Download as xls, pdf, or txt
You might also like
- Fuel Bill FormatDocument1 pageFuel Bill Formatbhartiyaanuj100% (2)
- All PharmacyDocument16 pagesAll PharmacyBilling FOPJHRCNo ratings yet
- Electric BillDocument1 pageElectric BillImran HossainNo ratings yet
- Electricity Bill ReceiptDocument1 pageElectricity Bill ReceiptPranit shrivastavaNo ratings yet
- Tata Memorial Hospital-Electronic Medical Record REMARKSDocument2 pagesTata Memorial Hospital-Electronic Medical Record REMARKSSATISH KUMARNo ratings yet
- Medical Reimbursement (Supported by Bills) Hrms Application ParticularsDocument3 pagesMedical Reimbursement (Supported by Bills) Hrms Application ParticularsKarthikeyan GuruNo ratings yet
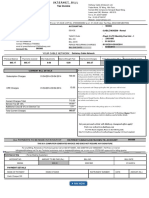
- Internet Bill FormatpdfDocument1 pageInternet Bill FormatpdfAdvaith KumarNo ratings yet
- Hospital Bill ReceiptDocument2 pagesHospital Bill Receiptakhil kottedi100% (1)
- Summary Account Payable Statement: (I) Platform Services Amount ( ) Invoice Number ParticularsDocument9 pagesSummary Account Payable Statement: (I) Platform Services Amount ( ) Invoice Number Particularsgsreddy6006No ratings yet
- Mobile Services: Your Account Summary This Month'S ChargesDocument5 pagesMobile Services: Your Account Summary This Month'S ChargesvijaykumarzNo ratings yet
- Interim Inpatient Bill (Summary)Document2 pagesInterim Inpatient Bill (Summary)Sairishi GhoshNo ratings yet
- Manayu Hospital, Rajura: Ipd BillDocument7 pagesManayu Hospital, Rajura: Ipd BillYatharth KatwareNo ratings yet
- Medicine BillDocument4 pagesMedicine BillRahul OmarNo ratings yet
- Real Medical Bill ScanDocument1 pageReal Medical Bill Scanmiranda criggerNo ratings yet
- Jiofiber Postpaid Bill FormatDocument10 pagesJiofiber Postpaid Bill Formatsystemwindows6432No ratings yet
- Payment Receipt: Fast Auto and Payday Loans, Inc. D/b/a Cash CowDocument1 pagePayment Receipt: Fast Auto and Payday Loans, Inc. D/b/a Cash CowKevin ChownsNo ratings yet
- Summary Bill FormatDocument1 pageSummary Bill FormatAmanNo ratings yet
- Due Date Telephone Number Amount Payable: Nwzamdvu Ewëh Eh Ma Ewëh DV© - MZ Ewëh (DdauDocument3 pagesDue Date Telephone Number Amount Payable: Nwzamdvu Ewëh Eh Ma Ewëh DV© - MZ Ewëh (DdauMohit DasNo ratings yet
- Movers and Packers Bill ReceiptDocument12 pagesMovers and Packers Bill ReceiptGaurav ChoudharyNo ratings yet
- Print Dup Bill 1Document1 pagePrint Dup Bill 1munibphotocopierNo ratings yet
- Hospital Bill 1Document2 pagesHospital Bill 1Süññy MäñèNo ratings yet
- Medical Bill - PDFDocument12 pagesMedical Bill - PDFSandeep SandyNo ratings yet
- Shri Krishna Meddicos: Shop No.159, Municpal Market, Murhtal Road, SonepatDocument4 pagesShri Krishna Meddicos: Shop No.159, Municpal Market, Murhtal Road, SonepatRaviArryanNo ratings yet
- Biswas Book Stores: Cash MemoDocument7 pagesBiswas Book Stores: Cash Memodeepak100% (1)
- Hotel Bill FormatDocument1 pageHotel Bill FormatDipesh YogiNo ratings yet
- Concorde Billing May 1-8, 2011Document33 pagesConcorde Billing May 1-8, 2011Rhoda PasardozaNo ratings yet
- Medical Bill1 PDFDocument1 pageMedical Bill1 PDFRahul KumarNo ratings yet
- Vehicle Insurance Policy FormatDocument2 pagesVehicle Insurance Policy FormatKannakiNo ratings yet
- Medical Bill Receipt: Patient InformationDocument1 pageMedical Bill Receipt: Patient InformationTolaNo ratings yet
- Property Tax Payment ReceiptDocument1 pageProperty Tax Payment Receiptyogi xeroxNo ratings yet
- Billed To: Date: Method: Receipt #: Invoice #Document1 pageBilled To: Date: Method: Receipt #: Invoice #michael PeacheyNo ratings yet
