Download as pdf or txt
You might also like
- Intra Operative MonitoringDocument4 pagesIntra Operative MonitoringEsamNo ratings yet
- Closing The Loop Patient SafetyDocument34 pagesClosing The Loop Patient SafetyVirginia Abalos0% (1)
- Enhancing Nurses Pain Assessment To Improve.11Document2 pagesEnhancing Nurses Pain Assessment To Improve.11Na d'Nazaie CodeNo ratings yet
- 1 Perspectives of Pediatric NursingDocument57 pages1 Perspectives of Pediatric NursingBluebloodboyNo ratings yet
- SBAs and EMQs For MRCOG II Addressing The New Exam Format2Document460 pagesSBAs and EMQs For MRCOG II Addressing The New Exam Format2Hasan Dahamsheh92% (13)
- Maquet Operating Table Betaclassic - User ManualDocument24 pagesMaquet Operating Table Betaclassic - User Manualpaninaro100% (4)
- Patient Safety: What Should We Be Trying To Communicate?Document32 pagesPatient Safety: What Should We Be Trying To Communicate?cicaklomenNo ratings yet
- Iso and HealthDocument11 pagesIso and Healthjavier yesidNo ratings yet
- Clinical Practice Guidelines GS PIMSDocument86 pagesClinical Practice Guidelines GS PIMSDrvikash Singh100% (1)
- Assessment of Knowledge Attitude and Practices Regarding Awareness of Biomedical Waste Management Among Health Care Personnel A Cross-Sectional SurveyDocument5 pagesAssessment of Knowledge Attitude and Practices Regarding Awareness of Biomedical Waste Management Among Health Care Personnel A Cross-Sectional SurveyAms BeeNo ratings yet
- Day Surgery Update 2019Document15 pagesDay Surgery Update 2019O Mei NeilNo ratings yet
- Patient Safety 1, 2Document98 pagesPatient Safety 1, 2salah salem100% (1)
- Guide To Clinical Audit Antibiotic Use in Urinary Tract InfectionDocument10 pagesGuide To Clinical Audit Antibiotic Use in Urinary Tract Infectionihtisham1No ratings yet
- Regulations in Organ Transplantation in IndiaDocument8 pagesRegulations in Organ Transplantation in IndiaRoss DennyNo ratings yet
- Breastfeeding Posters and DisplaysDocument3 pagesBreastfeeding Posters and DisplaysDhea Rizky Amelia SatoNo ratings yet
- Day Care SurgeryDocument5 pagesDay Care SurgeryazharmoNo ratings yet
- Blood Transfusion Error Prevention - Nurses RoleDocument5 pagesBlood Transfusion Error Prevention - Nurses RoleLorenn AdarnaNo ratings yet
- Hospital Incident ReportingDocument32 pagesHospital Incident Reportingakhtarulmunim2279No ratings yet
- Saudi Guidelines For Informed Consent: First Edition 1440H (2019G)Document52 pagesSaudi Guidelines For Informed Consent: First Edition 1440H (2019G)Munira Nasser Said DawoodNo ratings yet
- Patient SafetyDocument133 pagesPatient Safetydrabhimanyu_b6956100% (1)
- Safety Event Reporting PolicyDocument10 pagesSafety Event Reporting PolicypatientsafetyNo ratings yet
- Patient Safety PPT PDFDocument39 pagesPatient Safety PPT PDFGraha KhitanNo ratings yet
- Sentinel Events: Vidya PrasadDocument21 pagesSentinel Events: Vidya PrasadTOUSHIFAHEMEDNo ratings yet
- Actionable Patient Safety Solutions (APSS)Document441 pagesActionable Patient Safety Solutions (APSS)aku kaukuaNo ratings yet
- National Integrated Emergency Medicine TrainingDocument274 pagesNational Integrated Emergency Medicine TrainingAddisu AdaneNo ratings yet
- Patient and Family Medication Education PolicyDocument2 pagesPatient and Family Medication Education PolicyspiceyjoeNo ratings yet
- Quality Improvement ProjectDocument13 pagesQuality Improvement Projectapi-384138456No ratings yet
- Day Case For WebDocument34 pagesDay Case For WebDavid CruzNo ratings yet
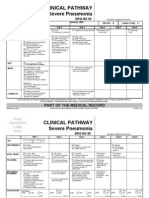
- Clinical Pathways Severe PneumoniaDocument2 pagesClinical Pathways Severe PneumoniaaandakuNo ratings yet
