Download as pdf or txt
You might also like
- Flowers For Algernon by Daniel KeyesDocument59 pagesFlowers For Algernon by Daniel Keyesguelmeguelme100% (1)
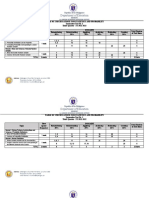
- Department of Education: Republic of The PhilippinesDocument6 pagesDepartment of Education: Republic of The PhilippinesAngel Guillermo Jr.100% (1)
- Text Book of Human ParasitologyDocument257 pagesText Book of Human ParasitologyKethlein Pearl Quiñonez100% (1)
- Zoonoses: Review ArticleDocument4 pagesZoonoses: Review ArticlerohishaakNo ratings yet
- Daszak 2000Document7 pagesDaszak 2000Alejandro Acuña MellaNo ratings yet
- Effects of Fungal InfectionsDocument3 pagesEffects of Fungal InfectionsAlexa BarniegoNo ratings yet
- Epidemiologi MyiasisDocument9 pagesEpidemiologi Myiasisrizky afiantiNo ratings yet
- Daszak Et Al - EID - Science 2000Document7 pagesDaszak Et Al - EID - Science 2000javenacostaNo ratings yet
- 1 - Helminths Infections - Introductory Notes - Importance of Studying HelminthsDocument11 pages1 - Helminths Infections - Introductory Notes - Importance of Studying HelminthsMuhammad KamranNo ratings yet
- Micoses Superficiais - GlobalDocument19 pagesMicoses Superficiais - GlobalJosé Paulo Ribeiro JúniorNo ratings yet
- MAROLI Et Al-2013-Medical and Veterinary EntomologyDocument25 pagesMAROLI Et Al-2013-Medical and Veterinary EntomologymclimacoNo ratings yet
- 2018 Febreamarela Trendsin EntomolingDocument9 pages2018 Febreamarela Trendsin EntomolingMárcius SilvaNo ratings yet
- Antifungal Activities of Selected MedicaDocument40 pagesAntifungal Activities of Selected Medicavalerybikobo588No ratings yet
- tmp63B0 TMPDocument15 pagestmp63B0 TMPFrontiersNo ratings yet
- Detection of Rodent-Borne Parasitic Pathogens of Wild Rats in Serdang, Selangor, Malaysia - A Potential Threat To Human HealthDocument9 pagesDetection of Rodent-Borne Parasitic Pathogens of Wild Rats in Serdang, Selangor, Malaysia - A Potential Threat To Human HealthMohd AriffNo ratings yet
- Vaccines 10 01385 With CoverDocument12 pagesVaccines 10 01385 With CoverDiana GonzalezNo ratings yet
- Kakhuangailiu GangmeiDocument10 pagesKakhuangailiu Gangmeizeyarag5608No ratings yet
- 06 Chapter 1Document46 pages06 Chapter 1Joscila OlfindoNo ratings yet
- Biological Control of Mosquitoes and Other Biting Files by Bacillus Sphaericus and Bacillus ThuringiensisDocument13 pagesBiological Control of Mosquitoes and Other Biting Files by Bacillus Sphaericus and Bacillus ThuringiensisMilena NovaNo ratings yet
- Othman 2014Document44 pagesOthman 2014Jessica QuevedoNo ratings yet
- Don Dorathy SEMINAR REVIEWDocument53 pagesDon Dorathy SEMINAR REVIEWUdofia JuniorNo ratings yet
- Research Paper On ZoonosesDocument8 pagesResearch Paper On Zoonosesaflbtvmfp100% (1)
- Henn Et Al 2008 Generating and Testing Molecular Hypotheses in The DermatophytesDocument8 pagesHenn Et Al 2008 Generating and Testing Molecular Hypotheses in The Dermatophytesnandaas887No ratings yet
- ADOLE M.SC FinalDocument61 pagesADOLE M.SC FinalTerna HonNo ratings yet
- Parasites: Christine A Northrop-Clewes and Christopher ShawDocument16 pagesParasites: Christine A Northrop-Clewes and Christopher ShawBouazzi IslemmNo ratings yet
- Artikel 3Document11 pagesArtikel 3Andini TalithaNo ratings yet
- Melgarejo-Colmenares2022 - Blood Feeding Habits of Mosquitoes Hardly A Bite in South AmericaDocument24 pagesMelgarejo-Colmenares2022 - Blood Feeding Habits of Mosquitoes Hardly A Bite in South AmericakevinNo ratings yet
- Bat Hunts and Disease OutbreaksDocument9 pagesBat Hunts and Disease OutbreaksDr V. Ramanathan, Assistant Professor Department of Chemistry, IIT (BHU), VaranasiNo ratings yet
- Public Health Pesticides: 4.1 IntroductionDocument26 pagesPublic Health Pesticides: 4.1 Introductionmecejo7728No ratings yet
- Abdul Project 2022 - 2Document35 pagesAbdul Project 2022 - 2Joseph TsokenNo ratings yet
- 1 s2.0 S0001706X22001309 MainDocument18 pages1 s2.0 S0001706X22001309 MainEstie KiriwennoNo ratings yet