- Online Payment Receipt: Applicant DetailsDocument1 pageOnline Payment Receipt: Applicant Detailsprasanna malasheNo ratings yet
- Domestic: SMT Supriya ChowdhuryDocument2 pagesDomestic: SMT Supriya ChowdhurySujay HalderNo ratings yet
- Internet BillsDocument2 pagesInternet Billsrajal_995483669No ratings yet
- Hotel Bill FormatDocument1 pageHotel Bill FormatYeshu RathnamNo ratings yet
- Medical Invoice FinalDocument1 pageMedical Invoice FinalFaraz SahiNo ratings yet
- Hotel Bill Format in ExcelDocument1 pageHotel Bill Format in ExcelArsh SinhaNo ratings yet
- Summary Account Payable Statement: JiopayDocument1 pageSummary Account Payable Statement: JiopayhazihappyNo ratings yet
- Ishan Netsol Private Limited: Tax InvoiceDocument2 pagesIshan Netsol Private Limited: Tax InvoiceSunil Patel100% (1)
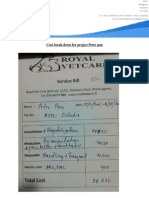
- Cost Break Down For Peter Pan, Marvricks 2 and Six SterlizationsDocument12 pagesCost Break Down For Peter Pan, Marvricks 2 and Six SterlizationsAdopt a Dog in Sri Lanka100% (1)
- Rent Receipt: (Signature)Document1 pageRent Receipt: (Signature)Akhil RaviNo ratings yet
- Invoice - Payment PrintDocument2 pagesInvoice - Payment PrintJithuJohnNo ratings yet
- Wire Request FormDocument3 pagesWire Request Formkhushbu25No ratings yet
- NBPDCL Bill FormatDocument1 pageNBPDCL Bill FormatASHUTOSH RANJANNo ratings yet
- The Billing Mechanism Has Been Revised So That The Benefit of One Previous / Preceeding Slab Is Available To Domestic Consumers (Residential User)Document1 pageThe Billing Mechanism Has Been Revised So That The Benefit of One Previous / Preceeding Slab Is Available To Domestic Consumers (Residential User)babarali3991No ratings yet
- Anuj File PDFDocument1 pageAnuj File PDFanuj thakurNo ratings yet
- For Billing Enquiry Visit Https://selfcare - Tikona.inDocument2 pagesFor Billing Enquiry Visit Https://selfcare - Tikona.inJatin BindalNo ratings yet
- Tax CorporationDocument1 pageTax CorporationAngsuman SenguptaNo ratings yet
- Property Tax Receipt - 2022Document1 pageProperty Tax Receipt - 2022Bablu DexterNo ratings yet
- Fixedline and Broadband Services Tax Invoice: Telephone Number 01149092480 User Id 01191365977 - DSLDocument2 pagesFixedline and Broadband Services Tax Invoice: Telephone Number 01149092480 User Id 01191365977 - DSLAnonymous L6LG6CTFpNo ratings yet
- Invoice: Ashirwad Hospital & PolyclinicDocument1 pageInvoice: Ashirwad Hospital & PolyclinicranjitNo ratings yet
- My Post Paid Bill SepDocument3 pagesMy Post Paid Bill SepSelvaraj ArunachalamNo ratings yet
- Bill (Horming Hospital)Document64 pagesBill (Horming Hospital)paras rahangdaleNo ratings yet
- Donation Receipt From (Type Organization Name) : Thank You For Your Generosity. We Appreciate Your Support!Document4 pagesDonation Receipt From (Type Organization Name) : Thank You For Your Generosity. We Appreciate Your Support!ipasetiNo ratings yet
- Tax Invoice: Billing Address Installation Address Invoice DetailsDocument1 pageTax Invoice: Billing Address Installation Address Invoice DetailsaffanNo ratings yet
- Tax Bill 2022Document1 pageTax Bill 2022LOUNGE HOMENo ratings yet
- Blank Petrol Bill ReceiptDocument12 pagesBlank Petrol Bill ReceiptSASI KUMARNo ratings yet
- Rosemarie Postpaid BillDocument1 pageRosemarie Postpaid BillGodlyn LitanaNo ratings yet
- Methods to Overcome the Financial and Money Transfer Blockade against Palestine and any Country Suffering from Financial BlockadeFrom EverandMethods to Overcome the Financial and Money Transfer Blockade against Palestine and any Country Suffering from Financial BlockadeNo ratings yet