Download as pdf or txt
You might also like
- The Myth of Autism: How a Misunderstood Epidemic Is Destroying Our Children, Expanded and Revised EditionFrom EverandThe Myth of Autism: How a Misunderstood Epidemic Is Destroying Our Children, Expanded and Revised EditionRating: 2.5 out of 5 stars2.5/5 (3)
- ADR Reporting FormDocument2 pagesADR Reporting FormApoorva Tatti100% (1)
- Multiple Pregnancy LectureDocument33 pagesMultiple Pregnancy Lecturefarid_nchep100% (1)
- ACLS For TachycardiaDocument31 pagesACLS For TachycardiaTausif HaqueNo ratings yet
- Brain 2014 Yu Brain Awu239Document5 pagesBrain 2014 Yu Brain Awu239Angeles RbNo ratings yet
- Exercise-Associated Numbness and Tingling in The Legs: For Editorial Comment See Page 1509Document4 pagesExercise-Associated Numbness and Tingling in The Legs: For Editorial Comment See Page 1509herpthederpNo ratings yet
- Cabot 2007Document9 pagesCabot 2007marchsheyNo ratings yet
- Heart Failure in A ChildDocument8 pagesHeart Failure in A ChildChici FarlinaNo ratings yet
- Laporan Kasus: A 44-Day Old Male Infant With Thoracoabdominal Ectopia Cordis of Pentalogy Cantrell'S SyndromeDocument6 pagesLaporan Kasus: A 44-Day Old Male Infant With Thoracoabdominal Ectopia Cordis of Pentalogy Cantrell'S SyndromearlitasofyanNo ratings yet
- Adem LikeDocument4 pagesAdem LikeRodrigo AriasNo ratings yet
- Agenesia CerebeloDocument5 pagesAgenesia CerebeloDiretoria CientíficaNo ratings yet
- Ischemic Chiasmal Syndrome and Hypopituitarism Associated With Progressive Cerebrovascular Occlusive DiseaseDocument5 pagesIschemic Chiasmal Syndrome and Hypopituitarism Associated With Progressive Cerebrovascular Occlusive DiseaseJaime TobarNo ratings yet
- Thalssemia & Spinal Cord Compression in PregnancyDocument1 pageThalssemia & Spinal Cord Compression in PregnancyThao NguyenNo ratings yet
- EBSTEIN'S ANOMALY Dhini - Maju 17 Juli 2014Document29 pagesEBSTEIN'S ANOMALY Dhini - Maju 17 Juli 2014Azizi PranokoNo ratings yet
- Leukodystrophies and MucopolysacridosisDocument78 pagesLeukodystrophies and MucopolysacridosisMobin Ur Rehman KhanNo ratings yet
- Neuroradiological Findings of Trisomy 13 in A Rare Long-Term SurvivorDocument3 pagesNeuroradiological Findings of Trisomy 13 in A Rare Long-Term Survivorchristian roblesNo ratings yet
- 678 FullDocument5 pages678 Fullakram socisseNo ratings yet
- Rare Intracardiac Yolk Sac Tumour Rjw187Document4 pagesRare Intracardiac Yolk Sac Tumour Rjw187jagadeeshNo ratings yet
- Evolution of Technetium-99m-HMPAO SPECT and Brain Mapping in A Patient Presenting With Echolalia and PalilaliaDocument3 pagesEvolution of Technetium-99m-HMPAO SPECT and Brain Mapping in A Patient Presenting With Echolalia and PalilaliaMihaela ToaderNo ratings yet
- Pediatrics Etiologia 2Document5 pagesPediatrics Etiologia 2Julio YedesNo ratings yet
- Leopard SyndromeDocument9 pagesLeopard Syndromenoira.uvasNo ratings yet
- Primary Aldosteronism Caused by Unilateral Adrenal Hyperplasia: Rethinking The Accuracy of Imaging StudiesDocument5 pagesPrimary Aldosteronism Caused by Unilateral Adrenal Hyperplasia: Rethinking The Accuracy of Imaging StudiesRonald DelosendoNo ratings yet
