Download as pdf or txt
You might also like
- Differences Between British, Canadian and American SpellingDocument9 pagesDifferences Between British, Canadian and American SpellingMr. doody100% (2)
- Critical Care Goals and ObjectivesDocument28 pagesCritical Care Goals and ObjectivesjyothiNo ratings yet
- History and Phhyscical Examination OrthopaedicsDocument4 pagesHistory and Phhyscical Examination OrthopaedicsPATHMAPRIYA GANESANNo ratings yet
- 4.NIKEN-crowding Destinaion PDFDocument7 pages4.NIKEN-crowding Destinaion PDFAli Akbar RahmaniNo ratings yet
- Patient Perceptions of Emergency Department Fast Track: A Prospective Pilot Study Comparing Two Models of CareDocument3 pagesPatient Perceptions of Emergency Department Fast Track: A Prospective Pilot Study Comparing Two Models of CareErvin WidhiantyasNo ratings yet
- Er ReadingsDocument6 pagesEr ReadingsReginald UyNo ratings yet
- Implementation of A Provider in Triage and Its Effect On Left Without Being Seen Rate at A Community Trauma CenterDocument5 pagesImplementation of A Provider in Triage and Its Effect On Left Without Being Seen Rate at A Community Trauma CenterEpifanus Arie TanotoNo ratings yet
- Get Homework/Assignment DoneDocument6 pagesGet Homework/Assignment Donehomeworkping1No ratings yet
- Modeling and Simulation of Patient Flow in Hospitals For Resource UtilizationDocument10 pagesModeling and Simulation of Patient Flow in Hospitals For Resource UtilizationIndra GunawanNo ratings yet
- Delay EmergencyDocument6 pagesDelay EmergencyKharisma PutraNo ratings yet
- Decreasing Length of Stay in The Emergency Department With A Split Emergency Severity Index 3 Patient Flow ModelDocument9 pagesDecreasing Length of Stay in The Emergency Department With A Split Emergency Severity Index 3 Patient Flow ModelrutnomleniNo ratings yet
- Turning Frequency in Adult Bedridden Patients To Prevent Hospital-Acquired Pressure Ulcer: A Scoping ReviewDocument12 pagesTurning Frequency in Adult Bedridden Patients To Prevent Hospital-Acquired Pressure Ulcer: A Scoping ReviewfajaqaNo ratings yet
- Emergency Physician Awareness of Prehospital ProceDocument8 pagesEmergency Physician Awareness of Prehospital ProceNines RíosNo ratings yet
- High Hospital Occupancy Is Associated With Increased Risk For Patients Boarding in The Emergency DepartmentDocument7 pagesHigh Hospital Occupancy Is Associated With Increased Risk For Patients Boarding in The Emergency DepartmentdrartzNo ratings yet
- Original Research: Intensive Care Unit Structure Variation and Implications For Early Mobilization PracticesDocument12 pagesOriginal Research: Intensive Care Unit Structure Variation and Implications For Early Mobilization Practicesandi kurniawanNo ratings yet
- Utilizing Health Analytics in ImprovingDocument9 pagesUtilizing Health Analytics in ImprovingLikithaNo ratings yet
- Medline 8Document8 pagesMedline 8Veronica GomesNo ratings yet
- Emergency Medicine Resident Efficiency and Emergency Department CrowdingDocument9 pagesEmergency Medicine Resident Efficiency and Emergency Department CrowdingRenzo Iván Marín DávalosNo ratings yet
- Estimating A Reasonable Patient Panel Size For Primary Care Physicians With Team-Based Task DelegationDocument5 pagesEstimating A Reasonable Patient Panel Size For Primary Care Physicians With Team-Based Task DelegationEmily NascimentoNo ratings yet
- Journal Pone 0154372 PDFDocument15 pagesJournal Pone 0154372 PDFrutnomleniNo ratings yet
- Factors Affecting ED Length-of-Stay in Surgical Critical Care PatientsDocument6 pagesFactors Affecting ED Length-of-Stay in Surgical Critical Care PatientsMuhammad HidayantoNo ratings yet
- Art:10.1186/s12873 016 0102 5 PDFDocument8 pagesArt:10.1186/s12873 016 0102 5 PDFrutnomleniNo ratings yet
- Original Article: The Weekend Effect: Does Time of Admission Impact Management and Outcomes of Small Bowel Obstruction?Document5 pagesOriginal Article: The Weekend Effect: Does Time of Admission Impact Management and Outcomes of Small Bowel Obstruction?DeVisShoppNo ratings yet
- Healthcare 3Document6 pagesHealthcare 3Noor KhanNo ratings yet
- Putnam 2014Document7 pagesPutnam 2014mia widiastutiNo ratings yet
