Download as pdf or txt
You might also like
- 1485 Digital Breast TomosynthesisDocument156 pages1485 Digital Breast TomosynthesisWinston Mauricio Casco SobalvarroNo ratings yet
- Goodbye Parkinsons, Hello Life SampleDocument37 pagesGoodbye Parkinsons, Hello Life SampleMichael Wiese Productions100% (8)
- Liver Function TestsDocument4 pagesLiver Function TestsAnbaraj ArunNo ratings yet
- Voxyvi A System For Long-Term Audio and Video Acquisitions in NeonatalDocument15 pagesVoxyvi A System For Long-Term Audio and Video Acquisitions in NeonatalSuvarn SrivatsaNo ratings yet
- Ecr2017 C-2712Document14 pagesEcr2017 C-2712regarskidNo ratings yet
- (Download PDF) Diffusion Weighted Imaging of The Hepatobiliary System Techniques and Clinical Applications Celso Matos Online Ebook All Chapter PDFDocument42 pages(Download PDF) Diffusion Weighted Imaging of The Hepatobiliary System Techniques and Clinical Applications Celso Matos Online Ebook All Chapter PDFeverett.carnes371100% (16)
- Jove 96 52238Document10 pagesJove 96 52238Saffa AzharaaniNo ratings yet
- Applied Sciences: Respiration Monitoring For Premature Neonates in NicuDocument11 pagesApplied Sciences: Respiration Monitoring For Premature Neonates in NicuNicole LantinNo ratings yet
- Radiation Exposure From CT in Early Childhood: A French Large-Scale Multicentre StudyDocument8 pagesRadiation Exposure From CT in Early Childhood: A French Large-Scale Multicentre StudyArizal FuadNo ratings yet
- MRI of Acute Osteomyelitis in Long Bones of Children: Pathophysiology StudyDocument7 pagesMRI of Acute Osteomyelitis in Long Bones of Children: Pathophysiology Studyilhamhamka12345No ratings yet
- A Survey On Neonatal Incubator Monitoring SystemDocument9 pagesA Survey On Neonatal Incubator Monitoring SystemCARLOS DANIEL YI VILLAMIZARNo ratings yet
- In Vivo Determination of Chewing Patterns Using FBG and Artificial Neural NetworksDocument4 pagesIn Vivo Determination of Chewing Patterns Using FBG and Artificial Neural NetworksDaniel Prado de CamposNo ratings yet
- Research Grant Sample Proposal and BudgetDocument11 pagesResearch Grant Sample Proposal and Budgetiseekknowledge12No ratings yet
- Functional Magnetic Resonance Urography in Infants: Feasibility of A Feed-And-Sleep TechniqueDocument7 pagesFunctional Magnetic Resonance Urography in Infants: Feasibility of A Feed-And-Sleep TechniqueCristian DemecoNo ratings yet
- 1 s2.0 S1059131120303162 MainDocument9 pages1 s2.0 S1059131120303162 MainInes Arias PazNo ratings yet
- Cranial Ultrasound Findings in Late Preterm Infants and Correlation With Perinatal Risk FactorsDocument7 pagesCranial Ultrasound Findings in Late Preterm Infants and Correlation With Perinatal Risk FactorsM Ibnu Rahman SyahNo ratings yet
- Pilot Study of A New Freely Available Computer Aided Polyp Detection System in Clinical PracticeDocument6 pagesPilot Study of A New Freely Available Computer Aided Polyp Detection System in Clinical PracticeJoel TroyaNo ratings yet
- Prenatal Diagnosis of Fetal Abdominal Cystic Masses: Can MR Change The Outcome?Document10 pagesPrenatal Diagnosis of Fetal Abdominal Cystic Masses: Can MR Change The Outcome?salahzotoNo ratings yet
- Real-Time Anomaly Detection in Surveillance Footage (Deliverable1)Document4 pagesReal-Time Anomaly Detection in Surveillance Footage (Deliverable1)Sadia ShafiqNo ratings yet
- Gambier2019 9Document8 pagesGambier2019 9Laura ImreNo ratings yet