- Corazon y SojenDocument7 pagesCorazon y Sojenmaria cristina aravenaNo ratings yet
- Solomon 1969Document3 pagesSolomon 1969putu risyaNo ratings yet
- 852-Article Text-1602-1-10-20190613Document12 pages852-Article Text-1602-1-10-20190613anidar1245No ratings yet
- Pedia SGD NICUDocument62 pagesPedia SGD NICUJAIRISH YZABELLE SALVADORNo ratings yet
- Tmp9e41 TMPDocument3 pagesTmp9e41 TMPFrontiersNo ratings yet
- Caso Clinico Clinica Mayo 2Document5 pagesCaso Clinico Clinica Mayo 2Francisco HernandezNo ratings yet
- Survival of A Neurologically Intact Patient With Subarachnoid Hemorrhage and Cardiopulmonary ArrestDocument4 pagesSurvival of A Neurologically Intact Patient With Subarachnoid Hemorrhage and Cardiopulmonary ArrestDino RatnamNo ratings yet
- Clinical Cases: Ischaemic Heart DiseaseDocument4 pagesClinical Cases: Ischaemic Heart DiseaseLADY JOWAHER ALLASNo ratings yet
- Large Arachnoid Cyst: T. Mondal K. Jagdish Kumar R. Anand N.K. Dubey D. SharmaDocument3 pagesLarge Arachnoid Cyst: T. Mondal K. Jagdish Kumar R. Anand N.K. Dubey D. SharmaJaya PrabhaNo ratings yet
- A 38 Year Old Woman With Global Aphasia and MigraiDocument4 pagesA 38 Year Old Woman With Global Aphasia and MigraiAchmad Dodi MeidiantoNo ratings yet
- Hemimegalencephaly: A Study of Abnormalities Occurring Outside The Involved HemisphereDocument5 pagesHemimegalencephaly: A Study of Abnormalities Occurring Outside The Involved Hemisphereapi-148100258No ratings yet
- Cases - Fisical DevelopDocument5 pagesCases - Fisical DevelopSarthak DubeyNo ratings yet
- Renal Bruit Due To Aberrant Renal Vessels: Indian Pediatrics VOLUME 32-MARCH1995Document3 pagesRenal Bruit Due To Aberrant Renal Vessels: Indian Pediatrics VOLUME 32-MARCH1995ShamNo ratings yet
- 9.pediatric Dural Arteriovenous MalformationsDocument7 pages9.pediatric Dural Arteriovenous MalformationsNisa MahdiataraNo ratings yet
- Is Central Pontine Myelinolysis A Sign of Pre-Symptomatic Neurologic Form of Wilson Disease?Document2 pagesIs Central Pontine Myelinolysis A Sign of Pre-Symptomatic Neurologic Form of Wilson Disease?Ricardo ZetaNo ratings yet
- Cardiology ExamDocument9 pagesCardiology ExamKhadar mohamedNo ratings yet
- PosterDocument5 pagesPosterNitika SharmaNo ratings yet
- 9 RFTCXDocument24 pages9 RFTCXpotnic44No ratings yet
- EPIDURIALDocument3 pagesEPIDURIALALBERTO URIEL MONTAÑO CERVANTESNo ratings yet
- Pallister-Killian Mosaic Syndrome in An Omani NewbDocument5 pagesPallister-Killian Mosaic Syndrome in An Omani NewbFrank Harry LampardNo ratings yet
- Delhi July 2018Document18 pagesDelhi July 2018quillcharmNo ratings yet
- منهج الحراحة العامةDocument36 pagesمنهج الحراحة العامةAndro GalaxNo ratings yet
- Xrayand ElectrocardiogramDocument104 pagesXrayand ElectrocardiogramdrelvNo ratings yet
- Transcranial Ultrasound Doppler Parameters in CereDocument7 pagesTranscranial Ultrasound Doppler Parameters in CereImin BuntaraNo ratings yet
- Dr. A. Ramcharan's Firm Thursday 31 Match 2011Document56 pagesDr. A. Ramcharan's Firm Thursday 31 Match 2011Ronald ChongNo ratings yet