- Handover Paper Final 22 3 16 BJNDocument13 pagesHandover Paper Final 22 3 16 BJNsisaraaah12No ratings yet
- ArticleDocument5 pagesArticleJosé Ilton limaNo ratings yet
- Sepsis Screen Treatment AlgorithmDocument66 pagesSepsis Screen Treatment AlgorithmcindythungNo ratings yet
- Shortstay LiteratureDocument5 pagesShortstay LiteratureDon RicaforteNo ratings yet
- A Study On Waiting Time of The OPD Patient in A Multispecialty HospitalDocument6 pagesA Study On Waiting Time of The OPD Patient in A Multispecialty HospitalIJRASETPublicationsNo ratings yet
- Effects of Nursing Rounds: On Patients' Call Light Use, Satisfaction, and SafetyDocument13 pagesEffects of Nursing Rounds: On Patients' Call Light Use, Satisfaction, and SafetyhanimozaghiNo ratings yet
- J 1553-2712 2011 01122 X PDFDocument8 pagesJ 1553-2712 2011 01122 X PDFSriatiNo ratings yet
- 13 SPDocument8 pages13 SPDaroo D.TNo ratings yet
- Consultation Outcomes in The Emergency Department Exploring Rates and ComplexityDocument7 pagesConsultation Outcomes in The Emergency Department Exploring Rates and ComplexityAngela LilianaNo ratings yet
- The Addition of A Nurse Practitioner To An Inpatient Surgical Team Results in Improved Use of ResourcesDocument7 pagesThe Addition of A Nurse Practitioner To An Inpatient Surgical Team Results in Improved Use of Resourcesericc949432No ratings yet
- Emergency DepartmentDocument9 pagesEmergency DepartmentSarah Mae SanchezNo ratings yet
- CR4 PDFDocument3 pagesCR4 PDFPalak BatraNo ratings yet
- Harris 2012Document5 pagesHarris 2012Nurul AidaNo ratings yet
- Forecasting Waiting Time To Treatment For Emergency Department PatientsDocument29 pagesForecasting Waiting Time To Treatment For Emergency Department PatientsBudi RiyantoPrabowoNo ratings yet
- CMRP0218Document14 pagesCMRP0218cherish60126No ratings yet
- ResearchDocument11 pagesResearchIMNG_PDFNo ratings yet
- Hardy 2017Document8 pagesHardy 2017Achmad SetyaNo ratings yet
- E O - M A C N P A C N P: Ffect of An Utcomes Anaged Pproach To Are of Euroscience Atients by Cute ARE Urse RactitionersDocument12 pagesE O - M A C N P A C N P: Ffect of An Utcomes Anaged Pproach To Are of Euroscience Atients by Cute ARE Urse RactitionersFathchur RohmanNo ratings yet
- S0196064413X00125 S0196064413010895 Main PDFDocument2 pagesS0196064413X00125 S0196064413010895 Main PDFwilmaNo ratings yet
- Association Between Emergency Department Length Of.10Document6 pagesAssociation Between Emergency Department Length Of.10mutu wonogiriNo ratings yet
- Journal Homepage: - : Introduction:-Objectives of The StudyDocument4 pagesJournal Homepage: - : Introduction:-Objectives of The StudyIJAR JOURNALNo ratings yet
- Qualitative ResearchDocument9 pagesQualitative ResearchGideon M KimariNo ratings yet
- RCT 1Document19 pagesRCT 1Riyan UkiNo ratings yet
- Daily Interruption of Sedation in Patients Receiving Mechanical VentilationDocument10 pagesDaily Interruption of Sedation in Patients Receiving Mechanical VentilationEryll Jean SamotNo ratings yet
- 38 Hoot 2007Document9 pages38 Hoot 2007ARTZchebilNo ratings yet
- Effectofcarereducationon Functionalabilitiesofpatients WithstrokeDocument7 pagesEffectofcarereducationon Functionalabilitiesofpatients WithstrokeDan Gerald Alcido SalungaNo ratings yet
- Nguyen 2019Document6 pagesNguyen 2019ClintonNo ratings yet
- Evaluation and Outcome of Patients After Polytrauma-Can Patients Be Recruited For Long-Term Follow-UpDocument7 pagesEvaluation and Outcome of Patients After Polytrauma-Can Patients Be Recruited For Long-Term Follow-UpVfor VendettaNo ratings yet
- ASE Reintro Statement FINALDocument14 pagesASE Reintro Statement FINALIrina Cabac-PogoreviciNo ratings yet
- Sacks - Variation in Hospital UseDocument9 pagesSacks - Variation in Hospital UseUm ShooqNo ratings yet
- Two-Year Outcome After Endovascular Treatment For Acute Ischemic StrokeDocument9 pagesTwo-Year Outcome After Endovascular Treatment For Acute Ischemic Strokedoni anandaNo ratings yet
- International Emergency Nursing: P. Roivainen, M.J. Hoikka, T.I. Ala-Kokko, M. K A Ari AinenDocument7 pagesInternational Emergency Nursing: P. Roivainen, M.J. Hoikka, T.I. Ala-Kokko, M. K A Ari AinenAinulNo ratings yet