- CNS Part 2 Targeted NeurosonographyDocument12 pagesCNS Part 2 Targeted NeurosonographyRicardo GuerreroNo ratings yet
- AET ConferrencThe Early Step of Healthiness Detection For Coral Quality of LifeeDocument6 pagesAET ConferrencThe Early Step of Healthiness Detection For Coral Quality of LifeeWahyu SesulihatienNo ratings yet
- 2D-3D Assessment of The Face, Cleft LipDocument10 pages2D-3D Assessment of The Face, Cleft LipginogjNo ratings yet
- TMP 6 D40Document11 pagesTMP 6 D40FrontiersNo ratings yet
- Analysis of Fetal Development Using Ultrasound Images: Shamya Shetty, Dr. Jose Alex MathewDocument7 pagesAnalysis of Fetal Development Using Ultrasound Images: Shamya Shetty, Dr. Jose Alex MathewIOSRjournalNo ratings yet
- Symposium Article: Imaging of A Child With PolytraumaDocument22 pagesSymposium Article: Imaging of A Child With PolytraumaAnonymous wdmpgxNo ratings yet
- Lorenz2009 Article Wide-fieldDigitalImagingBasedTDocument12 pagesLorenz2009 Article Wide-fieldDigitalImagingBasedTtecim3No ratings yet
- Clinical Study: Rehabilitation of Children With Hemiparesis: A Pilot Study On The Use of Virtual RealityDocument5 pagesClinical Study: Rehabilitation of Children With Hemiparesis: A Pilot Study On The Use of Virtual RealityAitana Castro BravoNo ratings yet
- CTG HaDocument15 pagesCTG HaNabila SaribanunNo ratings yet
- Fifteen Years Experience in Laparoscopic Inguinal Hernia Repair in Pediatric Patients. Results and Considerations On A Debated ProcedureDocument11 pagesFifteen Years Experience in Laparoscopic Inguinal Hernia Repair in Pediatric Patients. Results and Considerations On A Debated Procedurebendot29No ratings yet
- 0100 7203 Rbgo 37 04 00149Document3 pages0100 7203 Rbgo 37 04 00149marcosdabataNo ratings yet
- Fetal Intervetion - Abdelghaffarhelal2019Document20 pagesFetal Intervetion - Abdelghaffarhelal2019Trần Ngọc BíchNo ratings yet
- Local DRL and Organ Dose Pediatric Procedures (PCXMC)Document9 pagesLocal DRL and Organ Dose Pediatric Procedures (PCXMC)sebastian CarrascoNo ratings yet
- Anoplastia Percutanea 2022Document11 pagesAnoplastia Percutanea 2022Sandra Cárdenas HilasacaNo ratings yet
- Pelod 2Document14 pagesPelod 2gaatgaatNo ratings yet
- Example of SPMPDocument7 pagesExample of SPMPRoberto Julianto KondoruraNo ratings yet
- How to Perform Ultrasonography in EndometriosisFrom EverandHow to Perform Ultrasonography in EndometriosisStefano GuerrieroNo ratings yet
- Point-of-Care Thoracic Ultrasound in Children New Advances in Pediatric Emergency SettingDocument19 pagesPoint-of-Care Thoracic Ultrasound in Children New Advances in Pediatric Emergency SettingVeronica Romero MouthonNo ratings yet
- Children and Neonates Anesthesia in Magnetic Resonance Environment in Italy - BMC Anest22Document9 pagesChildren and Neonates Anesthesia in Magnetic Resonance Environment in Italy - BMC Anest22Gunther MirandaNo ratings yet
- Broncoscopia Cuando y CuantoDocument10 pagesBroncoscopia Cuando y CuantoiliseeNo ratings yet
- DL For LaparosDocument7 pagesDL For LaparosVainavi SamantNo ratings yet
- Neonatal Respiratory System Updates 2020Document824 pagesNeonatal Respiratory System Updates 2020link_wolfloboNo ratings yet
- Biomedical Signal Processing and Control: Lina Abou-Abbas, Hesam Fersaie Alaie, Chakib TadjDocument9 pagesBiomedical Signal Processing and Control: Lina Abou-Abbas, Hesam Fersaie Alaie, Chakib TadjnidhalNo ratings yet