- Posterior Reversible Encephalopathy Syndrome Secondary To Acute Post-Streptococcal Glomerulonephritis in A 12-Year-Old GirlDocument2 pagesPosterior Reversible Encephalopathy Syndrome Secondary To Acute Post-Streptococcal Glomerulonephritis in A 12-Year-Old GirlwawaningNo ratings yet
- Cla Eys 1997Document6 pagesCla Eys 1997jahfdfgsdjad asdhsajhajdkNo ratings yet
- Omur - Tc-99m MIBI Myocard Perfusion SPECT Findings in Patients With Typical Chest Pain and Normal Coronary ArteriesDocument8 pagesOmur - Tc-99m MIBI Myocard Perfusion SPECT Findings in Patients With Typical Chest Pain and Normal Coronary ArteriesM. PurnomoNo ratings yet
- Radiology ReportDocument4 pagesRadiology ReportMayNo ratings yet
- Kearn Sayre Syndrome Brheartj00076-0090Document5 pagesKearn Sayre Syndrome Brheartj00076-0090Heart of the Valley, Pediatric CardiologyNo ratings yet
- HSS Clinical Pronostic ConsiderationDocument4 pagesHSS Clinical Pronostic ConsiderationReyes Ivan García CuevasNo ratings yet
- Article Heart-2001-Lindström-31-8Document9 pagesArticle Heart-2001-Lindström-31-8dgina8800No ratings yet
- Aortic Dissection Associated With Aortic Aneurysms and Posterior Paresis in A DogDocument7 pagesAortic Dissection Associated With Aortic Aneurysms and Posterior Paresis in A DogMuhamad Abdul MubdiNo ratings yet
- PDF JNS 27Document7 pagesPDF JNS 27emreyavuz8745No ratings yet
- Imp Points - Khalid Iqbal Waqar YounisDocument16 pagesImp Points - Khalid Iqbal Waqar YounisJansher Ali Chohan100% (1)
- A Detail of The Molecular AnatomyDocument5 pagesA Detail of The Molecular AnatomyMihaela Simona IsacNo ratings yet
- Nejmcps 2116690Document8 pagesNejmcps 2116690Luis MadrigalNo ratings yet
- Circulation 1961 HERSCH 853 60Document9 pagesCirculation 1961 HERSCH 853 60chuck55No ratings yet
- Acute Pseudobulbar Palsy After Bilateral ParamediaDocument6 pagesAcute Pseudobulbar Palsy After Bilateral ParamediaGeraldi ContrerasNo ratings yet
- Lapkas Pediatrik NLDocument31 pagesLapkas Pediatrik NLHannaTashiaClaudiaNo ratings yet
- The Myth of Autism: How a Misunderstood Epidemic Is Destroying Our ChildrenFrom EverandThe Myth of Autism: How a Misunderstood Epidemic Is Destroying Our ChildrenRating: 2.5 out of 5 stars2.5/5 (8)
- Liss DFDocument48 pagesLiss DFthomsoon010% (1)
- Sirtalis SurgicalDocument8 pagesSirtalis Surgicalthomsoon01No ratings yet
- Acumed® Dual-Trak Clavicle ScrewDocument12 pagesAcumed® Dual-Trak Clavicle Screwthomsoon01No ratings yet
- 3 5mmClavHookPlateDocument11 pages3 5mmClavHookPlatethomsoon01No ratings yet
- Acumed® Clavicle PlatingDocument68 pagesAcumed® Clavicle Platingthomsoon01No ratings yet
- Moyamoya DiseaseDocument14 pagesMoyamoya Diseasethomsoon01No ratings yet
- Antegrade Femoral Nail (AFN)Document56 pagesAntegrade Femoral Nail (AFN)thomsoon01No ratings yet
- Pathophysiology and Genetic Factors in Moyamoya DiseaseDocument6 pagesPathophysiology and Genetic Factors in Moyamoya Diseasethomsoon01No ratings yet
- Thesis Topics in Obstetrics and Gynaecology in RguhsDocument7 pagesThesis Topics in Obstetrics and Gynaecology in Rguhsdwns3cx2100% (2)
