Roque vs. IACDocument3 pagesCASE DIGEST: Roque vs. IACMichael Joseph NogoyNo ratings yet
- Ultrasound in Contemporary Physiotherapy PracticeDocument9 pagesUltrasound in Contemporary Physiotherapy Practicekinesiologíau0% (1)
- Course Syllabus TTL2 ScienceDocument8 pagesCourse Syllabus TTL2 ScienceMelan Joy Dela Cruz100% (1)





































![[The Journal of Emergency Medicine 2011-jun vol. 40 iss. 6] Anna Engeln - Cardiopulmonary Resuscitation Outcome of Out-of-hospital Cardiac Arrest in Low-volume versus High-volume Emergency Departments_ (2011) [10.1016_j.](https://imgv2-2-f.scribdassets.com/img/document/749360456/149x198/6a6749084c/1720609855?v=1)


















































Download as pdf or txt
You might also like
- Laporan Praktikum Evidence Based Medicine (EBM)Document13 pagesLaporan Praktikum Evidence Based Medicine (EBM)LalaNo ratings yet
- International Conference Vote of ThanksDocument1 pageInternational Conference Vote of ThanksRini Kaithamangalam Abraham85% (13)
- Challenges of OBDocument10 pagesChallenges of OBGeetanjali Soni 1937629No ratings yet
- PDF BelpalsyDocument4 pagesPDF Belpalsygoche29No ratings yet
- Hirano 1999Document7 pagesHirano 1999LitaDwiNo ratings yet
- Comparison Between The Efficacy of Steroids and Acyclovir in The Management of Patients With Bells PalsyDocument5 pagesComparison Between The Efficacy of Steroids and Acyclovir in The Management of Patients With Bells PalsyucenucenNo ratings yet
- An Evidence-Based Approach To The First SeizureDocument8 pagesAn Evidence-Based Approach To The First SeizureheribertoNo ratings yet
- Methods: Jeremy M. Hernandez, MD, PHD Jonathan Sherbino, MD, Med Data SourcesDocument2 pagesMethods: Jeremy M. Hernandez, MD, PHD Jonathan Sherbino, MD, Med Data SourcesabbbabbbNo ratings yet
- Papel de La Estimulación Eléctrica Añadida A La Terapia Convencional en Pacientes Con Parálisis Facial (De Campana) IdiopáticaDocument7 pagesPapel de La Estimulación Eléctrica Añadida A La Terapia Convencional en Pacientes Con Parálisis Facial (De Campana) IdiopáticaandresNo ratings yet
- The Efficacy of Acupuncture in The Treatment of Bell's Palsy SequelaeDocument11 pagesThe Efficacy of Acupuncture in The Treatment of Bell's Palsy Sequelaeseptiani hasibuanNo ratings yet
- The Effect of Prednisolone On Sequelae in Bell's PalsyDocument5 pagesThe Effect of Prednisolone On Sequelae in Bell's Palsyrara fifiNo ratings yet
- Comparison of Outcomes of The Epley and Self-Epley Maneuvers inDocument5 pagesComparison of Outcomes of The Epley and Self-Epley Maneuvers inYunie ArmyatiNo ratings yet
- A Comparison of Oral Procaterol and Albuterol in Reversible Airflow ObstructionDocument6 pagesA Comparison of Oral Procaterol and Albuterol in Reversible Airflow Obstructionparris shanyNo ratings yet
- Neurology Journal WNLDocument7 pagesNeurology Journal WNLDokter KarisNo ratings yet
- PotasiumDocument11 pagesPotasiumDesy YeyenNo ratings yet
- CD001869 AbstractDocument4 pagesCD001869 AbstractMarsya Yulinesia LoppiesNo ratings yet
- Exercise Recommendations in PatientsDocument4 pagesExercise Recommendations in PatientsAleCsss123No ratings yet
- Bells PalsyDocument9 pagesBells PalsysasoyNo ratings yet
- Pulsed Radiofrequency ofDocument8 pagesPulsed Radiofrequency ofDiego Pinto PatroniNo ratings yet