- Azria 2016Document14 pagesAzria 2016Nour Saïd Nour NourNo ratings yet
- Tracking Organisms: Toxtrac: A Fast and Robust Software ForDocument72 pagesTracking Organisms: Toxtrac: A Fast and Robust Software ForRogério GerbatinNo ratings yet
- Journal of Biophotonics - 2014 - Caprio - Holographic Imaging of Unlabelled Sperm Cells For Semen Analysis A ReviewDocument11 pagesJournal of Biophotonics - 2014 - Caprio - Holographic Imaging of Unlabelled Sperm Cells For Semen Analysis A ReviewSergeNo ratings yet
- Near-Infrared Spectroscopy Measurements of Cerebral Oxygenation in Newborns During Immediate Postnatal AdaptationDocument6 pagesNear-Infrared Spectroscopy Measurements of Cerebral Oxygenation in Newborns During Immediate Postnatal Adaptationcodruta_holtzNo ratings yet
- 2014 - Maturation of The Middle Phalanx and CMV - Comperative Study - PerinettiDocument10 pages2014 - Maturation of The Middle Phalanx and CMV - Comperative Study - PerinettiSrdjan StojanovskiNo ratings yet
- Findlay Et Al 2020 Component Processes of Detection Probability in Camera Trap StudiesDocument14 pagesFindlay Et Al 2020 Component Processes of Detection Probability in Camera Trap StudiesFelipe Indo AriasNo ratings yet
- Smart Cradle ModuleDocument6 pagesSmart Cradle ModuletejaswiniNo ratings yet
- An Affordable Platform For Virtual Reality𠄽ocument9 pagesAn Affordable Platform For Virtual Reality𠄺hmedNo ratings yet
- Children: Perinatal Femoral Fracture: A Ten-Year Observational Case Series StudyDocument7 pagesChildren: Perinatal Femoral Fracture: A Ten-Year Observational Case Series StudyStella Gracia OctaricaNo ratings yet
- Acta Ophthalmologica - 2007 - Lavezzo - Eye Blink in Newborn and Preschool Age ChildrenDocument4 pagesActa Ophthalmologica - 2007 - Lavezzo - Eye Blink in Newborn and Preschool Age ChildrenKhairul HafizNo ratings yet
- Martinho2019 - Artigo Vaginal Childbirth Is The Primary Environmental Factor in TheDocument6 pagesMartinho2019 - Artigo Vaginal Childbirth Is The Primary Environmental Factor in TheGleiciane AguiarNo ratings yet
- Engel 2018Document11 pagesEngel 2018GonzaloNo ratings yet
- Automatic Posture and Movement Tracking of Infants With Wearable Movement SensorsDocument13 pagesAutomatic Posture and Movement Tracking of Infants With Wearable Movement SensorsEccoNo ratings yet
- Ecr2018 C-0537 PDFDocument37 pagesEcr2018 C-0537 PDFvivek kumarNo ratings yet
- Fnins 17 1155900Document19 pagesFnins 17 1155900Hoàng Huyền NhungNo ratings yet
- Point of Care Ultrasound For Non Vascular Invasive Procedures in Critically Ill Neonates and Children - Current Status and Future PerspectivesDocument9 pagesPoint of Care Ultrasound For Non Vascular Invasive Procedures in Critically Ill Neonates and Children - Current Status and Future PerspectivesVeronica Romero MouthonNo ratings yet
- Essential of Audiology: Screening and Post-ScreeningDocument3 pagesEssential of Audiology: Screening and Post-ScreeningBhisma D. SyaputraNo ratings yet
- Ni Hms 12505Document10 pagesNi Hms 12505noorhadi.n10No ratings yet
- Electronic Fetal MonitoringFrom EverandElectronic Fetal MonitoringXiaohui GuoNo ratings yet
- Design Ideas: Keyboard CircuitDocument2 pagesDesign Ideas: Keyboard CircuitTariq Zuhluf100% (3)
- E 05 B 040Document7 pagesE 05 B 040Tariq Zuhluf100% (2)