- NIH Public Access: Author ManuscriptDocument12 pagesNIH Public Access: Author ManuscriptvenyNo ratings yet
- Pa Shik Anti 2012Document8 pagesPa Shik Anti 2012Irfan FauziNo ratings yet
- H C P T I O: Ealth ARE Rovider in Riage To Mprove UtcomesDocument6 pagesH C P T I O: Ealth ARE Rovider in Riage To Mprove Utcomesbayu sih aksami khasanahNo ratings yet
- Effectiveness Mobility Protocol Towards Intensive Care Unit PatientsDocument10 pagesEffectiveness Mobility Protocol Towards Intensive Care Unit PatientsMhar IcelNo ratings yet
- The Maximally Efficient and Optimally Effective Emergency Department: One Good Thing A DayFrom EverandThe Maximally Efficient and Optimally Effective Emergency Department: One Good Thing A DayNo ratings yet
- Bookshelf NBK153098Document238 pagesBookshelf NBK153098Beny HermawanNo ratings yet
- Jurnal 9Document312 pagesJurnal 9Beny HermawanNo ratings yet
- Jurnal 12Document142 pagesJurnal 12Beny HermawanNo ratings yet
- Jurnal 16Document166 pagesJurnal 16Beny HermawanNo ratings yet
- Jurnal 9Document312 pagesJurnal 9Beny HermawanNo ratings yet
- DispesingDocument36 pagesDispesingLupus BoyssNo ratings yet
- PBL NeuroDocument45 pagesPBL NeuroInsan_aqidNo ratings yet
- Frankel's Functional Regulator / Orthodontic Courses by Indian Dental AcademyDocument129 pagesFrankel's Functional Regulator / Orthodontic Courses by Indian Dental Academyindian dental academy100% (4)
- Pemeriksaan GonioskopiDocument26 pagesPemeriksaan GonioskopiMuhammad Mu'amar HabibieNo ratings yet
- Final TML JuneDocument144 pagesFinal TML JuneTinTin CjNo ratings yet
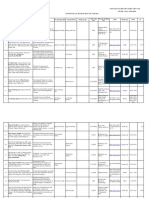
- Danh Sach Bai Bao Quoc Te 2020 794Document14 pagesDanh Sach Bai Bao Quoc Te 2020 794Master DrNo ratings yet
- Pediatric DentistryDocument15 pagesPediatric DentistryPeyman Dhg100% (2)
- Musculosleketal Risk Assesment Among Nurses in Pateint Manual Handling in Hospital Wards - A Cross Sectional StudyDocument10 pagesMusculosleketal Risk Assesment Among Nurses in Pateint Manual Handling in Hospital Wards - A Cross Sectional StudyCureusNo ratings yet
- NSI New FlowchartDocument4 pagesNSI New FlowchartL054-Melissa Ong Lie LianNo ratings yet
- Cast and MoldsDocument11 pagesCast and Moldskaliente0118No ratings yet
- School ResumeDocument1 pageSchool Resumerachel crawfordNo ratings yet
- NPB 840 CatalogueDocument8 pagesNPB 840 CatalogueSumair Saeed KhanNo ratings yet
- Dr. Boyd, Darwinian Dentistry Part 2Document6 pagesDr. Boyd, Darwinian Dentistry Part 2lisakatevNo ratings yet
- Testing Placement of Nasogastric Tubes in Infants & ChildrenDocument4 pagesTesting Placement of Nasogastric Tubes in Infants & ChildrenYwagar YwagarNo ratings yet
- Barrier To CommunicationDocument10 pagesBarrier To CommunicationDianaNo ratings yet
- Maternal History InterviewDocument4 pagesMaternal History InterviewaringkinkingNo ratings yet
- Singrauli - PIP ReportDocument29 pagesSingrauli - PIP Reportgaurav chauhanNo ratings yet
- Patients With Anaplastic Thyroid CancerDocument45 pagesPatients With Anaplastic Thyroid Cancerfanny_febrianiNo ratings yet
- ENGLISH - Reading - Grammar. UNIT 5.Document14 pagesENGLISH - Reading - Grammar. UNIT 5.Angie ReyesNo ratings yet
- Unit 1Document20 pagesUnit 1Sandhya BasnetNo ratings yet
- Reflex Sympathetic Dystrophy, CRPS-1Document47 pagesReflex Sympathetic Dystrophy, CRPS-1Sayantika Dhar100% (1)
- Management of Severe Pre-Eclampsia and Eclampsia Update 2009Document6 pagesManagement of Severe Pre-Eclampsia and Eclampsia Update 2009Praveen RadhakrishnanNo ratings yet
- Medical and Surgical History of The WarDocument1,136 pagesMedical and Surgical History of The WarsuzenataleNo ratings yet
- Joint Annual Scientific Meeting 2020Document1 pageJoint Annual Scientific Meeting 2020Tom ChanNo ratings yet
- LOLADocument23 pagesLOLASHOW_ME_DEM_TITIESNo ratings yet
- The Ortho PodDocument60 pagesThe Ortho PodxyequusNo ratings yet
- Bilateral Hydronephrosis - A Case With An Unfavorable OutcomeDocument4 pagesBilateral Hydronephrosis - A Case With An Unfavorable OutcomeMihai Cristian HodorogNo ratings yet