- Evidence Based Medicine - CONSORT & AppraisalDocument52 pagesEvidence Based Medicine - CONSORT & AppraisalNurul Aulia AbdullahNo ratings yet
- NLR Bells PalsyDocument4 pagesNLR Bells PalsyIskandar HasanNo ratings yet
- Isopropyl Alcohol Nasal Inhalation For Nausea in The Emergency Department: A Randomized Controlled TrialDocument10 pagesIsopropyl Alcohol Nasal Inhalation For Nausea in The Emergency Department: A Randomized Controlled TrialNagib MuhammadNo ratings yet
- Anorexia 1Document4 pagesAnorexia 1Antonio Gil EscalanteNo ratings yet
- Etr80003 994 995Document2 pagesEtr80003 994 995Karen Mae PadillaNo ratings yet
- The Efficacy of Acupuncture in The Treatment of Bell's Palsy SequelaeDocument9 pagesThe Efficacy of Acupuncture in The Treatment of Bell's Palsy SequelaerezteevicNo ratings yet
- Factors Associated With Fast Recovery of Bell Palsy in ChildrenDocument6 pagesFactors Associated With Fast Recovery of Bell Palsy in ChildrenPutri GintingNo ratings yet
- Comparison of Conservative Therapy and Steroid Therapy For Bell's Palsy in ChildrenDocument6 pagesComparison of Conservative Therapy and Steroid Therapy For Bell's Palsy in ChildrenyogihermawanNo ratings yet
- Manoeuvres For The Treatment of Benign Positional Paroxysmal Vertigo A Systematic ReviewDocument9 pagesManoeuvres For The Treatment of Benign Positional Paroxysmal Vertigo A Systematic ReviewShresthaNo ratings yet
- Artikel RCTDocument8 pagesArtikel RCTSALSABILA PUTRI AULIANo ratings yet
- Nihms 562917Document9 pagesNihms 562917Vincent LivandyNo ratings yet
- Literature Review of Bells PalsyDocument5 pagesLiterature Review of Bells Palsyafmzxppzpvoluf100% (1)
- 658 PDFDocument6 pages658 PDFismail39 orthoNo ratings yet
- Steroids: The Clinical Problem of Bell's Palsy: Treatment Effective?Document5 pagesSteroids: The Clinical Problem of Bell's Palsy: Treatment Effective?putriseptinaNo ratings yet
- Treatments For Bronchiolitis in Children Do Not Seem Review: Commonly Used PharmacologicalDocument2 pagesTreatments For Bronchiolitis in Children Do Not Seem Review: Commonly Used Pharmacologicalapi-3711135No ratings yet
- 2008 Physical Therapy For Bell's Palsy (Idiopathic Facial Paralysis) (Review)Document24 pages2008 Physical Therapy For Bell's Palsy (Idiopathic Facial Paralysis) (Review)Francisco Antonó Castro WeithNo ratings yet
- Derry, Sheena Et Al 2014 Single Dose Dipyrone For Acute Postoperative PainDocument48 pagesDerry, Sheena Et Al 2014 Single Dose Dipyrone For Acute Postoperative PainlilingNo ratings yet
- Tecer 2004 Audiovestibular Functioning in Patients With Panic DisorderDocument6 pagesTecer 2004 Audiovestibular Functioning in Patients With Panic DisorderJuan Hernández GarcíaNo ratings yet
- [The Journal of Emergency Medicine 2011-jun vol. 40 iss. 6] Anna Engeln - Cardiopulmonary Resuscitation Outcome of Out-of-hospital Cardiac Arrest in Low-volume versus High-volume Emergency Departments_ (2011) [10.1016_j.Document1 page[The Journal of Emergency Medicine 2011-jun vol. 40 iss. 6] Anna Engeln - Cardiopulmonary Resuscitation Outcome of Out-of-hospital Cardiac Arrest in Low-volume versus High-volume Emergency Departments_ (2011) [10.1016_j.royhiranmay94No ratings yet
- IVIgG AmiloidDocument4 pagesIVIgG AmiloidyinvilllNo ratings yet