- Practical Neural Networks (3) : Part 3 - Feedback Nets and Competitive NetsDocument5 pagesPractical Neural Networks (3) : Part 3 - Feedback Nets and Competitive NetsTariq Zuhluf100% (2)
- Mains Voltage Monitor: Goswin VisschersDocument1 pageMains Voltage Monitor: Goswin VisschersTariq Zuhluf100% (2)
- E 055077Document1 pageE 055077Tariq ZuhlufNo ratings yet
- Psd3Xx Chips: by A. Riet JensDocument3 pagesPsd3Xx Chips: by A. Riet JensTariq Zuhluf100% (1)
- Ensors FOR Humans: Sensor Technology at MITDocument4 pagesEnsors FOR Humans: Sensor Technology at MITTariq ZuhlufNo ratings yet
- E 905030Document4 pagesE 905030Tariq ZuhlufNo ratings yet
- Slave Mains On-Off Control: Amplificationj Attenuation SelectorDocument3 pagesSlave Mains On-Off Control: Amplificationj Attenuation SelectorTariq Zuhluf100% (2)
- Universal Power-On Delay: by J. RuffellDocument1 pageUniversal Power-On Delay: by J. RuffellTariq Zuhluf100% (2)
- Seven-Eleven: Ir NVDocument3 pagesSeven-Eleven: Ir NVTariq Zuhluf100% (2)
- E 02 CH 04Document1 pageE 02 CH 04Tariq Zuhluf100% (2)
- Remote Control by Mobile Phone: Switch & Control Using DTMF SignallingDocument4 pagesRemote Control by Mobile Phone: Switch & Control Using DTMF SignallingTariq Zuhluf100% (2)
- Noise of The The V /115.: R.rn.sDocument1 pageNoise of The The V /115.: R.rn.sTariq Zuhluf100% (1)
- In Questof A PangramDocument5 pagesIn Questof A PangramTariq Zuhluf100% (1)
- Stereo Peak Indicator: Small CircuitscollectionDocument1 pageStereo Peak Indicator: Small CircuitscollectionTariq Zuhluf100% (1)
- Token Number Display: Small CircuitscollectionDocument1 pageToken Number Display: Small CircuitscollectionTariq Zuhluf100% (2)
- E 03 B 035Document1 pageE 03 B 035Tariq Zuhluf100% (1)
- Current Probe: Parts ListDocument1 pageCurrent Probe: Parts ListTariq Zuhluf100% (2)
- Speed-Up For Darlingtons: Small CircuitscollectionDocument1 pageSpeed-Up For Darlingtons: Small CircuitscollectionTariq Zuhluf100% (1)
- Wireless Museum: Components ListDocument1 pageWireless Museum: Components ListTariq Zuhluf100% (1)
- E05c070 PDFDocument4 pagesE05c070 PDFTariq Zuhluf100% (1)
- Electrical Isolation For I C Bus: National Semiconductor ApplicationDocument1 pageElectrical Isolation For I C Bus: National Semiconductor ApplicationTariq ZuhlufNo ratings yet
- The Miser'S T/R Loop Antenna: MiserlyDocument3 pagesThe Miser'S T/R Loop Antenna: MiserlyTariq ZuhlufNo ratings yet
- AT90S8535 Programmer: Suitable For In-System UseDocument3 pagesAT90S8535 Programmer: Suitable For In-System UseTariq ZuhlufNo ratings yet
- Idc To Box Header Adaptor: ReferenceDocument2 pagesIdc To Box Header Adaptor: ReferenceTariq Zuhluf100% (1)
- Valve Detector Receiver: Small CircuitscollectionDocument1 pageValve Detector Receiver: Small CircuitscollectionTariq ZuhlufNo ratings yet
- Mains Splitter For AF Power Amps: Elektor Electronics. A Copy ofDocument1 pageMains Splitter For AF Power Amps: Elektor Electronics. A Copy ofTariq ZuhlufNo ratings yet
- Advanced Stock Control and Kitting Program: EqwnsiveDocument2 pagesAdvanced Stock Control and Kitting Program: EqwnsiveTariq ZuhlufNo ratings yet
- Programing Tool For Attiny15: Small CircuitscollectionDocument2 pagesPrograming Tool For Attiny15: Small CircuitscollectionTariq ZuhlufNo ratings yet
- MRI of Enthesitis in As (Including PsA)Document7 pagesMRI of Enthesitis in As (Including PsA)wandering_bearNo ratings yet
- Home Care and Family PhysicianDocument25 pagesHome Care and Family PhysiciandesypermitasariNo ratings yet