- 1096-8644 (2000) 43 31+ 3 Aid-Ajpa2 3.0.co 2-ZDocument29 pages1096-8644 (2000) 43 31+ 3 Aid-Ajpa2 3.0.co 2-ZMaïga YoussouphNo ratings yet
- 1 PBDocument17 pages1 PBTércio MeloNo ratings yet
- The Problem and Its ScopeDocument4 pagesThe Problem and Its ScopeCJ ManlangitNo ratings yet
- Ecologia de Enfermedades Infecciosas EmergentesDocument14 pagesEcologia de Enfermedades Infecciosas EmergentesJONATHAN DAVID SANCHEZ RODRIGUEZNo ratings yet
- ZoonosisDocument3 pagesZoonosismeganursantoNo ratings yet
- 2018 Hyde WorldSTenMostFearedFungiDocument34 pages2018 Hyde WorldSTenMostFearedFungijScribdNo ratings yet
- 2003 - The Origin, Emergence and Evolutionary Genetics of Dengue VirusDocument10 pages2003 - The Origin, Emergence and Evolutionary Genetics of Dengue VirusAnglia LopesNo ratings yet
- The Role of Cockroaches and Flies in Mechanical Transmission of Medical Important Parasites PDFDocument7 pagesThe Role of Cockroaches and Flies in Mechanical Transmission of Medical Important Parasites PDFAaron YakubuNo ratings yet
- The Emergence of Arthropod-Borne Viral Diseases A Global Prospective On Dengue, Chikungunya and Zika FeversDocument23 pagesThe Emergence of Arthropod-Borne Viral Diseases A Global Prospective On Dengue, Chikungunya and Zika FeversdianamfgNo ratings yet
- The Prevalence of Soil Transmitted HelmiDocument7 pagesThe Prevalence of Soil Transmitted HelmilynneunlocksNo ratings yet
- 9e58 PDFDocument10 pages9e58 PDFcarlos javierNo ratings yet
- Wong Et Al. (2007)Document25 pagesWong Et Al. (2007)Sammer Cañesares BurgosNo ratings yet
- Arici BoliDocument18 pagesArici BolibedeliniNo ratings yet
- Soil-Transmitted Helminth Infections Lancet 2018Document14 pagesSoil-Transmitted Helminth Infections Lancet 2018cico3002No ratings yet
- Holland 2015-2017 PDFDocument14 pagesHolland 2015-2017 PDFGuadalupe Cristina Chuchón CáceresNo ratings yet
- River Continuum Concept - Vannote Et AlDocument29 pagesRiver Continuum Concept - Vannote Et Alshemar TrotmanNo ratings yet
- Chapter 1 Introduction 2019 Medical and Veterinary EntomologyDocument16 pagesChapter 1 Introduction 2019 Medical and Veterinary EntomologyLarisa PazNo ratings yet
- Morphological, Molecular, and Pathological Appraisal of Hymenolepis Nana (Hymenolepididae) Infecting Laboratory Mice (Mus Musculus)Document15 pagesMorphological, Molecular, and Pathological Appraisal of Hymenolepis Nana (Hymenolepididae) Infecting Laboratory Mice (Mus Musculus)Mery Nurun rNo ratings yet
- Tomassonne Et Al 2018Document10 pagesTomassonne Et Al 2018SoniaMaricelNo ratings yet
- He 2019Document20 pagesHe 2019mel93egNo ratings yet
- Review On Epidemiology and Pathology of Yellow Fever VirusDocument24 pagesReview On Epidemiology and Pathology of Yellow Fever Virushenok bushura100% (1)
- Molecules 22 00058Document41 pagesMolecules 22 00058Jordan MillerNo ratings yet
- Wild Great Apes As Sentinels and Sources of Infectious DiseaseDocument8 pagesWild Great Apes As Sentinels and Sources of Infectious Diseaseapi-286454950No ratings yet
- Tick-Borne Diseases in Turkey A Review One Health ApproachDocument12 pagesTick-Borne Diseases in Turkey A Review One Health ApproachAamir muse osmanNo ratings yet
- Research ProjectDocument55 pagesResearch ProjectOkwukwu ChrisNo ratings yet
- Plasmodium Genomics: An Approach For Learning About and Ending Human MalariaDocument27 pagesPlasmodium Genomics: An Approach For Learning About and Ending Human MalariaHatem EletrebyNo ratings yet
- WNOFNS 28 (2020) 34-50 (Might Be Useful)Document17 pagesWNOFNS 28 (2020) 34-50 (Might Be Useful)Shadows BlameNo ratings yet
- It's Not About the Bats: Conservation, the coronavirus and how we must re-set our relationship with natureFrom EverandIt's Not About the Bats: Conservation, the coronavirus and how we must re-set our relationship with natureNo ratings yet
- Ebola Virus Disease: A Manual for EVD ManagementFrom EverandEbola Virus Disease: A Manual for EVD ManagementMarta LadoNo ratings yet