- Prednisolone or Acyclovir in Bell's Palsy: CorrespondenceDocument2 pagesPrednisolone or Acyclovir in Bell's Palsy: CorrespondenceSukhvinder Singh RanaNo ratings yet
- Art. - Qual - of Life AsthmaDocument6 pagesArt. - Qual - of Life AsthmaMaria MariaNo ratings yet
- Vit B12Document6 pagesVit B12Winda PradnyaNo ratings yet
- CorrespondenceDocument3 pagesCorrespondenceFayza RihastaraNo ratings yet
- The Natural History of Epilepsy: An Epidemiological View: ReviewDocument6 pagesThe Natural History of Epilepsy: An Epidemiological View: ReviewDiana LeonNo ratings yet
- Online Reference Notes - Nursing Research Drill AnswerDocument17 pagesOnline Reference Notes - Nursing Research Drill AnswerDairyl TagaroNo ratings yet
- The Recent History of AcupunctureDocument2 pagesThe Recent History of AcupunctureBhaskaranNo ratings yet
- 1 s2.0 S0002838X23001041Document2 pages1 s2.0 S0002838X23001041Võ Văn Phúc ToànNo ratings yet
- Summary Proceedings From The Neurology Group On Neonatal SeizuresDocument7 pagesSummary Proceedings From The Neurology Group On Neonatal SeizuresTran Trang AnhNo ratings yet
- Nested Case-Control Study of Children Presenting WDocument6 pagesNested Case-Control Study of Children Presenting Wbilal hadiNo ratings yet
- OutDocument5 pagesOutFayza RihastaraNo ratings yet
- Sieo Irizarry2021Document28 pagesSieo Irizarry2021Luluil MunirohNo ratings yet
- Rosenbloom 2013Document4 pagesRosenbloom 2013Imam SabarudinNo ratings yet
- Carbamazepine For Acute and Chronic Pain in AdultsDocument3 pagesCarbamazepine For Acute and Chronic Pain in AdultsGading AuroraNo ratings yet
- Pneumonia in The Immunocompetent Child ETDocument32 pagesPneumonia in The Immunocompetent Child ETVianney OlveraNo ratings yet
- Journal of Clinical Anesthesia: Original ContributionDocument6 pagesJournal of Clinical Anesthesia: Original ContributionzaimmuhtarNo ratings yet
- Peds 2020-0586Document16 pagesPeds 2020-0586Emilio Emmanué Escobar CruzNo ratings yet
- Epstein-Barr Virus (EBV) Treatment: Study - Authors & Date Purpose of Evaluation or Research Methods Summary of FindingsDocument3 pagesEpstein-Barr Virus (EBV) Treatment: Study - Authors & Date Purpose of Evaluation or Research Methods Summary of Findingsapi-719803017No ratings yet
- Spinal Anaesthesia For Ambulatory Arthroscopic Surgery of The KneeDocument6 pagesSpinal Anaesthesia For Ambulatory Arthroscopic Surgery of The KneeGustavo MosqueraNo ratings yet
- Original Article: Banu HB, Rahman S, Hossain S, Nessa J, Khan EH, Mahmood K, Rahman DML, Ahmed MDocument6 pagesOriginal Article: Banu HB, Rahman S, Hossain S, Nessa J, Khan EH, Mahmood K, Rahman DML, Ahmed MDicky HaryantoNo ratings yet
- Comparison of The Efficacy of Combination Therapy of Prednisolone - Acyclovir With Prednisolone Alone in Bell's PalsyDocument30 pagesComparison of The Efficacy of Combination Therapy of Prednisolone - Acyclovir With Prednisolone Alone in Bell's PalsyAvindhaNo ratings yet
- E46 FullDocument9 pagesE46 Fulljames.armstrong35No ratings yet
- 21ST Lit WorksheetsDocument21 pages21ST Lit WorksheetsRea BartolomeNo ratings yet
- DISTRIBUTION STATEMENT A: Approved For Public Release Distribution Is UnlimitedDocument189 pagesDISTRIBUTION STATEMENT A: Approved For Public Release Distribution Is UnlimitedStein Hjalmar Hansen100% (1)