- Questionnaire Survey of Working Relationships Between Nurses and Doctors in University Teaching Hospitals in Southern NigeriaDocument22 pagesQuestionnaire Survey of Working Relationships Between Nurses and Doctors in University Teaching Hospitals in Southern NigeriaMin MinNo ratings yet
- Laparoscopic CholecystectomyDocument41 pagesLaparoscopic CholecystectomyLim MelaniNo ratings yet
- San Juan de Dios Educational Foundation, IncDocument6 pagesSan Juan de Dios Educational Foundation, Incmae- athenaNo ratings yet
- Mandatory PhilHealth Coverage of Senior Citizens Pursuant To RA 10645 02.22.2015Document33 pagesMandatory PhilHealth Coverage of Senior Citizens Pursuant To RA 10645 02.22.2015Ralph Julius L. Mendoza100% (1)
- Case ReportDocument29 pagesCase Reportannisa hayatiNo ratings yet
- Presentation For Saksham Training - Basic Life SupportDocument51 pagesPresentation For Saksham Training - Basic Life SupportPotluri SunilNo ratings yet
- CBQDocument6 pagesCBQCarlos BaysaNo ratings yet
- Implementing AORN Recommended Practices For Surgical AttireDocument19 pagesImplementing AORN Recommended Practices For Surgical AttireKimberly Bundley-JohnsonNo ratings yet
- Disease EssayDocument5 pagesDisease Essayapi-309393081No ratings yet
- Automated External DefibrillatorDocument4 pagesAutomated External Defibrillatormelek saadiNo ratings yet
- ND - Disturbed Thought ProcessDocument2 pagesND - Disturbed Thought ProcessHu DawiNo ratings yet
- Mastitis and Urinary RetentionDocument8 pagesMastitis and Urinary RetentionNayacil LicayanNo ratings yet
- (Current Clinica (Current - Clinical - Strategies) - Gynecology - and - Obstetrics - 2004l Strategies) - Gynecology and Obstetrics 2004Document125 pages(Current Clinica (Current - Clinical - Strategies) - Gynecology - and - Obstetrics - 2004l Strategies) - Gynecology and Obstetrics 2004Eliza Stochita100% (1)
- Uterine AtonyDocument1 pageUterine AtonyYakumaNo ratings yet
- Buvanendran 2009 Acute-PainDocument2 pagesBuvanendran 2009 Acute-PainOmar BazalduaNo ratings yet
- Third Degree Block After Mi........ Observe The PatientDocument23 pagesThird Degree Block After Mi........ Observe The PatientSunn Ren TeeNo ratings yet
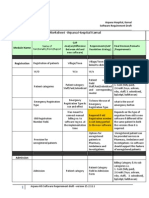
- Finalized Requirements-Worksheet - Arpana Hospital KarnalDocument11 pagesFinalized Requirements-Worksheet - Arpana Hospital KarnalMahesh PatilNo ratings yet
- Thyroid Disease Anesthetic ConsiderationsDocument30 pagesThyroid Disease Anesthetic Considerationssachin10dulkarNo ratings yet
- Observer Ship - Faraz Khan LuniDocument23 pagesObserver Ship - Faraz Khan LuniWaqas SaeedNo ratings yet
- Linking Dental With Medical Presentation by Dr. Carl Stoel DDSDocument44 pagesLinking Dental With Medical Presentation by Dr. Carl Stoel DDSShivendra Nath TripathiNo ratings yet
- NCLEX FundamentalsDocument13 pagesNCLEX FundamentalsSara Pirman100% (1)
- Ivf StudyDocument1 pageIvf StudyjeliinNo ratings yet
- Causes of Spontaneous Abortion 2Document23 pagesCauses of Spontaneous Abortion 2kenNo ratings yet
- Moisture-Associated Skin Damage (MASD) - Tear CollectionDocument14 pagesMoisture-Associated Skin Damage (MASD) - Tear CollectionIchigo RukiaNo ratings yet
- MBA HCS Project DownloadDocument2 pagesMBA HCS Project DownloadArvind K100% (1)
- The Body ElectricDocument335 pagesThe Body Electricsuper0sonicNo ratings yet