- Cauti PreventionDocument25 pagesCauti Preventionapi-340154088No ratings yet
- Modified Early Obstetric Warning Score MEOWS MID33 AO13 v4.2Document9 pagesModified Early Obstetric Warning Score MEOWS MID33 AO13 v4.2indirinoor5No ratings yet
- Hourly Round ProjectDocument8 pagesHourly Round ProjectaustinisaacNo ratings yet
- Resume: Mobile KSA: 00966536979152 Mobile Jordan: 00962795661774 EmailDocument8 pagesResume: Mobile KSA: 00966536979152 Mobile Jordan: 00962795661774 EmailAhmad Khalil Ahmad Al-SadiNo ratings yet
- Clinical AuditDocument5 pagesClinical AuditdrskumarNo ratings yet
- 7 Steps Patient SafetyDocument58 pages7 Steps Patient SafetyDanissa Fidia PuteriNo ratings yet
- Aorn Proposed Guidelines For Sterile TechniqueDocument104 pagesAorn Proposed Guidelines For Sterile TechniqueRudy DuterteNo ratings yet
- Patient Safety and Quality Care MovementDocument9 pagesPatient Safety and Quality Care Movementapi-300362983No ratings yet
- Accomplishment Report 2017 - IcuDocument5 pagesAccomplishment Report 2017 - IcuMikhaelEarlSantosTacordaNo ratings yet
- SWOT Analysis of The Emergency ServiceDocument20 pagesSWOT Analysis of The Emergency ServiceScribdTranslationsNo ratings yet
- Innovations in Medical Education - PptxfinalDocument15 pagesInnovations in Medical Education - PptxfinalSujatha RagoorNo ratings yet
- Icu Delirium Final PaperDocument12 pagesIcu Delirium Final Paperapi-348346538No ratings yet
- Patient SafetyDocument27 pagesPatient Safetyarahman168No ratings yet
- Key Performance Indicator Description: Nursing Care Kpis (1/2)Document4 pagesKey Performance Indicator Description: Nursing Care Kpis (1/2)Olaya alghareniNo ratings yet
- Improving Operating Theatre Performance Complete Step Guide Without PicDocument83 pagesImproving Operating Theatre Performance Complete Step Guide Without PicNana AkwaboahNo ratings yet
- Cannulation TrainingGuideDocument28 pagesCannulation TrainingGuideKavidu Keshan100% (1)
- Hospital Wards and Departments: By: Drs. Nur Panca Marhendra, M.PDDocument35 pagesHospital Wards and Departments: By: Drs. Nur Panca Marhendra, M.PDSerendipity English100% (1)
- Activities Patient SafetyDocument13 pagesActivities Patient SafetyummuawisyNo ratings yet
- Opd MSDocument35 pagesOpd MSkanikaNo ratings yet
- IPSGDocument4 pagesIPSGmohsinaNo ratings yet
- Different Departments Required in A HospitalDocument11 pagesDifferent Departments Required in A HospitalEdsel Dudes AbanteNo ratings yet
- Access To Care and Continuity of CareDocument44 pagesAccess To Care and Continuity of CareCamille Honeyleith Lanuza FernandoNo ratings yet
- Quality Audit Experience in HealthcareDocument15 pagesQuality Audit Experience in HealthcareMrzitedakucasam Seminarski,Diplomski radoviNo ratings yet
- Code of Medical EthicsDocument33 pagesCode of Medical Ethicsp1843dNo ratings yet
- Patient SafetyDocument11 pagesPatient SafetyMardiyanti FirmanNo ratings yet
- Clinical Science Questions and Answers - Standards MaintainedDocument7 pagesClinical Science Questions and Answers - Standards MaintainedManish JainNo ratings yet
- Southern Philippines Medical CenterDocument19 pagesSouthern Philippines Medical CenterST ANNE GENERAL HOSPITAL INC (SAFETY DEPARTMENT)100% (1)
- Guidelines - Safe - Surgery MOH PDFDocument97 pagesGuidelines - Safe - Surgery MOH PDFlisaNo ratings yet
- IPSGDocument16 pagesIPSGNyimas Milka Ayu NabilaNo ratings yet
- Final Pre Accreditation Entry Level Standards For Hospital Book PDFDocument53 pagesFinal Pre Accreditation Entry Level Standards For Hospital Book PDFams_1234100% (1)
- Medication ErrorDocument22 pagesMedication ErrorSulastri LastriNo ratings yet