- Hospital Management & Information System: S SkiesDocument2 pagesHospital Management & Information System: S SkiesHandi FerryandiNo ratings yet
- DocumentDocument9 pagesDocumentpuskesmas ciapusNo ratings yet
- Mosaic TRD1 U2 VideoDocument1 pageMosaic TRD1 U2 VideomariaNo ratings yet
- Digital Principles UNIT 1 FinalDocument86 pagesDigital Principles UNIT 1 FinalSathish Kumar0% (1)
- Table of Contents - FinalDocument9 pagesTable of Contents - FinalkathleenNo ratings yet
- Lesson 11: Stakeholder Theory: A Comprehensive Approach To Corporate Social ResponsibilityDocument17 pagesLesson 11: Stakeholder Theory: A Comprehensive Approach To Corporate Social ResponsibilityMerlanie MaganaNo ratings yet
- Woldia University - 3 Year Cs Section 1 Group 5Document85 pagesWoldia University - 3 Year Cs Section 1 Group 5Yitayal GebruNo ratings yet
- Lines and AnglesDocument2 pagesLines and AnglesKaonashiNo ratings yet
- Adultery On The Part of The Wife - Desertion On The Part of The Husband - Loss of Affection - Cruelty - Insanity - ChildlessnessDocument2 pagesAdultery On The Part of The Wife - Desertion On The Part of The Husband - Loss of Affection - Cruelty - Insanity - ChildlessnesschiaocoNo ratings yet
- Abstinence in ReligionDocument3 pagesAbstinence in ReligionnieotyagiNo ratings yet
- Medical Terminology A Short Course 7th Edition Chabner Test BankDocument25 pagesMedical Terminology A Short Course 7th Edition Chabner Test BankKatherineMooretfqm100% (58)
- Hsse Department: (Solar Alert SDN BHD)Document2 pagesHsse Department: (Solar Alert SDN BHD)syafiq firdausNo ratings yet
- Art App HandoutDocument14 pagesArt App HandoutMarphil Rey TardioNo ratings yet
- Delhi Domestic Working Womens Forum Vs Union of Ins950517COM455916Document6 pagesDelhi Domestic Working Womens Forum Vs Union of Ins950517COM455916Bleach Body BoiNo ratings yet
- Synthesis of Tert-Butyl ChlorideDocument4 pagesSynthesis of Tert-Butyl ChlorideJoel AtienzaNo ratings yet
- (17 December 2014) Revised SC Draft Resolution-For CirculationDocument4 pages(17 December 2014) Revised SC Draft Resolution-For CirculationColum LynchNo ratings yet
- Periodic Assignment 1 Fall 21 201 B-1Document1 pagePeriodic Assignment 1 Fall 21 201 B-1Patrick MillerNo ratings yet
- Passivation On Chemical TankerDocument15 pagesPassivation On Chemical TankerRonald MesinaNo ratings yet
- Lutheran Social Service of MN - Chief Development OfficerDocument7 pagesLutheran Social Service of MN - Chief Development OfficerLars LeafbladNo ratings yet
- Hrdp-Shehla Zia & Ors V WAPDA (1994)Document6 pagesHrdp-Shehla Zia & Ors V WAPDA (1994)Robert WalusimbiNo ratings yet
- S01 Management and OrganizationDocument4 pagesS01 Management and OrganizationmijacajoNo ratings yet
- Rosa Interview Acta SociologicaDocument21 pagesRosa Interview Acta SociologicaDanielNo ratings yet
- United States v. Donald Eugene Johnson, 966 F.2d 1445, 4th Cir. (1992)Document6 pagesUnited States v. Donald Eugene Johnson, 966 F.2d 1445, 4th Cir. (1992)Scribd Government DocsNo ratings yet
- CASE DIGEST: Roque vs. IACDocument3 pagesCASE DIGEST: Roque vs. IACMichael Joseph NogoyNo ratings yet
- Ultrasound in Contemporary Physiotherapy PracticeDocument9 pagesUltrasound in Contemporary Physiotherapy Practicekinesiologíau0% (1)
- Course Syllabus TTL2 ScienceDocument8 pagesCourse Syllabus TTL2 ScienceMelan Joy Dela Cruz100% (1)