- Pests and Pestilence: The Management of Invasive Species, Pests and Disease in New ZealandFrom EverandPests and Pestilence: The Management of Invasive Species, Pests and Disease in New ZealandNo ratings yet
- What on Earth Evolved? ... in Brief: 100 species that have changed the worldFrom EverandWhat on Earth Evolved? ... in Brief: 100 species that have changed the worldRating: 3 out of 5 stars3/5 (2)
- Open Pit Mine Planning With Blending ConstraintsDocument6 pagesOpen Pit Mine Planning With Blending ConstraintsJose GonzalesNo ratings yet
- In What Ways Is The Sorcerer and His Magic An Example of Structural AnthropologyDocument5 pagesIn What Ways Is The Sorcerer and His Magic An Example of Structural Anthropologyselina_kollsNo ratings yet
- SSCBS - FDPDocument7 pagesSSCBS - FDPkunalNo ratings yet
- COA - C97-003Revised Estimated Useful Life in Computing Depreciation For Government PropDocument5 pagesCOA - C97-003Revised Estimated Useful Life in Computing Depreciation For Government PropJonnel AcobaNo ratings yet
- Tillich, Paul - The Interpretation of History PDFDocument134 pagesTillich, Paul - The Interpretation of History PDFIvan HorvatNo ratings yet
- Cross Cultural AdvDocument15 pagesCross Cultural AdvSinita BasakNo ratings yet
- ARI - 820-2000 Ice Storage BinsDocument8 pagesARI - 820-2000 Ice Storage BinsHellenHoaNo ratings yet
- Npi PDFDocument23 pagesNpi PDFNatasya Juliani DodieNo ratings yet
- 8 IntelliJDocument7 pages8 IntelliJSuraj GhimireNo ratings yet
- Halgren - 2000 - Molecular Geometries and Vibrational Frequencies For MMFF94Document34 pagesHalgren - 2000 - Molecular Geometries and Vibrational Frequencies For MMFF94Fred KarlNo ratings yet
- K P Krishman S Astrology For Beginners Encyclopedia of Astrology Vol 1Document120 pagesK P Krishman S Astrology For Beginners Encyclopedia of Astrology Vol 1Satyabrata NayakNo ratings yet
- Introduction To ParabolaDocument5 pagesIntroduction To ParabolaMelvin EstoleroNo ratings yet
- Masbate BL Forms 1st BatchDocument18 pagesMasbate BL Forms 1st BatchLiezel NibresNo ratings yet
- Curriculum JD Sustainable DevelopmentDocument52 pagesCurriculum JD Sustainable DevelopmentAmruchanNo ratings yet
- Men of War Assault Squad2 Manual VIEWDocument20 pagesMen of War Assault Squad2 Manual VIEWtunimaoNo ratings yet
- Business Studies 2015 SamDocument7 pagesBusiness Studies 2015 SamBIKASH166No ratings yet
- 7.standard Adapter Framework Modules (AF - Modules) PDFDocument5 pages7.standard Adapter Framework Modules (AF - Modules) PDFankaiah_yadavNo ratings yet
- كيفية إدارة الاجتماعDocument27 pagesكيفية إدارة الاجتماعAlfa99kNo ratings yet
- Abhijeet K Sahu Product Design BIWDocument2 pagesAbhijeet K Sahu Product Design BIWabhie4u100% (1)
- Perkembangan Terakhir Serat Optik Di IndonesiaDocument14 pagesPerkembangan Terakhir Serat Optik Di IndonesiaAnis ZulaikahNo ratings yet
- Calculating Percent ErrorDocument9 pagesCalculating Percent ErrorMr. PetersonNo ratings yet
- Research Methods in Political ScienceDocument537 pagesResearch Methods in Political ScienceArtemusKonstantinPi100% (1)
- Philippians 4 13 - PPT DEFENSEDocument17 pagesPhilippians 4 13 - PPT DEFENSESherwina Marie del RosarioNo ratings yet
- ESpace U1910 Unified Gateway V100R001C01SPC600 Software Installation Guide 06Document79 pagesESpace U1910 Unified Gateway V100R001C01SPC600 Software Installation Guide 06Mostafa Gamal El DeepNo ratings yet
- HTML Tags Chart For CodingDocument9 pagesHTML Tags Chart For CodingBalaji_SAPNo ratings yet
- Rman To Windows DriveDocument3 pagesRman To Windows DrivecarlosNo ratings yet
- Mathworks-Matlab Programming Fundamentals r2017b-2017Document1,360 pagesMathworks-Matlab Programming Fundamentals r2017b-2017ivansanc100% (1)
- Num 1 Den (1 20 30) Plant TF (Num, Den) Step (Plant,'r') Xlabel ('Amplitude - ') Ylabel ('Time - ') Title ('Plant Function Response')Document7 pagesNum 1 Den (1 20 30) Plant TF (Num, Den) Step (Plant,'r') Xlabel ('Amplitude - ') Ylabel ('Time - ') Title ('Plant Function Response')mohanNo ratings yet