- Patient Safety Organization A Complete Guide - 2020 EditionFrom EverandPatient Safety Organization A Complete Guide - 2020 EditionNo ratings yet
- Correctional Health Care Patient Safety Handbook: Reduce Clinical Error, Manage Risk, and Improve QualityFrom EverandCorrectional Health Care Patient Safety Handbook: Reduce Clinical Error, Manage Risk, and Improve QualityRating: 2 out of 5 stars2/5 (1)
- Principles Cancer Systemic TherapyDocument57 pagesPrinciples Cancer Systemic TherapyKarimina50% (2)
- Job Description of ICU Staff NurseDocument1 pageJob Description of ICU Staff NurseGAGANJOT8550% (2)
- Case of The Week (Hypercalcemia)Document23 pagesCase of The Week (Hypercalcemia)ckyew64No ratings yet
- Pamphlet Liver BiopsyDocument8 pagesPamphlet Liver BiopsyManisha ShakyaNo ratings yet
- Blood Supply To Femoral HeadDocument3 pagesBlood Supply To Femoral HeadReinita Arlin PringgoredjoNo ratings yet
- Inspection Workbook Obstetrics and GynecologyDocument40 pagesInspection Workbook Obstetrics and Gynecologydelap05No ratings yet
- Echocardiographic Anatomy in The FetusDocument14 pagesEchocardiographic Anatomy in The FetusAnonymous hOHi6TZTnNo ratings yet
- DRG Griya Ridha Raharja: IIUM MalaysiaDocument3 pagesDRG Griya Ridha Raharja: IIUM MalaysiaBudi AthAnza SuhartonoNo ratings yet
- Newborn Assessment PDFDocument123 pagesNewborn Assessment PDFSarahNo ratings yet
- Obstetrics Notes by DR Kamal Deep PDFDocument33 pagesObstetrics Notes by DR Kamal Deep PDFKrisha PatelNo ratings yet
- Catherine Jenkins ReportDocument60 pagesCatherine Jenkins Reportjupiter stationeryNo ratings yet
- The Effects of Nursing Care Based On Watson's Theory of Human CaringDocument7 pagesThe Effects of Nursing Care Based On Watson's Theory of Human CaringNadhifah RahmawatiNo ratings yet
- College Essay Example #3: This Is A College Essay That Worked ForDocument2 pagesCollege Essay Example #3: This Is A College Essay That Worked For4- Desiree FuaNo ratings yet
- LFD 15 IudmcDocument2 pagesLFD 15 IudmcMaria Elvira Abrogena DuadNo ratings yet
- Sample Cleaning Checklist OR Pre and Postop TEMPLATEDocument3 pagesSample Cleaning Checklist OR Pre and Postop TEMPLATEFalochNo ratings yet
- Aisha Tabassum EtalDocument4 pagesAisha Tabassum EtaleditorijmrhsNo ratings yet
- CSB BookletDocument36 pagesCSB BookletHitesh Parmar100% (2)
- GerdDocument83 pagesGerdFebrila HarmainiNo ratings yet
- Cesarean Scar Defect: A Prospective Study On Risk Factors: GynecologyDocument8 pagesCesarean Scar Defect: A Prospective Study On Risk Factors: Gynecologynuphie_nuphNo ratings yet
- Colpocleisis: A Guide For WomenDocument2 pagesColpocleisis: A Guide For WomenbayuwinotoNo ratings yet
- More Serious Health ProblemsDocument3 pagesMore Serious Health ProblemsYassin KhanNo ratings yet
- Legal and Ethical Issues in Nursing DiscussionDocument3 pagesLegal and Ethical Issues in Nursing Discussionapi-639782898No ratings yet
- Pneumonperitoneum A Review of Nonsurgical Causes PDFDocument7 pagesPneumonperitoneum A Review of Nonsurgical Causes PDFDellysa Eka Nugraha TNo ratings yet
- Medical Documentation - Nan SharafiDocument13 pagesMedical Documentation - Nan Sharafi756bynw6jcNo ratings yet
- Obstetric History Taking - OSCE GuideDocument18 pagesObstetric History Taking - OSCE Guideabdalbaset100% (1)
- Protocol MSCT 16 For Pediatric CardiovascDocument7 pagesProtocol MSCT 16 For Pediatric CardiovascirmaNo ratings yet
- Cleft Lip & Palate: Presented by Sameerah Al-SomaliDocument35 pagesCleft Lip & Palate: Presented by Sameerah Al-SomaliriyasavlaNo ratings yet
- GesamtkatalogDocument190 pagesGesamtkatalogAntonio BerebereNo ratings yet