- Chapter 12 Disorders of The Immune Response - UnlockedDocument10 pagesChapter 12 Disorders of The Immune Response - UnlockedThalia FortuneNo ratings yet
- The Smoker's BodyDocument1 pageThe Smoker's BodyAnna Rose CabuncalNo ratings yet
- QUESTION 2 Counselling AssignmentDocument7 pagesQUESTION 2 Counselling AssignmentTakudzwa GomeraNo ratings yet
- Advanced Herd Health Management, Sanitation and HygieneDocument28 pagesAdvanced Herd Health Management, Sanitation and Hygienejane entunaNo ratings yet
- Genpath - Glomerular Diseases (Primary Glomerulopathies (Nephritic) )Document5 pagesGenpath - Glomerular Diseases (Primary Glomerulopathies (Nephritic) )Julie Gemarino LumasagNo ratings yet
- Lepechoux 2020Document7 pagesLepechoux 2020Aniketh BaghoriyaNo ratings yet
- Mandalas and Wellness WheelsDocument22 pagesMandalas and Wellness WheelsnuskoNo ratings yet
- Nootropil Injection SMPC 2016 02 04Document11 pagesNootropil Injection SMPC 2016 02 04MarkusNo ratings yet
- Routes of Drug AdministrationDocument23 pagesRoutes of Drug Administrationrosalyn sugayNo ratings yet
- Lesson 1 Hand Spa TreatmentDocument22 pagesLesson 1 Hand Spa TreatmentAthena SantosNo ratings yet
- Untitled DocumentDocument4 pagesUntitled Documentclockstudy5No ratings yet
- 1-Abbreviations of Medical TermsDocument6 pages1-Abbreviations of Medical Termsyuki_teefNo ratings yet
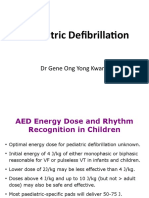
- B 04 Paediatric DefibrillationDocument10 pagesB 04 Paediatric DefibrillationIndri AbdulNo ratings yet
- Prosthetic Rehabilitation OF Maxillary Defects: A ReviewDocument12 pagesProsthetic Rehabilitation OF Maxillary Defects: A ReviewragulNo ratings yet
- Wound Bed Score and Its Correlation With Healing of Chronic WoundsDocument8 pagesWound Bed Score and Its Correlation With Healing of Chronic WoundsErick VásquezNo ratings yet
- EkggDocument44 pagesEkggLedy ErvitaNo ratings yet
- 4th Quarter Summative Test Mapeh 7Document3 pages4th Quarter Summative Test Mapeh 7Theness BonjocNo ratings yet
- Infant Star® Model 500®ventilator: SpecificationsDocument1 pageInfant Star® Model 500®ventilator: SpecificationsNando T MendozaNo ratings yet
- Pneumonia, COPD, Tuberculosis - ReportDocument23 pagesPneumonia, COPD, Tuberculosis - ReportJoceelyyn EufemianoNo ratings yet
- Indications and Contraindications For Couples TherapyDocument10 pagesIndications and Contraindications For Couples TherapyVartika jainNo ratings yet
- Anatomy of Cardio Vascular System NotesDocument16 pagesAnatomy of Cardio Vascular System NotesAgleema AhmedNo ratings yet
- Ankylosing Spondylitis (Marie-Strümpell Disease/ Bechterew's Disease)Document39 pagesAnkylosing Spondylitis (Marie-Strümpell Disease/ Bechterew's Disease)MoineeNo ratings yet
- Deaf Children With Additional Needs#1Document28 pagesDeaf Children With Additional Needs#1prppolNo ratings yet
- Moa PCMDocument32 pagesMoa PCMHinaRaviNo ratings yet
- Siwes ReportDocument58 pagesSiwes ReportMfonobong AbrahamNo ratings yet
- Bukupin Grading Perineal RupturDocument2 pagesBukupin Grading Perineal RupturWadhe Omara TobingNo ratings yet